Advancements in genetic sequencing continue to enable microbiologists and genetic scientists to explore the origins and mutations of deadly diseases
Microbiologists and researchers can now study the gene sequence of 5,000-year-old bubonic plague bacteria. The scientific team that achieved this feat of gene sequencing believes this is the oldest case of the ancient strain of the plague found to date.
For microbiologists, this demonstrates how advances in gene sequencing technologies are allowing scientists to go further back in time to look at how the genomes of bacteria and viruses have evolved and mutated. This helps science understand the process of genetic mutation, as well as learning which mutations survived because they could more easily infect humans.
Missing Gene has ‘Dramatic Influence on Virulence’ of Plague
To conduct their study, the researchers sequenced the genomes of samples from the teeth and bones of four hunter-gatherers and tested the remains for bacterial and viral pathogens. They found evidence of Yersinia pestis (Y. pestis) in the dental remains of a 20- to 30-year-old male dubbed RV 2039.
The jaw bones used for the research were discovered in the late 1800s in the Rinnukalns, a stone age settlement unearthed in present-day Republic of Latvia in the late 19th century.
Missing Genetic Element in Ancient Bacterium
The scientists were surprised to find evidence of Y. pestis in the remains and noted that the analysis of the microbe lacked a crucial genetic element observed in later strains of the bacteria. Missing was the gene that allows biting fleas to act as vectors to spread the plague to humans.
“What’s so surprising is that we see already in this early strain more or less the complete genetic set of Y. pestis, and only a few genes are lacking,” said biochemist and archeologist Ben Krause-Kyora, Professor and head of the Ancient DNA (aDNA) Laboratory at the University of Kiel in Germany, and one of the authors of the study, in a press release.
“But even a small shift in genetic settings can have a dramatic influence on virulence,” he added.
This absent gene also is responsible for creating the pus-filled buboes associated with the Black Death (bubonic plague) that occurred in the 1300s. The Black Death killed 75 million to 200 million people worldwide, mostly in Eurasia and North Africa. It is to date the most fatal pandemic recorded in human history.
“Different pathogens and the human genome have always evolved together,” said Professor Ben Krause-Kyora (above left with and Steve Zäuner at center and Dr. Silvia Codreanu-Windauer at right), in the press release. “We know Y. pestis most likely killed half of the European population in a short time frame, so it should have a big impact on the human genome. But even before that, we see major turnover in our immune genes at the end of the Neolithic Age, and it could be that we were seeing a significant change in the pathogen landscape at that time as well,” he added. (Photo copyright: Mittelbayerische.)
A Less Lethal Bubonic Plague?
Although RV 2039 most likely perished from the bubonic plague, the researchers believe his strain of the infection was more mild, less contagious, and not as lethal as the later genetic mutations of the bacteria that caused the Black Death pandemic. The researchers concluded that the man most likely contracted the disease through a bite from an infected rodent or other animal, the press release notes.
“Isolated cases of transmission from animals to people could explain the different social environments where these ancient diseased humans are discovered,” Krause-Kyora said in the press release. “We see it in societies that are herders in the steppe, hunter-gatherers who are fishing, and in farmer communities—totally different social settings but always spontaneous occurrence of Y. pestis cases.”
From Animal Bite to Flea Infection in 7,000 Years’ Worth of Mutations
The Y. pestis bacteria that infected RV 2039, the researchers surmised, most likely split from its predecessor, Yersinia pseudotuberculosis, which first appeared on Earth about 7,000 years ago. It most likely took Y. pestis over a thousand years to acquire all the mutations necessary for flea-based transmission of the bacteria to humans, the researchers noted.
“What’s most astonishing is that we can push back the appearance of Y. pestis 2,000 years farther than previously published studies suggested,” Krause-Kyora said. “It seems that we are really close to the origin of the bacteria.”
