Challenges abound as the NHS tries to recover before UK citizens move to private insurance; some patients have wait times of up to six months for a histopathology diagnosis of cancer
As we noted, thousands of clinical laboratory tests and surgical pathology readings had to be delayed or cancelled due to the strikes.
An NHS worker in a Liverpool hospital told CNN that conditions felt like a “war zone” with patients being treated in the backs of ambulances, corridors, waiting rooms, cupboards, or not at all since hospitals are well over capacity.
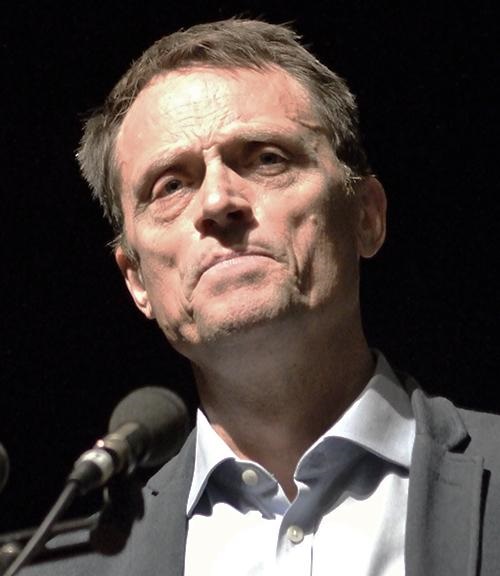
“Those who can afford to get private insurance are,” Chris Thomas (above), told The Guardian. Thomas is Head of the Commission on Health and Prosperity for UK progressive policy think tank the Institute for Public Policy Research (IPPR). “People are not opting out of the NHS because they have stopped believing in it as the best and fairest model of healthcare,” he said. “Rather, those who can afford it are being forced to go private … and those without the funds are left to ‘put up or shut up.’” (Photo copyright: Institute for Public Policy Research.)
Two-Tier System Could Become UK’s Norm, Dividing Classes
The drive towards private insurance is leaving Britain on the brink of having a “two-tier” system where the NHS is overpowered by private healthcare. And it’s not an unwarranted fear. One in six people in Britain are prepared to use private healthcare instead of waiting for the NHS, The Guardian reported.
A report from the Institute for Public Policy Research (IPPR) claims a UK two-tiered system would not mimic what we have here in the US. Rather, if the trend continues in the private direction, it would more likely be comparable to dentistry in England, “… where poor NHS access exists for some and superior but expensive access exists for many. We stand at the precipice of a growing ‘opt-out’ by those who can,” according to the IPPR report, The Guardian noted.
More importantly, this could further divide classes. “Such a trend could threaten the deep and widespread public support for the NHS among voters and leave millions of patients vulnerable because of their ethnicity, postcode, income or job,” The Guardian noted the IPPR report as saying.
“It’s different when you see your everyday reality though naïve eyes. He saw the elderly patients on the jigsaw of trolleys crammed into the department, pushed against the wall, squeezed in the gap between the bed and nursing stations.
“He saw the fluids hanging from rails where we had no stands, lines running into the patient’s forearms. He saw the oxygen fed into their noses from cylinders propped along the bed, the cacophony of beeping machines and alarms.
“It doesn’t look like it does on the TV. It doesn’t even look like it does on reality TV,” she wrote.
The healthcare statistics are alarming. According to CNN:
There was a 20% increase in excess deaths the final week of December 2022, compared to the previous five years.
Half of patients waiting for emergency care that month waited for more than four hours, which was a record.
Also in December, 54,000 people waited more than 12 hours for emergency admission. The wait was “virtually zero” prior to the COVID-19 pandemic.
And “category 2” conditions, such as a stroke or heart attack, had a more than 90-minute wait time for ambulance attendance. The target response time is 18 minutes.
Dim Hopes for Improvement
Though the NHS has struggled in recent years, the challenges are seemingly worse now. “This time feels different. It’s never been as bad as this,” gastroenterologist Peter Neville, MD, a consultant physician who worked with the NHS since 1989, told CNN.
