Research could lead to similar treatments for other diseases, as well as creating a demand for a new line of oncology tests for clinical labs and pathology groups
Cancer treatment has come a long way in the past decades, and it seems poised to take another leap forward thanks to research being conducted at Rice University in Houston. Molecular scientists there have developed what they call a “molecular jackhammer” that uses special molecules and near-infrared light to attack and kill cancer cells.
The technique has been effective in research settings. Should it be cleared for use in patient care, it could change the way doctors treat cancer patients while giving clinical laboratories a new diagnostic tool that could guide treatment decisions.
The researchers “found that the atoms of a small dye molecule used for medical imaging can vibrate in unison—forming what is known as a plasmon [a quantum of plasma oscillation]—when stimulated by near-infrared light, causing the cell membrane of cancerous cells to rupture,” a Rice University news release noted.
The small dye molecule is called aminocyanine, a type of fluorescent synthetic dye that is already in use in medical imaging.
“These molecules are simple dyes that people have been using for a long time,” said physical chemistry scientist Ciceron Ayala-Orozco, PhD, the researcher who led the study, in the news release. “They’re biocompatible, stable in water, and very good at attaching themselves to the fatty outer lining of cells. But even though they were being used for imaging, people did not know how to activate these as plasmons.”
“The method had a 99% efficiency against lab cultures of human melanoma cells, and half of the mice with melanoma tumors became cancer-free after treatment,” according to the Rice University news release.
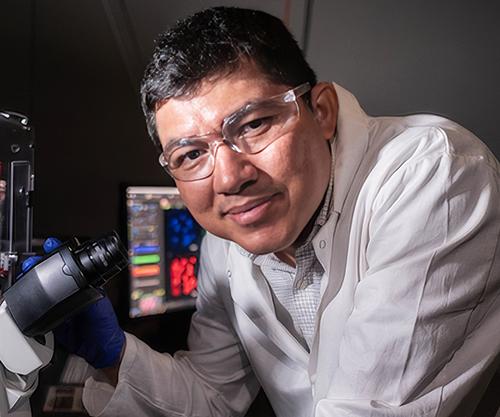
“I spent approximately four years working with these ideas on using molecular forces and what is called blue-light activated molecular motors,” Ciceron Ayala-Orozco, PhD (above), told Oncology Times. “At some point, I connected the dots that what I wanted to do is use a simple molecule, not necessarily a motor, that absorbs NIR light in similar ways as plasmonic nanoparticles do and go deeper into the tissue. When activated, we found that the molecules vibrate even faster than our minds can imagine and serve as a force to break the cancer cells apart.” Once approved for use treating cancer patients, clinical laboratories working with oncologists may play a key role in diagnosing candidates for the new treatment. (Photo copyright: Rice University.)
How the Technique Works
Nuclei of the aminocyanine molecules oscillate in sync when exposed to near-infrared radiation and pummel the surface of the cancer cell. These blows are so powerful they rupture the cell’s membrane sufficiently enough to destroy it.
“The speed of this type of therapy can completely kill the cancer much faster than, say, photodynamic therapy,” Ayala-Orozco noted. “The mechanical action through the molecular jackhammer is immediate, within a few minutes.”
One advantage to near-infrared light is that it can infiltrate deeper into the body than visible light and access organs and bones without damaging tissue.
“Near-infrared light can go as deep as 10 centimeters (four inches) into the human body as opposed to only half a centimeter (0.2 inches), the depth of penetration for visible light, which we used to activate the nanodrills,” said James Tour, PhD, T. T. and W. F. Chao Professor of Chemistry, Professor of Materials Science and NanoEngineering at Rice University, in the news release. “It is a huge advance.”
The molecular plasmons identified by the team had a near-symmetrical structure. The plasmons have an arm on one side that does not contribute to the motion, but rather anchors the molecule to the lipid bilayer of the cell membrane. The scientists had to prove that the motion could not be categorized as a form of either photodynamic or photothermal therapy.
“What needs to be highlighted is that we’ve discovered another explanation for how these molecules can work,” Ayala-Orozco said in the Rice news release. “This is the first time a molecular plasmon is utilized in this way to excite the whole molecule and to actually produce mechanical action used to achieve a particular goal—in this case, tearing apart cancer cells’ membrane.
“This study is about a different way to treat cancer using mechanical forces at the molecular scale,” he added.
New Ways to Treat Cancer
The likelihood of cancer cells developing a resistance to these molecular jackhammers is extremely low, which renders them a safer and more cost effective method for inducing cancer cell death.
“The whole difference about this is because it’s a mechanical action, it’s not relying on some chemical effect,” Tour told KOMO News. “It’s highly unlikely that the cell will be able to battle against this. Once it’s cell-associated, the cell is toast once it gets hit by light. Only if a cell could prevent a scalpel from being able to cut it in half, could it prevent this.
“It will kill all sorts of cell types. With our other mechanical action molecules, we’ve demonstrated that they kill bacteria; we’ve demonstrated that they kill fungi. If a person has lost the ability to move a limb, if you can stimulate the muscle with light, that would be quite advantageous. Cancer is just the beginning,” he added.
