CDC asks physicians and clinical laboratories to be on the lookout and report symptoms of hepatitis to state health departments
Growing incidences of hepatitis in children are perplexing medical professionals and researchers in several countries around the world. The mysterious outbreak is occurring in otherwise healthy children and, to date, is of unknown origin, though an adenovirus may be involved.
Microbiologists and clinical laboratory scientists who perform virology testing may want to prepare for increased numbers of children presenting with hepatitis symptoms in the US.
On April 21, the Centers for Disease Control and Prevention (CDC) issued a nationwide health alert to notify the public about a cluster of children in Alabama who presented with hepatitis and adenovirus infections. The CDC asked physicians to watch for symptoms in children and to inform local and state health departments of any new suspected cases.
Also in April, the World Health Organization (WHO) issued its own alert to an outbreak of acute hepatitis of unknown etiology among young children in several countries. In addition to the United States, cases were reported in the United Kingdom, Spain, Israel, Denmark, Ireland, the Netherlands, Italy, Norway, France, Romania, and Belgium.
All the cases reported to the WHO involved children between one month and 16 years of age with the majority of cases occurring in children under five.
According to NBC News, as of May 19, the worldwide number of cases “under investigation” had reached 600 in more than 25 countries. In the US, more than 90% of the patients required hospitalization and 14% of those patients needed a liver transplant. The CDC is investigating five pediatric deaths that may be attributed to the mysterious hepatitis outbreak.
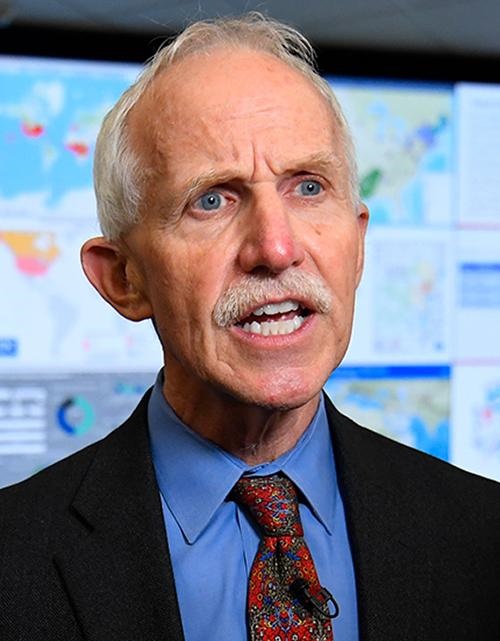
“Fifteen days ago, CDC issued a nationwide health alert to notify clinicians and public health authorities about an investigation involving nine children in Alabama identified between October of 2021 and February of 2022 with hepatitis or inflammation of the liver and adenovirus infection,” said pediatrician and epidemiologist Jay Butler, MD (above), Deputy Director for Infectious Diseases at the CDC. “We’re casting a broad net to increase our understanding,” he added. “As we learn more, we’ll share additional information and updates.” Hospital-based clinical laboratories that support emergency departments and urgent care centers with testing for hepatitis will want to monitor for upcoming CDC alerts. (Photo copyright: John Amis/AP/CNN.)
Adenovirus/SARS-CoV-2 May Be Linked to Hepatitis Outbreak
The cause of the hepatitis outbreak is as yet undetermined, but the pre-eminent theory among disease experts points to the presence of an adenovirus, which often causes cold and flu-like symptoms in addition to stomach issues.
NBC News reported that more than half of the US patients, 72% of the UK patients, and 60% of the affected patients across Europe tested positive for human adenovirus type 41. This virus, however, is generally not associated with hepatitis in healthy children, and rarely impacts the liver so severely.
Medical experts are also considering the possibility that COVID-19 infections could somehow be an underlying cause since the hepatitis outbreak occurred during the pandemic. The WHO is investigating whether exposure to the SARS-CoV-2 coronavirus might have prompted the immune systems in the infected children to react abnormally to adenoviruses that are typically non-life threatening.