CNN noted that a perfect storm of challenges might have brought the NHS to where it is today. COVID-19, flu seasons paired with COVID, lack of financial support, lack of social support, staffing and morale issues are just some of the problems that the NHS must address.
Experts point out that as the NHS’ struggles increase so begins a loop where one problem feeds another. Patients who wait to be seen have treatments that take longer, then they get sicker, and the cycle continues.
Despite having one of the highest proportions of government healthcare spending on Earth, up to 40% of Britons report having accessed or plan to access private care, Breitbart reported.
Sadly, it’s unlikely enough cash will come in from the UK government to make significant improvements for the NHS. The budget announcement in November showed the NHS was to get an average 2% spending increase over the next two years, CNN reported.
Are there lessons here for US hospitals, clinical laboratories, and pathology groups? Perhaps. It’s always instructive to see how our fellow healthcare providers across the pond respond to public pressure for more access to quality care.
More than 10,000 doctors walked out for the second time in two months, further burdening an already overwhelmed NHS
On April 11, tens of thousands of junior doctors (similar to medical residents in the US) left their posts in British hospitals commencing a four-day walkout. The strike resulted in the cancellation of thousands of operations and appointments, as well as cancelling or delaying thousands of clinical laboratory tests and anatomic pathology readings associated with those healthcare visits and surgical procedures.
The walkout was spurred by pay concerns and working conditions and comes on the heels of a three-day strike last month. That strike had already weakened the UK’s frail National Health System (NHS), which has become inundated with appointment backlogs that predate the COVID-19 pandemic, and which has led to longer wait times to see a doctor, ABC News reported.
This latest strike was more perilous since the senior doctors who covered for their juniors during last month’s strike were previously on leave for a holiday weekend, United Press International (UPI) reported.
“These strikes are going to have a catastrophic impact on the capacity of the NHS to recover,” Matthew Taylor (above), Chief Executive of the NHS Confederation, told Sky News. “The health service has to meet high levels of demand at the same time as making inroads into that huge backlog … That’s a tough thing to do at the best of times—it’s impossible to do when strikes are continuing.” (Photo copyright: Wikimedia Commons.)
Junior Docs Cite Injustice
Junior doctors who walked out are calling for a 35% pay raise to right the wrongs of 15 years of below-inflation raises, but the government continues to argue it cannot afford to increase pay, UPI noted.
“There is nothing ‘junior’ about the work I have done as a doctor. For an hour of work that I might save a life, I can be paid 19£ [$23.65],” said Jennifer Barclay, MD, a surgical junior doctor in the UK’s North West electoral zone, in a British Medical Association (BMA) press release.
“My dad, an electrician, tells me to quit and retrain in his footsteps. I’d be earning more, have less stress, less responsibility, better hours, and a better work-life balance after three years,” she added. “Surely, this life, this training, responsibility, debt, and crushing workload is worth more than 19£ per hour? I’ll be on the picket line this week because doctors believe that it is.”
According to the BMA, newly qualified junior doctors earn just over 14£ ($17.43) per hour, ABC News reported, which added, “The doctors’ union has asked for a 35% pay rise to bring junior doctor pay back to 2008 levels.”
However, their pay demands come in the midst of a cost-of-living crisis in the UK. Inflation has risen above 10%. Paired with increases in heating costs and food prices mean that decreased wages leave many struggling to pay bills, ABC news reports.
A hard-hitting BMA advertising campaign designed to shine light on these disparities depicts three junior doctors (with one-, seven-, and 10-years’ experience) removing an appendix. The video shows that the total the three would be paid for the hour-long operation would be 66.55£ ($82.84):
Doctor with one year experience: 14.09£ ($17.54).
Doctor with two years’ experience: 24.46£ ($30.45).
Doctor with three years’ experience: 28£ ($34.85).
And this for performing a potentially life-saving procedure, the BMA stated.
