Scientists reported positive Phase 1 trial results of their “intratumoral microdevice” in patients with glioma tumors
Here is an example of new microtechnology which has the potential to greatly shorten the time and improve the ability of physicians to determine which anti-cancer drug is most effective for an individual patient’s glioblastoma. As it is further developed, this technology could give anatomic pathologists and clinical laboratories an increased role in assessing the data produced by microdevices and helping physicians determine the most appropriate anti-cancer drug for specific patients.
In a news release, researchers at Brigham and Women’s Hospital (BWH) in Boston said they have developed an implantable “intratumoral microdevice” (IMD) that functions as a “lab in a patient,” capable of gauging the effectiveness of multiple drugs that target brain tumors. In a Phase 1 clinical trial, they tested the IMD on six patients with glioma tumors.
“In order to make the greatest impact on how we treat these tumors, we need to be able to understand, early on, which drug works best for any given patient,” study co-author Pier Paolo Peruzzi, MD, PhD, told the Harvard Gazette. “The problem is that the tools that are currently available to answer this question are just not good enough. So, we came up with the idea of making each patient their own lab, by using a device which can directly interrogate the living tumor and give us the information that we need.”
Peruzzi is Principal Investigator at the Harvey Cushing Neuro-Oncology Laboratories and Assistant Professor of Neurosurgery at Harvard Medical School.
“Our goal is for the placement of these devices to become an integral part of tumor surgery,” said Pier Paolo Peruzzi, MD PhD (above) of Brigham and Women’s Hospital and Harvard Medical School in an article he co-wrote for Healio. “Then, with the data that we have from these microdevices, we can choose the best systemic chemotherapy to give to that patient.” Pathologists and clinical laboratories may soon play a role in helping doctors interpret data gathered by implantable microdevices and choose the best therapies for their patients. (Photo copyright: Dana-Farber Cancer Institute.)
New Perspective on Tumor Treatments
In a news story he co-wrote for Healio, Peruzzi explained that the microdevice—about the size and shape of a grain of rice—contains up to 30 tiny reservoirs that the researchers fill with the drugs they want to test. Surgeons implant the device during a procedure to remove the tumors.
The surgery takes two to three hours to perform, and during that time, the device releases “nanodoses” of the drugs into confined areas of the tumor. Near the end of the procedure, the device is removed along with tissue specimens. The researchers can then analyze the tissue to determine the effectiveness of each drug.
“This is not in the lab, and not in a petri dish,” Peruzzi told Harvard Gazette. “It’s actually in real patients in real time, which gives us a whole new perspective on how these tumors respond to treatment.”
The Healio story notes that gliomas are “among the deadliest brain cancers and are notoriously difficult to treat.” With current approaches, testing different therapies has posed a challenge, Peruzzi wrote.
“Right now, the only way these drugs are tested in patients is through what are called window-of-opportunity studies, where we give one drug to the patient before we resect the tumor and analyze the effect of the drug,” he said. “We can only do this with one drug at a time.”
Determining Safety of Procedure
The primary goal of the Phase 1 trial was to determine the safety of the procedure, Peruzzi noted. “To be in compliance with standard clinical practice and minimize risks to the patients, we needed to integrate the placement and retrieval of the device during an otherwise standard operation.”
The trial consisted of three men and three women ranging from 27 to 86 years old, with a median age of 76. Five were diagnosed with glioblastoma and one with grade 4 astrocytoma.
“None of the six enrolled patients experienced adverse events related to the IMD, and the exposed tissue was usable for downstream analysis for 11 out of 12 retrieved specimens,” the researchers wrote in Science Translational Medicine. They noted that application of the IMD added about 32 minutes to the time required for the surgery, equating to a cost increase of $7,800.
One drug they tested was temozolomide (TMZ), “the most widely used agent in this patient population,” they wrote. “Several patients in our trial received it systemically, either before or after IMD insertion, as part of the standard of care. Thus, although our trial was not designed to choose chemotherapy agents based on IMD data, we still could compare the observed clinical-radiological response to systemic TMZ with the patient-specific response to TMZ in the IMD-exposed tissue.”
One patient, the researchers noted, had not benefited from the drug “in concordance with the poor tissue response observed in the IMD analysis.” But in another patient, a 72-year-old woman, “IMD analysis showed a marked response to TMZ,” and she survived for 20 months after receiving the treatment “with radiological evidence of tumor response. This was despite having a subtotal tumor resection, in itself an unfavorable prognostic factor. The patient expired because of an unrelated cardiovascular event, although she had remained neurologically stable.”