“The big focus over the next week is really looking at the serological testing for previous exposure and infections with COVID,” Phillipa Easterbrook, MD, a senior scientist at the WHO headquarters in Geneva, told NBC News.
Hepatitis, or inflammation of the liver, is typically caused by heavy alcohol use, exposure to toxins, certain medical conditions and medications, or a virus.
The most recent children diagnosed with hepatitis presented with some or most of these symptoms, particularly stomach issues and fatigue. However, one symptom was present in all the children.
“The big symptom that made all of these kids different was that they all showed signs of jaundice, which is the yellowish coloration of the skin and eyes,” Markus Buchfellner, MD, a pediatric infectious disease fellow at the University of Alabama, told NBC News.
Buchfellner was the first person in the US to notice an unusual pattern of hepatitis among children. He reported his findings to the CDC last fall in 2021.
“We were able to uncover the possible association with the adenovirus 41 strain because it is our standard practice to screen patients diagnosed with hepatitis for adenovirus,” he said. “For us to dig deeper into this medical mystery and see if this strain is the cause of these severe hepatitis cases, we first need more data on how widespread the outbreak is.”
Adenovirus 41 is usually spread through fecal matter, which makes hand washing critical, especially after visits to the bathroom or diaper changes. This type of adenovirus typically presents as diarrhea, vomiting, and fever, and is often accompanied by respiratory issues.
Clinical Labs Performing Gene Sequencing Can Help
Medical scientists around the world are responding to this threat to the youngest and most vulnerable among us. Research is underway into identifying additional cases, determining what is causing the hepatitis globally among children, and establishing preventative measures.
Pathologists and clinical laboratory managers in the US will want to be on the alert for positive hepatitis tests in children whose specimens were tested at their facilities. With advances in gene sequencing that make testing economical and expeditious, more labs have the ability to not only detect hepatitis, but also to identify any genetic variants that may be associated with the increased number of pediatric hepatitis cases appearing around the world.
Clinical laboratory scientists should also know experts warn that ‘herd resistance’ is more likely than ‘herd immunity’ due to low vaccination rates in many parts of the world
Scientists estimate 73% of the US population may be immune to the SARS-CoV-2 omicron variant. Whether the nation is approaching “herd immunity” against the disease, however, remains open to debate, the Associated Press (AP) reported. These estimates are relevant to medical laboratories doing serology tests for COVID-19, as different individuals will have different immune system responses to COVID-19 infections and vaccines.
More than two years into the COVID-19 pandemic in the United States, the CDC’s COVID Data Tracker shows the number of daily cases dropped to fewer than 50,000 as of March 4, 2022, after reaching a high of 928,125 on January 3, 2022.
Meanwhile, the seven-day death rate per 100,000 people stands at 2.78. That’s significantly above the seven-day death rate reached last July of .45, but well below the 7.21 mark recorded on January 13, 2021.
“We’re clearly entering a new phase of the pandemic,” William Morice, II, MD, PhD, Department of Laboratory Medicine and Pathology at Mayo Clinic in Rochester, Minn., told KARE11, an NBC affiliate.
Is Herd Immunity Achievable?
According to the AP, an estimated 73% of the US population is likely to be immune to the Omicron variant due to vaccination or natural immunity from contracting the disease. That calculation was done for the media outlet by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in Seattle. The IHME anticipates immunity to Omicron could rise to 80% this month, as more people receive vaccination booster shots or become vaccinated.
“Herd immunity is an elusive concept and doesn’t apply to coronavirus,” he told the Associated Press (AP).
Milton maintains populations are moving toward “herd resistance,” rather than “herd immunity.” This will transform COVID-19 into a permanent fixture with seasonal outbreaks similar to influenza.