It is unknown how many cases still occur worldwide due to unreliable diagnoses and poor reporting in developing countries. However, data from the World Health Organization (WHO) states that there were 3,248 cases of plague reported worldwide between 2010 and 2015, including 584 deaths. Currently, the three most endemic countries for plague are the Democratic Republic of the Congo, Madagascar, and Peru.
The researchers’ findings illustrate how advances in gene sequencing technologies are helping microbiologists, virologists, and genetic scientists understand the affect mutations have on diseases that have plagued humans since the beginning of humanity itself.
Will this lead to new genomic diagnostics? Perhaps. The research is worth watching.
The study ‘shows that measurement using a urine test provides improved accuracy relative to other measurement methods, for example certain kinds of blood tests,’ a KI news release states
Researchers at the Karolinska Institute (KI) in Sweden have developed a non-invasive urine-based test that can identify what type of asthma a patient has and its severity. If developed into a clinical laboratory diagnostic, such a test also could give clinicians a better idea of what treatment is more likely to be effective—a core goal of precision medicine.
Another benefit of this methodology is that it is a non-invasive test. Should further studies conclude that this urine-based test produces accurate results acceptable for clinical settings, medical laboratories would certainly be interested in offering this assay, particularly for use in pediatric patients who are uncomfortable with the venipunctures needed to collect blood specimens. Also, given the incidence of asthma in the United States, there is the potential for a urine-based asthma test to generate a substantial number of test requests.
The objective of the study, according to the Karolinska Institute researchers, was “To test if urinary eicosanoid metabolites can direct asthma phenotyping.” The team used mass spectrometry to measured certain lipid biomarkers (prostaglandins and leukotrienes), which are known to play a key role in the inflammation that occurs during asthma attacks.
According to a KI news release, “The study is based on data from the U-BIOPRED study (Unbiased BIOmarkers in PREDiction of respiratory disease outcomes), which was designed to investigate severe asthma. The study included 400 participants with severe asthma, which often requires treatment with corticosteroid tablets, nearly 100 individuals with milder forms of asthma, and 100 healthy control participants.”
“We discovered particularly high levels of the metabolites of the mast cell mediator prostaglandin D2 and the eosinophil product leukotriene C4 in asthma patients with what is referred to as Type 2 inflammation. Using our methodology, we were able to measure these metabolites with high accuracy and link their levels to the severity and type of asthma,” said Johan Kolmert, PhD (above), a post-doctoral researcher at the Institute of Environmental Medicine, Karolina Institute, and first author of the study, in the KI news release. If perfected, such accuracy could lead to effective precision medicine clinical laboratory tests. (Photo copyright: Karolinska Institute.)
More Accurate Testing Could Lead to Biomarker-guided Precision Medicine
In the US alone, 25,131,132 people currently suffer from asthma, about five million of which are children under the age of 18, according to 2019 CDC statistics. The World Health Organization (WHO) reports that worldwide, “Asthma affected an estimated 262 million people in 2019 and caused 461,000 deaths.”
People with mild asthma may have good success using steroid inhalers. However, for those with moderate to severe asthma where inhalers are not effective, oral corticosteroids may also be necessary. But corticosteroids have been associated with high blood pressure and diabetes, among other negative side effects.
“To replace corticosteroid tablets, in recent times several biological medicines have been introduced to treat patients with Type 2 inflammation characterized by increased activation of mast cells and eosinophils,” said Sven-Erik Dahlén, Professor at the Institute of Environmental Medicine, Karolinska Institute, in the news release.
Currently, there are no simple tests that show what type of asthma a patient has. Instead, clinicians rely on lung function tests, patient interviews, allergy tests, and blood tests.
Earlier this year, researchers at Brigham and Women’s Hospital and Exosome Diagnostics in Massachusetts investigated a non-invasive, urine-based test for transplant rejection. According to a news release, “Patients can spend up to six years waiting for a kidney transplant. Even when they do receive a transplant, up to 20% of patients will experience rejection.”