In the press release, BMA Junior Doctors Committee co-chairs Robert Laurenson and Vivek Trivedi said, “It is appalling that this government feels that paying three junior doctors as little as 66.55£ between them for work of this value is justified. This is highly skilled work requiring years of study and intensive training in a high-pressure environment where the job can be a matter of life or death.”
Patient Care is Affected
Lower salaries also affect patient care levels and have led to recruitment issues, with many doctors leaving the profession, the BBC reported. “This is not a situation where we are fixed in our position. We’re looking for negotiations and Steve Barclay (UK’s Secretary of State for Health and Social Care) isn’t even willing to talk to us. He hasn’t put any offer at all on the table … there has to be two sides in the discussion,” Emma Runswick, MD, a junior doctor and deputy chairwoman of the BMA, told the BBC.
But while the junior doctors battle for wages, the government’s initial focus has been on patient wellbeing. “There will be risks to patient safety, risks to patient dignity, as we are not able to provide the kind of care we want to,” NHS Confederation Chief Executive Matthew Taylor told UPI prior to the walkout.
The timing of the walkout also caused consternation with the NHS. “Not only will walkouts risk patient safety, but they have been timed to maximize disruption after the Easter break,” Health Secretary Barclay told UPI as the walkout was announced.
Barclay also claimed the amount sought by doctors was “unreasonable” and would cause raises above $25,000 per year, UPI reported. “If the BMA is willing to move significantly from this position and cancel strikes, we can resume confidential talks and find a way forward as we have done with other unions,” he stated.
It is important to note that doctors would be pulled from picket lines if immediate danger were present due to trade union laws that say life-and-limb coverage must be provided, the BMA told the BBC.
Research in the UK and US into how rapid WGS can prevent deaths and improve outcomes for kids with rare genetic diseases may lead to more genetic testing based in local clinical laboratories
Genetic scientists with the National Health Service (NHS) in England have embarked on an ambitious plan to offer rapid whole genome sequencing (rWGS) for children and babies with serious illnesses, as part of a larger initiative to embrace genomic medicine in the United Kingdom (UK).
The NHS estimates that the plan will benefit more than 1,000 children and babies each year, including newborns with rare diseases such as cancer, as well as kids placed in intensive care after being admitted to hospitals. Instead of waiting weeks for results from conventional tests, clinicians will be able to administer a simple blood test and get results within days, the NHS said in a press release.
The press release notes that about 75% of rare genetic diseases appear during childhood “and are responsible for almost a third of neonatal intensive care deaths.”
Here in the United States, pathologists and clinical laboratory managers should see this development as a progressive step toward expanding access to genetic tests and whole genome sequencing services. The UK is looking at this service as a nationwide service. By contrast, given the size of the population and geography of the United States, as this line of medical laboratory testing expands in the US, it will probably be centered in select regional centers of excellence.
“This strategy sets out how more people will be empowered to take preventative action following risk-based predictions, receive life-changing diagnoses, and get the support needed to live with genomically-informed diagnoses alongside improved access to cutting-edge precision [medicine] treatments. It also outlines how the NHS will accelerate future high-quality genomic innovation that can be adopted and spread across the country, leading to positive impacts for current and future generations,” the NHS wrote.
“This global first is an incredible moment for the NHS and will be revolutionary in helping us to rapidly diagnose the illnesses of thousands of seriously ill children and babies—saving countless lives in the years to come,” said NHS chief executive Amanda Pritchard (above) in a press release announcing the program. (Photo copyright: Hospital Times.)
New Rapid Whole Genome Sequencing Service
The NHS announced the plan following a series of trials last year. In one trial, a five-day old infant was admitted to a hospital in Cheltenham, Gloucester, with potentially deadly levels of ammonia in his blood. Whole genome sequencing revealed that changes in the CPS1 gene were preventing his body from breaking down nitrogen, which led to the spike in ammonia. He was given life-saving medication in advance of a liver transplant that doctors believed would cure the condition. Without the rapid genetic test, doctors likely would have performed an invasive liver biopsy.