Epidemiologist, Ali Mokdad, PhD (above), Chief Strategy Officer for Population Health and Professor of Health Metrics Science at the University of Washington in Seattle, believes the US is now much better positioned to withstand the next wave of COVID-19 cases. “I am optimistic even if we have a surge in summer, cases will go up, but hospitalizations and deaths will not,” he told the Associated Press (AP). Mokdad worked on the IHME model that calculated the 73% Omicron-immunity figure for the AP. However, he recommends continued vigilance toward COVID-19. “We’ve reached a much better position for the coming months, but with waning immunity we shouldn’t take it for granted,” he added. And so, clinical laboratories can expect to continue to play a vital role in the fight against the spread of the SARS-CoV-2 coronavirus. (Photo copyright: University of Washington.)
Herd Immunity Varies, according to the WHO
Because antibodies that developed from vaccines—or natural immunity from a previous infection—diminish over time, waning protection means even those boosted or recently recovered from COVID-19 could be reinfected. In addition, vaccination rates vary widely around the world. Our World in Data estimates only 13.6% of people in low-income countries had received one dose of the COVID-19 vaccine as of March 7, 2022.
The World Health Organization (WHO) points out that herd immunity levels vary with different diseases. Herd immunity against measles requires about 95% of a population to be vaccinated, while the threshold for polio is about 80%.
“The proportion of the population that must be vaccinated against COVID-19 to begin inducing herd immunity is not known. This is an important area of research and will likely vary according to the community, the vaccine, the populations prioritized for vaccination, and other factors,” the WHO website states.
Living with COVID-19
Nonetheless, the US appears to be moving into a new “normal” phase of living with the disease.
In an interview with Reuters, US infectious disease expert Anthony Fauci, MD, Director of the National Institute of Allergy and Infectious Diseases (NIAID) acknowledged a need for returning to normal living even though portions of the population—immunocompromised individuals and the unvaccinated, including children under age five who are not eligible for vaccination—remain vulnerable to more severe COVID-19.
“The fact that the world and the United States—and particularly certain parts of the United States—are just up to here with COVID, they just really need to somehow get their life back,” Fauci said. “You don’t want to be reckless and throw everything aside, but you’ve got to start inching towards that. There’s no perfect solution to this.”
Most states have lifted coronavirus-related restrictions, including masking requirements. As COVID-19 cases drop in California, Gov. Gavin Newsom put in motion a plan called SMARTER (Shots, Masks, Awareness, Readiness, Testing, Education, and Rx) that no longer responds to COVID-19 as a crisis, but instead emphasizes prevention, surveillance, and rapid response to future variant-based surges in cases.
“We have all come to understand what was not understood at the beginning of this crisis, that there’s no ending, that there’s not a moment where we declare victory,” Newsom told USA Today.
Mayo Clinic’s Morice agrees. “It can’t be out of sight, out of mind, per se, but it at least gives us hope that we can get back to some level of normalcy here over the course of the year,” he said.
Since clinical laboratories played a critical role in assay development and COVID-19 testing, medical laboratory leaders should continue monitoring COVID-19 as it moves from pandemic to endemic status due to high vaccination rates and advances in treatment options.
The COVID-19 pandemic has raised awareness among healthcare consumers as well, about the critical role laboratory medicine plays in modern medicine and healthcare. Medical laboratory leaders and pathologists would be wise to amplify this message and stress the importance of clinical laboratory testing for many diseases and healthcare conditions.
Given the large number of mutations found in the SARS-CoV-2 Omicron variant, experts in South Africa speculate it likely evolved in someone with a compromised immune system
As the SARS-CoV-2 Omicron variant spreads around the United States and the rest of the world, infectious disease experts in South Africa have been investigating how the variant developed so many mutations. One hypothesis is that it evolved over time in the body of an immunosuppressed person, such as a cancer patient, transplant recipient, or someone with uncontrolled human immunodeficiency virus infection (HIV).
One interesting facet in the story of how the Omicron variant was being tracked as it emerged in South Africa is the role of several medical laboratories in the country that reported genetic sequences associated with Omicron. This allowed researchers in South Africa to more quickly identify the growing range of mutations found in different samples of the Omicron virus.