“If rejection is not treated, it can lead to scarring and complete kidney failure. Because of these problems, recipients can face life-long challenges,” said Jamil Azzi, MD, Director of the Kidney Transplantation Fellowship Program at Brigham and Women’s Hospital, and Associate Professor of Medicine at Harvard School of Medicine. “Our goal is to develop better tools to monitor patients without performing unnecessary biopsies. We try to detect rejection early, so we can treat it before scarring develops,” he said.
Detecting Bladder Cancer with Urine Testing
Another condition where urine tests are being investigated is bladder cancer. An article in Trends in Urology and Men’s Health states, “Several point-of-care urine tests have been developed to help identify patients who may be at higher risk of bladder cancer.” Those tests could have the potential for use in primary care, which could mean fewer people would need invasive, painful, and risk-carrying cystoscopies.
“New tests to help identify hematuria patients who are at a higher risk of cancer would help to improve the diagnostic pathway, reduce the number diagnosed by emergency presentation, lessen the burden on urology services, and spare those who do not have cancer an invasive and costly examination, such as cystoscopy,” the article’s authors wrote.
These urine-based tests are still under investigation by various research teams and more research is needed before clinical trials can be conducted and the tests can be submitted for regulatory approval. Though still in the early stages of development, urine-based diagnostic testing represents far less invasive, and therefore safer, ways to identify and treat various diseases.
Studies into how the elements in urine might be used as biomarkers for clinical laboratory tests may lead to improved non-invasive precision medicine diagnostics that could save many lives.
Four International Pandemics That Occurred Prior to COVID-19 and Contributed to Increased Clinical Laboratory Testing to Aid in Managing the Outbreaks
Since 1900, millions have died worldwide from previous viruses that were as deadly as SARS-CoV-2. But how much do pathologists and clinical laboratory scientists know about them?
SARS-CoV-2 continues to infect populations worldwide. As of May 28, 2021, the World Health Organization (WHO) reported that 168,599,045 people have been diagnosed with COVID-19 infections globally, and 3,507,377 individuals have perished from the coronavirus.
At the same time, federal Centers for Disease Control and Prevention (CDC) statistics show there have been 33,018,965 cases of COVID-19 in the United States, 589,547 of which resulted in death.
But COVID-19 is just the latest in a string of pandemics that spread across the planet in the past century. Since 1900, there have been four major international pandemics resulting in millions of deaths. But how many people even remember them? And how many pathologists, microbiologists, and clinical laboratory scientists working today experienced even the most recent of these four global pandemics?
Here is a summary/review of these major pandemics to give clinical laboratory professionals context for comparing the COVID-19 pandemic to past pandemics.
Spanish Flu of 1918
The 1918 influenza pandemic, commonly referred to as the Spanish Flu, was the most severe and deadliest pandemic of the 20th century. This pandemic was caused by a novel strand of the H1N1 virus that had avian origins. It is estimated that approximately one third of the world’s population (at that time) became infected with the virus.
According to a CDC article, the flu pandemic of 1918 was responsible for at least 50 million deaths worldwide, with about 675,000 of those deaths occurring in the United States. This pandemic had an unusually high death rate among healthy individuals between the ages of 15 and 34 and actually lowered the average life expectancy in the United States by more than 12 years, according to a CDC report, titled, “The Deadliest Flu: The Complete Story of the Discovery and Reconstruction of the 1918 Pandemic Virus.”
Interestingly, experts feel the 1918 flu strain never fully left us, but simply weakened and became less lethal as it mutated and passed through humans and other animals.
“All those pandemics that have happened since—1957, 1968, 2009—all those pandemics are derivatives of the 1918 flu,” he told The Washington Post. “The flu viruses that people get this year, or last year, are all still directly related to the 1918 ancestor.”