Drug Duration Limitation
One limitation of the study was that testing the device during the tumor removal procedure limited the duration of the drug treatments, Peruzzi said. The Harvard Gazette noted that following their initial study, the researchers were testing a variation of the procedure in which the device is implanted three days before the main surgery in a minimally invasive technique. This gives the drugs more time to work.
Cancer researchers have theorized that common treatments for tumors can impair the immune system, Peruzzi wrote in Healio. “One thing we want to look at is which drugs can kill the tumor without killing the immune system as well,” he noted.
Future studies will determine the effectiveness of implanting microdevices into tumors to test therapies in vivo. Should they become viable, clinical laboratories and anatomic pathologists will likely be involved in receiving, interpreting, storing, and transmitting the data gathered by these devices to the patient’s doctors.
Survey respondents can give their opinions about the proposed VALID and VITAL acts
Two bills are pending in Congress, and each is written to change the current regulatory scheme for laboratory-developed tests (LDTs) and in vitro clinical tests (IVCTs). The bills go by the acronyms of the VALID Act and VITAL Act. Many clinical laboratories offering LDTs today may be unaware of the details within each bill as currently written.
That existing regulatory arrangement will change if one of the two pending bills in Congress were to pass and be signed into law. That proposal is known as the Verifying Accurate Leading-Edge IVCT Development Act, or VALID Act. It is a bipartisan, 245-page bill that proposes FDA oversight of LDTs and is making its way through both the Senate and the House of Representatives.
A smaller, seven-page counterproposal is also before the Senate called the Verified Innovative Testing in American Laboratories Act, or VITAL Act. The VITAL Act would keep LDTs under CLIA but mandate updates to CLIA’s rules to account for modern tests.
Readers: Are you in favor of more or less regulation of LDTs? Take this quick survey and let us know what you think. Dark Daily wants to know your thoughts about LDT oversight. Click here to take our six-question survey. Results of this survey will be reported in a coming Dark Daily e-briefing.
Alert pathologists and clinical laboratory managers know that behind every bill proposed in Congress is a party with a vested interest that brought the issue to a senator or representative. Once enacted into law, a new bill changes the status quo, generally to the benefit of the private interests that requested that bill. This is true of both the VALID Act and the VITAL Act.
The table at the bottom of this briefing compares the provisions of each act and is current as of March 28.
Who Opposes VALID Act?
The VALID Act is garnering more attention than the VITAL Act.
On March 22, the American Association for Clinical Chemistry (AACC) sent out an email message urging its members to oppose the VALID Act.
“Let your legislators know that that if VALID becomes law, your institution and other hospitals and small commercial laboratories could be forced to stop providing LDTs,” wrote Patricia Jones, PhD, DABCC, FACB, Chair of AACC’s Policy and External Affairs Core Committee. The AACC has long criticized the VALID Act..
On the other side of the debate, Philadelphia-based The Pew Charitable Trusts, a nonprofit that in part analyzes publics policy, has come out in support of the VALID Act’s proposed requirements.
Two bills are pending in Congress about the future of LDT regulation.
“Although the [current] LDT regulatory process offers labs significant flexibility and enables a more rapid response to public health needs when no FDA-cleared or -approved test exists, the relative lack of oversight for LDTs puts the health of patients at risk,” Pew wrote in an October 2021 report on LDTs.
The Advanced Medical Technology Association also supports the VALID Act, as do many manufacturers of in vitro test kits and large commercial labs. Proponents also believe FDA regulation is needed for IVCTs because they are similar to medical devices and bring with them patient safety concerns.
The American Clinical Laboratory Association and the National Independent Laboratory Association (NILA) have not taken formal positions on the VALID Act.
Congress Could Roll VALID Act into MDUFA Vote to Win Passage
There may be an effort to attach the VALID Act to the authorization vote for the Medical Device User Fee Agreement V (MDUFA), according to a February health legislation alert from law firm Akin Gump Strauss Hauer & Feld based in Washington.
MDUFA funding provides resources to the FDA’s medical device review program. Congress is set to receive final MDUFA V recommendations in April.