“Normally your immune system would kick a virus out fairly quickly, if fully functional,” Linda-Gail Bekker, PhD, of the Desmond Tutu Health Foundation (formerly the Desmond Tutu HIV Foundation) in Cape Town, South Africa, told the BBC.
“In someone where immunity is suppressed, then we see virus persisting,” she added. “And it doesn’t just sit around, it replicates. And as it replicates it undergoes potential mutations. And in somebody where immunity is suppressed that virus may be able to continue for many months—mutating as it goes.”
Multiple factors can suppress the immune system, experts say, but some are pointing to HIV as a possible culprit given the likelihood that the variant emerged in sub-Saharan Africa, which has a high population of people living with HIV.
Li “was among the first to detail extensive coronavirus mutations in an immunosuppressed patient,” the LA Times reported. “Under attack by HIV, their T cells are not providing vital support that the immune system’s B cells need to clear an infection.”
Linda-Gail Bekker, PhD (above), of the Desmond Tutu Health Foundation cautions that these findings should not further stigmatize people living with HIV. “It’s important to stress that people who are on anti-retroviral medication—that does restore their immunity,” she told the BBC. (Photo copyright: Test Positive Aware Network.)
Omicron Spreads Rapidly in the US
Genomics surveillance Data from the CDC’s SARS-CoV-2 Tracking system indicates that on Dec. 11, 2021, Omicron accounted for about 7% of the SARS-CoV-2 variants in circulation, the agency reported. But by Dec. 25, the number had jumped to nearly 60%. The data is based on sequencing of SARS-CoV-2 by the agency as well as commercial clinical laboratories and academic laboratories.
Experts have pointed to several likely factors behind the variant’s high rate of transmission. The biggest factor, NPR reported, appears to be the large number of mutations on the spike protein, which the virus uses to attach to human cells. This gives the virus an advantage in evading the body’s immune system, even in people who have been vaccinated.
“The playing field for the virus right now is quite different than it was in the early days,” Joshua Schiffer, MD, of the Fred Hutchinson Cancer Research Center, told NPR. “The majority of variants we’ve seen to date couldn’t survive in this immune environment.”
One study from Norway cited by NPR suggests that Omicron has a shorter incubation period than other variants, which would increase the transmission rate. And researchers have found that it multiplies more rapidly than the Delta variant in the upper respiratory tract, which could facilitate spread when people exhale.
Using Genomics Testing to Determine How Omicron Evolved
But how did the Omicron variant accumulate so many mutations? In a story for The Atlantic, virologist Jesse Bloom, PhD, Professor, Basic Sciences Division, at the Fred Hutchinson Cancer Research Center in Seattle, described Omicron as “a huge jump in evolution,” one that researchers expected to happen “over the span of four or five years.”
Hence the speculation that it evolved in an immunosuppressed person, perhaps due to HIV, though that’s not the only theory. Another is “that the virus infected animals of some kind, acquired lots of mutations as it spread among them, and then jumped back to people—a phenomenon known as reverse zoonosis,” New Scientist reported.
Still, experts are pointing to emergence in someone with a weakened immune system as the most likely cause. One of them, the L.A. Times reported, is Tulio de Oliveira, PhD, Affiliate Professor in the Department of Global Health at the University of Washington. Oliveira leads the Centre for Epidemic Response and Innovation at Stellenbosch University in South Africa, as well as the nation’s Network for Genomic Surveillance.
The Network for Genomic Surveillance, he told The New Yorker, consists of multiple facilities around the country. Team members noticed what he described as a “small uptick” in COVID cases in Gauteng, so on Nov. 19 they decided to step up genomic surveillance in the province. One private clinical laboratory in the network submitted “six genomes of a very mutated virus,” he said. “And, when we looked at the genomes, we got quite worried because they discovered a failure of one of the probes in the PCR testing.”