1957 Asian Flu
The H2N2 virus, which caused the Asian Flu, first emerged in East Asia in February 1957 and quickly spread to other countries throughout Asia. The virus reached the shores of the US by the summer of 1957, where the number of infections continued to rise, especially among the elderly, children, and pregnant women.
Between 1957-1958, the Asian Flu spread across the planet causing between one to two million deaths, including 116,000 deaths in the US alone. However, this pandemic could have been much worse were it not for the efforts of microbiologist and vaccinologist Maurice Hilleman, PhD, who in 1958 was Chief of the Department of Virus Diseases at Walter Reed Army Medical Center.
Concerned that the Asian flu would wreak havoc on the US, Hilleman—who today is considered the father of modern vaccines—researched and created a vaccine for it in four months. Public health experts estimated the number of US deaths could have reached over one million without the fast arrival of the vaccine, noted Scientific American, adding that though Hilleman “is little remembered today, he also helped develop nine of the 14 children’s vaccines that are now recommended.”
During his lifetime, Maurice Hilleman, PhD (above), developed a staggering 40 vaccines to help prevent everything from measles, mumps, rubella, pneumonia, meningitis, hepatitis A and B, and other infectious diseases. (Photo copyright: Scientific American.)
1968 Hong Kong Flu
The 1968 influenza pandemic known as the Hong Kong flu emerged in China and persisted for several years. Within weeks of its emergence in the heavily populated Hong Kong, the flu had infected more than 500,000 people. Within months, the highly contagious virus had gone global.
According to the Encyclopedia Britannica, this pandemic was initiated by the influenza A subtype H3N2 virus and is suspected to have evolved from the viral strain that caused the 1957 flu pandemic through a process called antigenic shift. In this case, the hemagglutinin (H) antigen located on the outer surface of the virus underwent a genetic mutation to manufacture the new H3 antigen. Persons who had been exposed to the 1957 flu virus seemed to retain immune protection against the 1968 virus, which, Britannica noted, could help explain the relative mildness of the 1968 outbreak.
It is estimated that the 1968 Hong Kong Flu killed one to four million people worldwide, with approximately 100,000 of those deaths occurring in the US. A vaccine for the virus was available by the end of 1968 and the outbreaks appeared to be under control the following year. The H3N2 virus continues to circulate worldwide as a seasonal influenza A virus.
2009 H1N1 Swine Flu
In the spring of 2009, the novel H1N1 influenza virus that caused the Swine Flu pandemic was first detected in California. It soon spread across the US and the world. This new H1N1 virus contained a unique combination of influenza genes not previously identified in animals or people. By the time the World Health Organization (WHO) declared this flu to be a pandemic in June of 2009, a total of 74 countries and territories had reported confirmed cases of the disease. The CDC estimated there were 60.8 million cases of Swine Flu infections in the US between April 2009 and April 2010 that resulted in approximately 274,304 hospitalizations and 12,469 deaths.
This pandemic primarily affected children and young and middle-aged adults and was less severe than previous pandemics. Nevertheless, the H1N1 pandemic dramatically increased clinical laboratory test volumes, as Dark Daily’s sister publication, The Dark Report, covered in “Influenza A/H1N1 Outbreak Offers Lessons for Labs,” TDR June 8, 2009.
“Laboratories in the United States experienced a phenomenal surge in specimen volume during the first few weeks of the outbreak of A/H1N1. This event shows that the capacity in our nation’s public health system for large amounts of testing is inadequate,” Steven B. Kleiboeker, DVM, PhD, told The Dark Report. At that time Kleiboeker was Chief Scientific Officer and a Vice-President of ViraCor Laboratories in Lee’s Summit, Mo.
1.7 Million ‘Undiscovered’ Viruses
As people travel more frequently between countries, it is unlikely that COVID-19 will be the last pandemic that we encounter. According to the World Economic Forum (WEF), there are 1.7 million “undiscovered” viruses that exist in mammals and birds and approximately 827,000 of those viruses have the ability to infect humans.