Nineteen healthcare and lab industry groups, including the American Medical Association, AACC, AMP, and NILA, sent a joint letter to four Congress members on Feb. 23 requesting they deliberate the VALID Act separately and not as part of MDUFA.
Again, please complete this survey and tell us what you think about FDA regulation of LDTs, as defined in the VALID Act, compared to continuing LDT oversight via a modernized CLIA in the VITAL Act.
—Scott Wallask
Comparison of VALID Act and VITAL Act
VALID Act
VITAL Act
Full act name
Verifying Accurate Leading-Edge IVCT Development Act
Verified Innovative Testing in American Laboratories Act
Bill numbers
House Bill H.R.4128 Senate Bill S.2209
Senate Bill S.1666
Sponsors
Sen. Michael Bennet (D-CO) , Sen. Mike Braun (R-IN), Rep. Larry Bucshon, MD (R-IN), Sen. Richard Burr (R-NC), and Rep. Diana DeGette (D-CO)
Sen. Rand Paul (R-KY)
Provisions
Developers shall apply for premarket approval of IVCTs if there is insufficient evidence of analytical validity or clinical validity or if it’s reasonably possible an IVCT will cause serious adverse health effects.
Applications shall include a summary of test data and scientific evidence to support analytical and clinical validity of the test.
Through a technology certification, developers can submit an IVCT to the FDA for review, and if granted, the certification allows them to develop similar tests without going back for review each time.
The FDA must establish a program for rapid review of breakthrough IVCTs that provide effective treatment of life-threatening diseases
The federal government should work to ensure that regulatory oversight of laboratory tests does not limit patient access, impede innovation, or limit a test’s sustainability as a result of being unduly burdensome or beyond the fiscal capacity of the laboratory to reasonably validate and perform.
No aspects of LTDs shall be regulated under the FDA.
No later than 180 days after enactment of the bill, the secretary of health and human services shall report to the Senate’s Committee on Health, Education, Labor, and Pensions about recommendations to update clinical lab regulations and provide an assessment of LDT use during the 2020 pandemic response.
Exemptions
IVCTs being marketed before the VALID Act goes into effect
Low-risk tests
IVCTs that are granted emergency use
No new exemptions
Review timelines
The FDA shall make a decision no later than 90 days after an application is submitted.
No new requirements noted.
Sources: VALID Act and VITAL Act bills. Information is current as of March 28, 2022.
Decision is part of UK effort to diagnose 75% of all cancers at stage I or stage II by 2028 and demonstrates to pathologists that the technology used in liquid biopsy tests is improving at a fast pace
Pathologists and medical laboratory scientists know that when it comes to liquid biopsy tests to detect cancer, there is plenty of both hope and hype. Nevertheless, following a successful pilot study at the Christie NHS Foundation Trust in Manchester, England, which ran from 2015-2021, the UK’s National Health Service (NHS) is pushing forward with the use of liquid biopsy tests for certain cancer patients, The Guardian reported.
NHS’ decision to roll out the widespread use of liquid biopsies—a screening tool used to search for cancer cells or pieces of DNA from tumor cells in a blood sample—across the UK is a hopeful sign that ongoing improvements in this diagnostic technology are reaching a point where it may be consistently reliable when used in clinical settings.
The national program provides personalized drug therapies based on the genetic markers found in the blood tests of cancer patients who have solid tumors and are otherwise out of treatment options. The liquid biopsy creates, in essence, a match-making service for patients and clinical trials.
Liquid Biopsy Genetic Testing for Cancer Patients
“The learnings from our original ‘Target’ study in Manchester were that genetic testing needs to be done on a large scale to identify rare genetic mutations and that broader access to medicines through clinical trials being undertaken across the country rather than just one site are required,” Matthew Krebs, PhD, Clinical Senior Lecturer in Experimental Cancer Medicine at the University of Manchester, told The Guardian.
Krebs, an honorary consultant in medical oncology at the Christie NHS Foundation Trust, led the Target National pilot study.
“This study will allow thousands of cancer patients in the UK to access genetic testing via a liquid biopsy. This will enable us to identify rare genetic mutations that in some patients could mean access to life-changing experimental medicines that can provide great treatment responses, where there are otherwise limited or no other treatment options available.”
Detecting cancers at earlier stages of disease—when treatment is more likely to result in improved survival—has become a strategic cancer planning priority in the UK, theBMJ noted.