Using a simple blood test, the new newborn genetic screening service in England is expected to benefit more than 1,000 critically ill infants each year, potentially saving their lives. “The rapid whole genome testing service will transform how rare genetic conditions are diagnosed,” explained Emma Baple, PhD, Professor of Genomic Medicine at University of Exeter Medical School and leader of the National Rapid Whole Genome Sequencing Service in the press release. “We know that with prompt and accurate diagnosis, conditions could be cured or better managed with the right clinical care, which would be life-altering—and potentially life-saving—for so many seriously unwell babies and children,” Precision Medicine Institute reported.
According to The Guardian, test results will be available in two to seven days.
Along with the new rWGS testing service, the NHS announced a five-year plan to implement genomic medicine more broadly. The provisions include establishment of an ethics advisory board, more training for NHS personnel, and an expansion of genomic testing within the existing NHS diagnostic infrastructure. The latter could include using NHS Community Diagnostics centers to collect blood samples from family members to test for inherited diseases.
UK’s Longtime Interest in Whole Genome Sequencing
The UK government has long been interested in the potential role of WGS for delivering better outcomes for patients with genetic diseases, The Guardian reported.
In 2013, the government launched the 100,000 Genomes Project to examine the usefulness of the technology. In November 2021, investigators with the project reported the results of a large pilot study in which they analyzed the genomes of 4,660 individuals with rare diseases. The study, published in the New England Journal of Medicine (NEJM) titled, “100,000 Genomes Pilot on Rare-Disease Diagnosis in Health Care—Preliminary Report,” found “a substantial increase in yield of genomic diagnoses made in patients with the use of genome sequencing across a broad spectrum of rare disease.”
The study’s findings suggest that use of WGS “could save the NHS millions of pounds,” The Guardian reported.
Whole Genome Sequencing System for Newborns in the US
“This NBS-rWGS [newborn screening by rapid whole genome sequencing] system is designed to complement the existing newborn screening process and has the potential to eliminate the diagnostic and therapeutic odyssey that many children and parents face,” Kingsmore said in a press release. “Currently, only 35 core genetic disorders are recommended for newborn screening in the United States, but there are more than 7,200 known genetic diseases. Outcomes remain poor for newborns with a genetic disease because of the limited number of recommended screenings. With NBS-rWGS, we can more quickly expand that number and therefore potentially improve outcomes through precision medicine.”
A more recent 2023 study which examined 112 infant deaths at Rady Children’s Hospital found that 40% of the babies had genetic diseases. In seven infants, genetic diseases were identified post-mortem, and in five of them “death might have been avoided had rapid, diagnostic WGS been performed at time of symptom onset or regional intensive care unit admission,” the authors wrote.
“Prior etiologic studies of infant mortality are generally retrospective, based on electronic health record and death certificate review, and without genome information, leading to underdiagnosis of genetic diseases,” said Christina Chambers, PhD, co-author of the study, in a press release. “In fact, prior studies show at least 30% of death certificates have inaccuracies. By implementing broad use of genome sequencing in newborns we might substantially reduce infant mortality.”
Pioneering work with whole genome sequencing for newborns, such as that being conducted by the clinical laboratory and genetic teams at Rady Children’s Hospital and the UK’s NHS, could allow doctors to make timely interventions for our most vulnerable patients.
Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
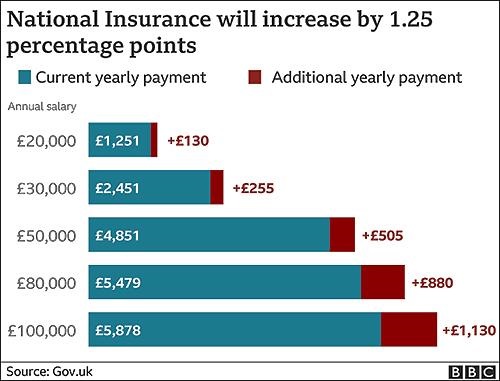
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
With improved genetic sequencing comes larger human genome databases that could lead to new diagnostic and therapeutic biomarkers for clinical laboratories
As the COVID-19 pandemic grabbed headlines, the human genome database at the US Department of Veterans Affairs Million Veterans Program (MVP) quietly grew. Now, this wealth of genomic information—as well as data from other large-scale genomic and genetic collections—is expected to produce new biomarkers for clinical laboratory diagnostics and testing.