Thus, it remains the job of pathologists and clinical laboratories worldwide to remain ever vigilant and prepared for the next global pandemic.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
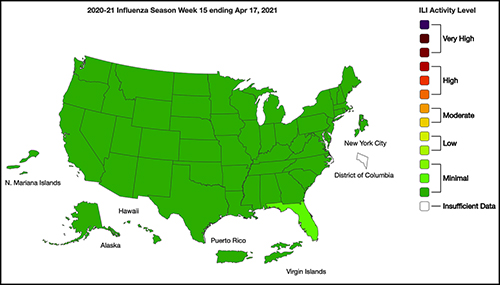
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
Royal College of Pathologists of Australia says the pandemic is ‘suppressed’ to ‘intermittent’ outbreaks, thanks to the dedication of thousands of pathologists, medical scientists, and laboratory professionals
COVID-19 efforts in Australia have achieved a milestone. Pathology laboratories there have performed more than 12 million SARS-CoV-2 tests since the pandemic began. That is an impressive feat and is equal to about half the country’s population of 25.4 million people.
“It is an incredible feat,” they continued. “Australia’s current position of having effectively suppressed the virus to intermittent outbreaks owes much to the year-long dedication and ingenuity of 35,000 pathologists, medical scientists, lab technicians, couriers, phlebotomists, and ancillary personnel.”
Australia Pathology Society Recognizes Accomplishments
Furthermore, Graves and Bott wrote, pathology in Australia deserves recognition for these pandemic-related accomplishments, among others, as well:
Australia launched drive-through COVID-19 testing clinics even before the pandemic was declared by the World Health Organization (WHO).
An RCPA quality assurance program for lab COVID-19 testing was the first of its kind to start worldwide, and it became a model for other countries.
Australia’s pathology labs were fast to develop in-house test kits once they had the genome sequence for the SARS-CoV-2 coronavirus.
Quick Responses to COVID-19 in the Land Down Under
The Doherty Institute (a joint venture of the University of Melbourne and the Royal Melbourne Hospital) offers research, teaching, public health and reference lab services, diagnostics, and clinical care for infectious diseases and immunity.
After receiving the patient sample on Jan. 24, 2020, institute scientists were the first outside China to grow the coronavirus in cell culture, noted a University of Melbourne news release.
“We’ve planned for an incident like this for many, many years, and that’s really why we were able to get an answer so quickly,” Dr. Mike Catton (above), Co-Deputy Director, Doherty Institute and Director of the Victorian Infectious Diseases Reference Laboratory (VIDRL), said in the news release. (Photo copyright: ABC News.)
Doherty Institute researchers also were first to report on immune response to COVID-19, according to a second news release.
“When COVID-19 emerged, we already had ethics and protocols in place so we could rapidly start looking at the virus and immune system in great deal,” Dr. Irani Thevarajan, Infectious Disease Physician, Doherty Institute, Royal Melbourne Hospital, said in the second news release.
“Our study provides novel contributions to the understanding and kinetics of immune responses during a non-severe case of COVID-19. This patient did not experience complications of respiratory failure or acute respiratory distress syndrome, did not require supplemental oxygenation, and was discharged within a week of hospitalization, consistent with non-severe but symptomatic disease,” Thevarajan and co-authors wrote in Nature Medicine.
Drive-Through COVID-19 Testing Sites in Australia
Also impressive was Australia’s launch of drive-through COVID-19 testing on March 9, 2020, before the pandemic was declared by WHO on March 11.
The COVID-19 testing site in Adelaide, South Australia, was “believed to be a first for the country’s public health system,” ABC News reported.
Public Recognition for Medical Laboratories has Global Reach
The COVID-19 response and scientific contributions by pathology laboratory scientists and researchers in Australia are noteworthy. It is also significant that Australia’s pathology professional society sought recognition for medical laboratory workers by detailing their accomplishments during the pandemic and sharing them in media with national and global reach.