“The NHS is committed to diagnosing 75% of all cancers at stage I or II by 2028, from around 50% currently,” the BMJ wrote. “Achieving such progress in less than a decade would be highly ambitious, even without disruption caused by the COVID-19 pandemic. In this context, considerable hope has been expressed that blood tests for circulating free DNA—sometimes known as liquid biopsy—could help achieve earlier detection of cancers.”
The Guardian noted that the UK’s initiative will use a liquid biopsy test made by Swiss-healthcare giant Roche.
“We can’t guarantee that we will find a fault in the genetic code of every cancer patient we recruit, or that if we do, there will be a suitable drug trial for them,” Matthew Krebs, PhD (above), lead scientist of the NHS’ Target National pilot study, told The Guardian. “However, as we learn more about the genetics of cancer in this study, it will help doctors and scientists develop new treatments to help people in the future. Ultimately, we hope liquid biopsy testing will be adopted into routine NHS care, but we need studies such as this to show the benefit of the test on a large scale and provide the evidence that patients can benefit from being matched to targeted medicines on the basis of the blood test.” (Photo copyright: Cancer Research UK Manchester Centre.)
In her article “The Promise of Liquid Biopsies for Cancer Diagnosis,” published in the American Journal of Managed Care (AJMC) Evidence-based Oncology, serial healthcare entrepreneur and faculty lecturer at Harvard Medical School Liz Kwo, MD, detailed the optimism surrounding the “revolutionary screening tool,” including its potential for:
identifying mechanisms of resistance to therapies,
measuring remaining disease after treatment,
assessing cancer relapse or resistance to treatment, and
eliminating risk surrounding traditional biopsies.
The AJMC article estimated the liquid biopsy market will be valued at $6 billion by 2030. However, Kwo also noted that clinical adoption of liquid biopsies in the US continues to face challenges.
Welch compared the investor hype surrounding liquid biopsies to that of the now-defunct blood testing company Theranos, which lured high-profile investors to pour millions into its unproven diagnostic technology.
“Effective cancer screening requires more than early detection. It also requires that starting therapy earlier helps people live to older ages than they would if they started treatment later,” he wrote. “If that doesn’t happen, liquid biopsies will only lead to people living longer with the knowledge they have a potentially incurable disease without extending their lives. These people would be subjected to cancer therapies and their toxicities earlier, but at a time when they would otherwise be experiencing no cancer-related signs or symptoms.”
And so, while there’s much excitement about the possibility of a minimally invasive way to detect cancer, anatomic pathology groups and clinical laboratories will have to wait and see if the hype and hope surrounding liquid biopsies is substantiated by further research.
Proof of vaccination, masking, and availability of on-site testing will continue to be measures taken at in-person events for pathologists and medical laboratory professionals
Organizers of in-person clinical laboratory conferences face an interesting dilemma as they plan events in 2022: Where do they draw the line with COVID-19 safety protocols?
On one hand, the surge of cases caused by the SARS-CoV-2 Omicron variant seems to be in its waning stages and large swaths of the population are vaccinated. On the other hand, clinical laboratory and anatomic pathology events want potential registrants to have confidence that it is safe to travel and attend the gatherings.
One lab industry conference producer who happens to be knee-deep in preparing for an in-person meeting this spring is Robert Michel, Editor-in-Chief of The Dark Report and Founder of the 27th Annual Executive War College on Laboratory and Pathology Management. This informative event takes place on April 27-28 in New Orleans and includes COVID-19 protocols to protect attendees.
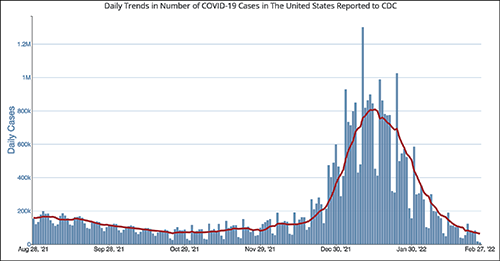
The CDC chart above shows the daily number of new COVID-19 cases in the US for the six-month period ending Feb. 28, 2022. Clinical laboratory managers should note that the number of new cases is at its lowest level since the Omicron variant showed up early this year.
“It’s important for all those planning to attend this year’s Executive War College to know that screening COVID-19 protocols will be in place to ensure the health and safety of all participants,” Michel noted. “We did a large lab conference in the fall of 2021 that included protocols for COVID-19 and the attendees told us they appreciated the protection provided by those protocols.”