Looking at national data, the scientists saw that the same failure was on the rise in PCR (Polymerase chain reaction) tests, prompting a request for samples from other medical laboratories. “We got over a hundred samples from over thirty clinics in Gauteng, and we started genotyping, and we analyzed the mutation of the virus,” he told The New Yorker. “We linked all the data with the PCR dropout, the increase of cases in South Africa and of the positivity rate, and then we began to see it might be a very suddenly emerging variant.”
Oliveira’s team first reported the emergence of the new variant to the World Health Organization, on Nov. 24. Two days later, the WHO issued a statement that named the newly classified Omicron variant (B.1.1.529) a “SARS-CoV-2 Variant of Concern.”
Microbiologists and clinical laboratory specialists in the US should keep close watch on Omicron research coming out of South Africa. Fortunately, scientists today have tools to understand the genetic makeup of viruses that did not exist at the time of SARS 2003, Swine flu 2008/9, MERS 2013.
The ongoing study shows promise in the general development of self-powered wearable biosensors, the researchers say, in a development that has implications for clinical laboratory testing
Years back, it would be science fiction to describe a wearable garment that can not only measure an individual’s biomarkers in real-time, but also generates the power the device needs from the very specimen used for the measurement. Clinical laboratory managers and pathologists may find this new technology to be an interesting milestone on the path to wearable diagnostic devices.
With cases of diabetes on the rise across the globe, innovative ways to monitor the disease and simplify care is critical for effective diagnoses and treatment. Now, a team of researchers at Tokyo University of Science (TUS) in Japan have recently developed a diaper that detects blood glucose levels in individuals living with this debilitating illness.
Of equal interest, this glucose-testing diaper has a self-powered sensor that utilizes a biofuel cell to detect the presence of urine, measure its glucose concentration, and then wirelessly transmit that information to medical personnel and patients. The biofuel cell generates its own power directly from the urine.
Glucose in urine provides valuable data regarding blood sugar levels and can be used as an alternative to frequent blood draws to measure those levels. Monitoring the onset and progression of diabetes is crucial to making patient care easier, particularly in elderly and long-term care patients. Widespread use of these diapers in skilled nursing facilities and other healthcare settings could create an opportunity for clinical laboratories to do real-time monitoring of the blood sugar measurements and alert providers when a patient’s glucose levels indicate the need for attention.
“Besides monitoring glucose in the context of diabetes, diaper sensors can be used to remotely check for the presence of urine if you stock up on sugar as fuel in advance,” said Isao Shitanda, PhD, Associate Professor at the Department of Pure and Applied Chemistry, Faculty of Science and Technology, Tokyo University of Science, in a TUS press release. “In hospitals or nursing care sites, where potentially hundreds of diapers have to be checked periodically, the proposed device could take a great weight off the shoulders of caregivers,” he added.
Through electrochemistry, the scientists created their paper-based biofuel cell so that it could determine the amount of glucose in urine via reduction oxidation reactions, or redox for short. Using a process known as “graft polymerization,” they developed a special anode that allowed them to “anchor glucose-reactive enzymes and mediator molecules to a porous carbon layer, which served as the base conductive material,” the press release noted.
The biosensor was tested using artificial urine at different glucose levels. The energy generated from the urine then was used to power up a Bluetooth transmitter to remotely monitor the urine concentration via a smartphone. The TUS researchers determined their biofuel cell was able to detect sugar levels present in urine within one second. The diaper with its sensor could help provide reliable and easy monitoring for diabetic and pre-diabetic patients.
“We believe the concept developed in this study could become a very promising tool towards the general development of self-powered wearable biosensors,” Shitanda said in the press release.
According to the Isao Shitanda, PhD (above), lead author of the TUS study, 34.2 million people, or just over 10% of the US population, were diagnosed with diabetes in 2020. The federal Centers for Disease Control and Prevention estimates that an additional 7.3 million people have diabetes and are undiagnosed. A self-powered biosensor that detects diabetes and prediabetes in urine could help clinical laboratories and doctors catch the disease early and/or monitor its treatment. (Photo copyright: Tokyo University of Science.)