In December, cancer genomics company Personalis, Inc. (NASDAQ:PSNL) of Menlo Park, Calif., achieved a milestone and delivered its 100,000th whole human genome sequence to the MVP, according to a news release, which also states that Personalis is the sole sequencing provider to the MVP.
The VA’s MVP program, which started in 2011, has 850,000 enrolled veterans and is expected to eventually involve two million people. The VA’s aim is to explore the role genes, lifestyle, and military experience play in health and human illness, notes the VA’s MVP website.
Health conditions affecting veterans the MVP is researching include:
The VA has contracted with Personalis through September 2021, and has invested $175 million, Clinical OMICS reported. Personalis has earned approximately $14 million from the VA. That’s about 76% of the company’s revenue, according to 2nd quarter data, Clinical OMICS noted.
“The VA MVP is the largest whole genome sequencing project in the United States, and this is a significant milestone for both the program and for Personalis,” said John West (above with wife Judy), Founder and CEO of Personalis, in the news release. “Population-scale sequencing projects of this nature represent a cornerstone in our effort to accelerate the advancement of precision medicine across a wide range of disease areas,” he added. (Photo copyright: MIT Technology Review.)
Database of Veterans’ Genomes Used in Current Research
What has the VA gained from their investment so far? An MVP fact sheet states researchers are tapping MVP data for these and other veteran health-related studies:
Differentiating between prostate cancer tumors that require treatment and others that are slow-growing and not life-threatening.
How genetics drives obesity, diabetes, and heart disease.
How data in DNA translates into actual physiological changes within the body.
Gene variations and patients’ response to Warfarin.
NIH Research Program Studies Effects of Genetics on Health
Another research program, the National Institutes of Health’s All of Us study, recently began returning results to its participants who provided blood, urine, and/or saliva samples. The NIH aims to aid research into health outcomes influenced by genetics, environment, and lifestyle, explained a news release. The program, launched in 2018, has biological samples from more than 270,000 people with a goal of one million participants.
“We’re changing the paradigm for research. Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible,” said Josh Denny, MD, CEO of the NIH’s All of Us research program in the news release. Denny, a physician scientist, was Professor of Biomedical Informatics and Medicine, Director of the Center for Precision Medicine and Vice President for Personalized Medicine at Vanderbilt University Medical Center prior to joining the NIH. (Photo copyright: National Institutes of Health.)
Inclusive Data Could Aid Precision Medicine
The news release notes that more than 80% of biological samples in the All of Us database come from people in communities that have been under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, All of Us Genomics Program Director, in the news release.
Precision medicine designed for specific healthcare populations is a goal of the All of Us program.
“[All of Us is] beneficial to all Americans, but actually beneficial to the African American race because a lot of research and a lot of medicines that we are taking advantage of today, [African Americans] were not part of the research,” Chris Crawford, All of US Research Study Navigator, told the Birmingham Times. “As [the All of Us study] goes forward and we get a big diverse group of people, it will help as far as making medicine and treatment that will be more precise for us,” he added.
Large Databases Could Advance Care
Genome sequencing technology continues to improve. It is faster, less complicated, and cheaper to sequence a whole human genome than ever before. And the resulting sequence is more accurate.
Thus, as human genome sequencing databases grow, researchers are deriving useful scientific insights from the data. This is relevant for clinical laboratories because the new insights from studying bigger databases of genomic information will produce new diagnostic and therapeutic biomarkers that can be the basis for new clinical laboratory tests as well as useful diagnostic assays for anatomic pathologists.