After a significant rise in COVID-19 cases in January 2022 due to the Omicron variant, current daily case levels now are lower than they were six months ago before the new variant hit, according to numbers from the federal Centers for Disease Control and Prevention (CDC).
The in-person 2021 Executive War College, which took place in San Antonio on Nov. 2-3, 2021, followed the CDC’s recommendations:
COVID-19 protocols included a daily set of questions and a temperature check for all speakers and attendees before they were allowed to enter the conference area.
CLIA-complex rapid PCR COVID-19 tests were available for individuals whose temperature and answers to the screening questions indicated the need for such testing.
Attendees used an app to answer the daily screening questions and upload proof of vaccination.
“At last fall’s Executive War College, approximately 400 attendees were screened on each of the three days before entering the conference area and not one rapid COVID-19 test was needed,” Michel said. “Not only is that an outstanding outcome, but a number of attendees also told us they appreciated our efforts to keep them safe and protect their health.”
The 2022 Executive War College will follow the CDC’s updated COVID-19 guidelines, along with any state and local directives in effect as of April 27.
Although 300 attendees were expected at the 2021 Executive War College, 400 registered and participated.
Proof of Vaccination Has Been Required at Other Clinical Lab Industry Events
Organizers of other clinical lab conferences also have dealt with COVID-19 safety protocols. For example, the American Clinical Laboratory Association (ACLA) will hold its annual meeting in Washington, D.C., on March 9. COVID-19-related requirements for attendees will include proof of vaccination uploaded to a vaccine verification vendor and proof of a negative PCR test taken within 72 hours prior to the event.
The annual meeting of the American Society of Clinical Pathology (ASCP) occurs later this year in September in Chicago—too early yet to publish protocols. Last year’s ASCP conference in Boston was a hybrid event, offering both in-person and virtual options. Those who attended in person needed to upload proof of vaccination to a third-party vendor and were required to wear masks. On-site COVID-19 testing was available.
Revived Corporate Travel Could Boost Clinical Laboratory Conferences
The path back to live events across all industries has not been easy given various COVID-19 surges, political divisiveness over masking, frozen corporate travel budgets, and corporate policies banning or limiting employee travel.
Conference organizers throughout the United States universally hope those barriers will lower as 2022 progresses.
“With the fast-spreading Omicron triggering another round of setbacks to start 2022, event planners now are betting on spring to finally mark a turning point for the hard-hit industry,” MarketWatch reported on Feb. 4. “Their hopes hinge on American corporations taking a note from the recovery already under way for domestic air travel for leisure purposes, with the linchpin being a robust revival of trade show attendance and other in-person business gatherings.”
For Michel, offering actionable advice through well-thought-out sessions has been a cornerstone of the content offered each year at the Executive War College. He believes that approach will continue to be the strongest drawing point for clinical laboratory and pathology executives now considering attending the event.
“Our reading of the tea leaves is that across the profession of laboratory medicine, a great many managers, administrators, executives, and pathologists want to return to in-person conferences,” Michel noted. “Registrations for our April event are running ahead of 2019, and people tell us that they recognize the changes in healthcare and the lab marketplace because of the pandemic. They want to understand what’s driving current trends, like greater consumer involvement in lab testing and how to get private payers to reimburse claims for COVID-19 and genetic tests, as well as how a growing number of clinical laboratories are incorporating artificial intelligence solutions in both clinical care settings and lab operations.”
Study conducted on International Space Station found crew’s red blood cells were destroyed 54% faster in space than while on Earth
Hemolysis in blood specimens is something that clinical laboratories deal with every day. Now researchers in Canada have determined that, while astronauts are in space, hemolysis is a causative factor in the condition known as “space anemia.”
Hematologists whose clinical laboratories process a steady volume of complete blood count (CBC) tests to diagnosis anemia will want to take note of this research study, which was conducted at the University of Ottawa and on the International Space Station. Dubbed the “MARROW” study, it may have uncovered not only why astronauts suffer from anemia even a year after returning to Earth, but also how those insights can be applied to treatments for anemia and other blood diseases for Earthbound patients as well.
Anemia is caused by a marked decrease in the number of red blood cells and can lead to weakness, persistent fatigue, and slower brain function, which on Earth is concerning, but in space can be life threatening.