The World Health Organization (WHO) estimates that 422 million people globally were living with diabetes in 2014, and that 1.5 million deaths could be attributed directly to diabetes in 2019.
A panel of colored squares embedded on the front of the diaper changed color if specific chemical reactions fell outside normal parameters. If such a color change was observed, a smart phone application could relay that information to the baby’s doctor to determine if any further testing was needed.
Since we wrote that ebriefing in 2013, Pixie Scientific has expanded its product line to include Pixie Smart Pads, which when added to a diaper, enable’s caregivers to monitor wearers for urinary tract infections (UTI) and report findings by smartphone to their doctors.
These examples demonstrate ways in which scientists are working to combine diagnostics with existing products to help people better manage their health. Wearable electronics and biosensors are increasingly helping medical professionals and patients monitor bodily functions and chronic diseases.
As clever as these new wearable devices may be, there is still the need to monitor the diagnostic data they produce and interpret this data as appropriate to the patient’s state of health. Thus, it is likely that pathologists and clinical laboratory professionals will continue to play an important role in helping consumers and providers interpret diagnostic information collected by wearable, point-of-care testing technology.
Fear that immunity-resistant mutations of SARS-CoV-2 will emerge are real and the scientific community is paying close attention
Detection of an increasing number of new variants of the SARS-CoV-2 coronavirus raises the possibility that a new strain of COVID-19 might emerge that brings new problems to the management of the pandemic. Public health officials and clinical laboratory scientists are on the alert to determine if any new COVID-19 variant is more virulent or more easily transmissible.
Pathologists, along with the rest of the scientific community worldwide, are following reports of increasing coronavirus mutations with growing concern. The Alpha variant (Lineage B.1.1.7) accounted for most of the COVID-19 cases in April of 2021 in the US, though it was first identified in the United Kingdom. That was followed by the Iota variant (Lineage B.1.526) first identified in New York City. A series of other variants were to follow. Scientists were not surprised. It is normal for viruses to mutate, so they logged and tracked the mutations.
Then, the Delta variant (Lineage B.1.617.2) emerged during a severe outbreak in India. At first, it did not seem more threatening than any other variant, but that changed very quickly. Delta was different.
“The speed with which it dominated the pandemic has left scientists nervous about what the virus will do next. The variant battles of 2021 are part of a longer war, one that is far from over,” The Washington Post reported, which added, “Today, [Delta] has nearly wiped out all of its rivals. The coronavirus pandemic in America has become a Delta pandemic. By the end of July, it accounted for 93.4% of new infections, according to the Centers for Disease Control and Prevention.”
Why is Delta the Worst COVID-19 Variant So Far?
The Delta variant has two advantages that scientists know about:
Stickier spike protein than the spike on the original SARS-CoV-2 coronavirus, as well as on the other, earlier variants. This means that the Delta variant stands a better chance of remaining in a person’s nose or throat long enough to reproduce.
Faster replication. When a virus mutation has more opportunity to reproduce, it quickly becomes the main viral strain. This is the case with the Delta variant. Experts say that the viral load in patients with Delta is around 1,000 times higher than in patients with the original virus.
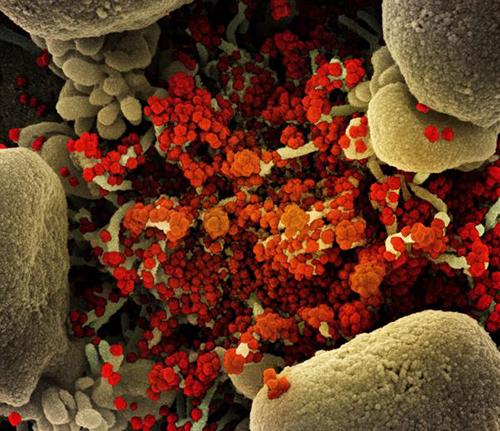
The image above is a “Colorized scanning electron micrograph of an apoptotic cell (tan) heavily infected with SARS-COV-2 virus particles (orange), isolated from a patient sample,” Newsweek reported. (Photo copyright: National Institute of Allergy and Infectious Diseases/Newsweek.)