“Space anemia has consistently been reported when astronauts returned to Earth since the first space missions, but we didn’t know why,” said the study’s lead author Guy Trudel, MD, in a University of Ottawa news release.
Trudel is Director of the Bone and Joint Research Laboratory at the Ottawa Hospital Rehabilitation Centre in Canada. He is also a Rehabilitation Physician and Researcher at the Ottawa Hospital and Professor of Medicine at the University of Ottawa, and the principal investigator of the MARROW study, which is investigating the effects of microgravity on bone marrow, according to NASA.
“Our study shows that upon arriving in space, more red blood cells are destroyed, and this continues for the entire duration of the astronaut’s mission,” he added.
Although these scientific findings may not immediately lead to new methodologies for testing human blood for use in clinical laboratories, the insights gleaned from the study could inform future studies designed to learn how to get the body to produce more red blood cells in ways that benefit patients diagnosed with anemia or other blood disorders.
Guy Trudel, MD (above), Rehabilitation Physician and Researcher at the Ottawa Hospital and Professor at the University of Ottawa, is lead author of a Canadian study explaining why astronauts develop “space anemia.” In space, astronauts’ red blood cells are destroyed 54% faster than while on Earth, a finding that could have implications for space tourists and astronauts on longer missions to the moon and Mars, the researchers noted. (Photo copyright: University of Ottawa.)
Effects of Anemia Continue One Year after Returning to Earth
The MARROW research project, which was funded by the Canadian Space Agency (CSA), required the participation of 14 astronauts on the International Space Station.
The researchers began collecting data in October 2015 and completed their final tests in June 2020. They found that astronauts’ bodies destroyed 54% more red blood cells in space than would be normal on Earth, according to the study published in Nature Medicine.
“Thankfully, having fewer red blood cells in space isn’t a problem when your body is weightless,” Trudel said in the news release. “But when landing on Earth, and potentially on other planets or moons, anemia affecting your energy, endurance, and strength can threaten mission objectives. The effects of anemia are felt once you land and must deal with gravity again.”
The MARROW experiment detected the following changes:
During a six-month mission, astronauts’ bodies were destroying 54% more red blood cells than typical preflight rates.
Five of the 13 astronauts who had their blood drawn shortly after landing back on Earth were anemic. Red blood cell levels gradually improved three to four months post-flight.
The rate of red blood cell destruction remained 30% higher one year after landing than before missions to the International Space Station.
“Increased hemolysis as a primary effect of exposure to space constitutes a paradigm shift in our understanding of space anemia … Persistent hemolysis during space missions suggests that the longer the exposure, the worse the anemia,” the study’s authors wrote.
Measurements were made by testing the astronauts’ blood for iron levels and using breath tests to measure exhaled carbon monoxide. One molecule of carbon monoxide is produced every time one molecule of heme, the deep-red pigment in blood cells, is destroyed.
According to the researchers, the discovery that space travel increases red blood cell destruction:
highlights the need to screen astronauts and space tourists for existing blood or health conditions that are affected by anemia;
impacts longer missions to the moon and Mars, which would likely worsen an astronaut’s anemia;
suggests astronauts require an adapted diet; and
shows it is unclear how long the body can maintain this higher rate of destruction and production of red blood cells.
Space Study Could Lead to Better Healthcare on Earth
A 2007 NASA study published in Microgravity Science and Technology blamed space anemia on water loss during space flight decreasing the amount of hemoglobin in red blood cells. The study labeled space anemia a “15-day ailment” because those researchers believed issues resolved within 15 days of crew members returning to Earth.
The MARROW study, however, found much longer-lasting implications for astronauts in space, which could lead to new insights for patients on Earth. The Canadian Space Agency believes the study’s findings could lead to better understanding and monitoring of the effects of physical inactivity on seniors, bedridden patients, and those with reduced mobility or undergoing rehabilitation.
“The findings have implications for understanding the physiological consequences of space flight and anemia in patients on the ground,” Sulekha Anand, PhD, a professor in the Department of Biological Sciences at San Jose State University, told Reuters.
This latest study shows how discoveries in space continue to lead to advancements in scientists’ understanding of how the human body functions. That knowledge may one day provide the foundation for developing new or improved clinical laboratory tests for astronauts as well as everyday earthlings.
Survey shows more than 50% of hospitals and health systems plan to increase virtual care services within two years, a development that can change how patients access clinical laboratory testing services
If anything positive came out of the COVID-19 pandemic, it’s the growing acceptance by physicians and health payers of telehealth—including telepathology, teleradiology, and other types of virtual doctor visits—as a way for patients to meet with their physicians in place of in-office healthcare.
In earlier coverage about the rapid adoption of telehealth and virtual doctor visits, Dark Daily has observed that this trend creates a unique challenge for clinical laboratories. If the patient has a virtual consultation with his or her physician, how would a clinical laboratory get access to this patient to do a venipuncture and collect the samples necessary to perform the medical laboratory tests ordered by the physician?
Nevertheless, according to multiple reports, healthcare providers are planning to increase investment in telehealth technologies.
Disparate Technologies Led to Technical Difficulties for Virtual Healthcare Providers
The terms telemedicine and telehealth are often used interchangeably. However, according to the American Academy of Family Physicians (AAFP), there are subtle differences worth noting.
Telehealth is a broad term which refers to “electronic and telecommunications technologies and services used to provide care and services at-a-distance [while] telemedicine is the practice of medicine using technology to deliver care at a distance.
“Telehealth is different from telemedicine in that it refers to a broader scope of remote health care services than telemedicine. Telemedicine refers specifically to remote clinical services, while telehealth can refer to remote non-clinical services,” the AAFP notes.
Kelly Lewis, former Vice President of Revenue Strategy and Enablement at telehealth provider Amwell, told Healthcare IT News (HIT News) that “the COVID-19 pandemic caused telehealth adoption to skyrocket.
However, “Because much of this adoption was driven out of an abundance of necessity, there was little time for organizations to think strategically about their technology investments,” she added.
“With urgency at a high, payers, provider organizations and clinicians all turned to the quickest options available so patients could continue to get care. The result, however, was what we are calling platform ‘sprawl’—the use of a number of disparate solutions that are leading to a confusing and frustrating care delivery system and experience.”
Nevertheless, according to a survey conducted by HIT News and HIMSS Analytics, “More than half (56%) of hospital and health system leaders say they are planning to increase their investment in telemedicine during the next two years.” This, “shows that the huge surge in and mainstreaming of telehealth during the ongoing pandemic has caused the C-suite and other healthcare leaders to embrace the technology that has for so long existed on the periphery of medicine,” HIT News noted.
“The clear message is that telehealth is here to stay and will continue to expand,” Lewis told HIT News, adding, “The majority of payers without virtual care offerings also reported planning to add them in the next 24 months.”
“Clinicians agree that moving toward a fully integrated telehealth platform would be beneficial. More than 80% believe investing in a fully integrated virtual or hybrid care system would have a positive impact on clinical outcomes and patient experiences,” Kelly Lewis (above), former VP at telehealth provider Amwell, told Healthcare IT News. Considering the growing demand for telehealth, pathologists and clinical laboratories will need a strategy for supporting virtual healthcare providers. (Photo copyright: Healthcare IT News.)
The HIT News/HIMSS Analytics survey findings suggest telehealth will transition as providers aim for “smart-growth” instead of “pandemic-fueled expediency,” Becker’s Hospital Review reported.
Survey respondents expressed positive attitudes about telehealth:
56% of healthcare leaders plan to increase investment in virtual care over the next two years.
80% of respondents noted “very” or “extremely” important telehealth factors are integrating with existing workflows, fast video connections, and reducing administrative burden.
77% called telehealth platform integration with the electronic health record (EHR) “very” or “extremely” important.
80% envision positive clinical outcomes and patient experiences from a fully integrated telemedicine platform.
75% of payers said a single digital platform has potential to streamline member experiences.
“With telehealth visits stabilizing at roughly 10 times pre-pandemic levels, digital transformation initiatives are rising across the field. As a result of the pandemic, 60% of healthcare organizations are adding new digital projects, with telemedicine becoming a higher priority for 75% of executives (vs. 42% in 2019) to improve the patient experience,” the AHA reported.
Medical laboratories and anatomic pathology groups are advised to keep pace with the changing healthcare landscape which increasingly puts a premium on remote and virtual visits. This has become even more critical as healthcare providers and investors infuse more capital into telehealth technology.
As physicians expand telemedicine virtual office visits post-pandemic, a clinical laboratory strategy to reach patients and acquire specimens will be required.