Will More Dangerous SARS-CoV-2 Variants Appear?
“The great fear is that nature could spit out some new variant that completely saps the power of vaccines and upends the progress we’ve made against the pandemic. But to virologists and immunologists, such a possibility seems very unlikely,” STAT reported.
That is because, unlike Influenza, which is also a coronavirus, SARS-CoV-2 variants are not able to share genetic materials and recombine into deadlier variants. Thus, scientists are skeptical that a variant could appear and wipe out the progress made with vaccines and treatments.
One of the reasons the Flu vaccine changes every year is Influenza’s ability to recombine into variants that can evade immunity. Therefore, scientists are beginning to suspect that SARS-CoV-2, like the Flu, will likely be around for a while.
“I don’t think eradication is on the table. But I think we could come up with something that’s better than what we have for the flu,” Sharone Green, MD, Associate Professor of Medicine, Division of Infectious Diseases and Immunology and Infection Control Officer at University of Massachusetts Medical School, told Newsweek.
Limiting Infections and Replication
Several factors combined to create the COVID-19 pandemic. But SARS-CoV-2 was a novel coronavirus, meaning it was a new pathogen of a known virus. This meant every person on the planet was a potential host.
The situation now is different. Thanks to natural immunity, vaccines, and treatments that shorten the infection, the SARS-CoV-2 coronavirus has less chance to replicate.
“The pressure is there, but the opportunity is not. The virus has to replicate in order to mutate, but each virus doesn’t get many lottery tickets in a vaccinated person who’s infected,” Jeremy Kamil, PhD, Associate Professor of Microbiology and Immunology at LSU Health in Shreveport, La., told STAT.
Tracking Variants of Interest and Variants of Concern
The World Health Organization (WHO) has been monitoring the viral evolution of SARS-CoV-2 since the beginning of the pandemic. In late 2020, the WHO created categories for tracking variants:
VOIs are “A variant with specific genetic markers that have been associated with changes to receptor binding, reduced neutralization by antibodies generated against previous infection or vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease severity.”
Current VOIs include:
Eta (Lineage B.1.525), detected in multiple countries, designated a VOI in March 2021.
Iota (Lineage B.1.526), US, first detected in November 2020, designated a VOI in March 2021.
Lambda (lineage C.37), Peru, first detected in December 2020, designated a VOI in June 2021.
VOCs, on the other hand, demonstrate all the characteristics of VOIs and also demonstrate “an increase in transmissibility, more severe disease (e.g., increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures.”
Current VOCs include:
Alpha (lineage B.1.1.7), first detected in the UK, September 2020.
Delta (lineage B.1.617.2), first detected in India, October 2020.
Will Vaccines Stop Working?
With each new variant, there tends to be a flurry of media attention and fearmongering. That a variant could emerge which would render our current vaccines ineffective has the scientific community’s attention.
“There is intense interest in whether mutations in the spike glycoprotein mediate escape from host antibodies and could potentially compromise vaccine effectiveness, since spike is the major viral antigen in the current vaccines,” wrote Adam S. Lauring, MD, PhD, and Emma B. Hodcroft, PhD, in “Genetic Variants of SARS-CoV-2—What Do They Mean?” published in the Journal of the American Medical Association (JAMA).
“Because current vaccines provoke an immune response to the entire spike protein, it is hoped that effective protection may still occur despite a few changes at antigenic sites in SARS-CoV-2 variants,” they added.
Future events may justify the optimism that the ongoing effectiveness of vaccines will help with many COVID-19 variants. But pathologists and clinical laboratory leaders may want to be vigilant, because as infection rates increase, so do workloads and demands on critical resources in their medical laboratories.