“From the medical point of view, when this technique is available, it will be beneficial and less expensive than methods such as photothermal therapy, photodynamics, radio-radiation, and chemotherapy,” said Jorge Seminario, PhD, Professor in the Artie McFerrin Department of Chemical Engineering at Texas A&M University in a news release.
“This is one of the very few theoretical-experimental approaches of this nature. Usually, research in the fields related to medicine does not use first principles quantum-chemistry techniques like those used in the present work, despite the strong benefit of knowing what the electrons and nuclei of all atoms are doing in molecules or materials of interest,” Seminario noted.
“It’s really a tremendous advance. What this is going to do is open up a whole new mode of treatment for medicine,” Tour said. “It’s just like when radiation came in [and] when immunotherapy came in. This is a whole new modality. And when a new modality comes in, so much begins to open up.
“Hopefully, this is going to change medicine in a big way,” he added.
More research and clinical studies are needed before this new technology is ready for patient care. Clinical laboratories and anatomic pathology groups will likely be involved identifying patients who would be good candidates for the new treatment. These molecular jackhammers could be a useful tool in the future fight against cancer, which is ranked second (after heart disease) as the most common cause of death in the US.
Similar diagnostic delays due to clinical laboratory staff shortages are reported in other nations as well
Critical pathology shortages are causing lengthy delays for clinical laboratory test results in New Zealand, according to a report that states some patients are waiting over a month for a melanoma diagnosis. This situation puts the lives of cancer patients at risk in the island nation.
The Melanoma Network of New Zealand (MelNet) is working to reduce the number of people who develop the disease and help melanoma patients receive a fast diagnosis and proper treatment and care.
However, plastic surgeon and MelNet Chair Gary Duncan, MBChB, FRACS, told Radio New Zealand (RNZ) that when patients return to their doctors for test results, those results often have not come back from the medical laboratory. Therefore, the physician cannot discuss any issues with the patient, which causes them to make another appointment for a later date or receive a melanoma diagnosis over the telephone, RNZ reported.
Dermatologist Louise Reiche, MBChB, FRACS, told RNZ that slow pathology services are unfair to patients. Such delays could result in the spreading of the melanoma to other parts of the body and require major surgery under anesthetic.
“Not only will they suffer an extensive surgical procedure, but it could also shorten their life,” she said.
“We’ve got shortages across the board, and it only seems to be getting worse,” said Trishe Leong, MB.BS (hons) Medicine, FRCPA Anatomical Pathology (above), President of the Royal College of Pathologists of Australasia (RCPA). She added that “there was also a backlog of pathological examinations of placentas, which are used to detect genetic conditions and shed light on complex births,” The Sydney Morning Herald reported. Clinical laboratories in several countries worldwide are experiencing similar delays in reporting critical test results to physicians and their patients. (Photo copyright: RCPA.)
Pathology Labs Cannot Meet Demand for Testing
The Royal College of Pathologists recommends that 80% of specimen results should be returned to clinicians within five days. General practitioner Jeremy Hay, MD, of the Upper Hutt Skin Clinic told RNZ that he has never seen a melanoma report returned from the laboratory he utilizes within the suggested five-day time span. He stated that his local pathology lab simply cannot meet the demand for the vast number of samples waiting to be tested.
“I have visited the lab, and you can see even in the corridors stacks of unreported slides sitting outside the pathologist’s rooms, and there are more inside their rooms,” he said. “They need more staff and that’s quite obvious.”
Hay added that, because of the delays, he typically does not start with a small biopsy of a suspicious-looking piece of skin. Instead, he just cuts the entire area out and sends it to the lab for testing to expedite the diagnosis process.
Lab Loses Accreditation Due to Delays
Long delays caused one lab—Auckland’s Community Anatomic Pathology Service (APS)—to lose its accreditation for the lab’s skin testing department. According to RNZ, some patients had to wait up to eight weeks to learn whether they had melanoma.
An article published by medical/science specialty recruiting firm Odyssey, states that the deficiency at APS was due to several factors, including:
Population growth.
An increase in private medical practices.
The underestimation of the costs required to run the lab.
An overestimation of potential savings.
A shortage of qualified pathologists, specifically in the fields of anatomical, chemical, and forensic pathology.
The article also states that pathologists are now listed on Immigration New Zealand’s list of shortage skills in the country. That designation means that foreign candidates who have the skills, and who are offered jobs in the country, can immediately apply for permanent residency.
Three Week Wait for Cancer Diagnoses in Australia
According to the World Cancer Research Fund International (WCRF), New Zealand has the second highest rate of melanoma in the world. The number one spot is held by Australia.
Other countries are experiencing long wait times for cancer diagnoses as well. According to The Sydney Morning Herald, some individuals are waiting up to three weeks to receive a cancer diagnosis due to a shortage of pathologists.
In those countries, and around the world, healthcare experts say the solution is expanding training opportunities to solve the shortage of clinical laboratory scientists, medical laboratory and imaging technologists, doctors, nurses, and other medical professionals, and increasing funding for modernizing hospital facilities and clinics.
But in countries with government-run healthcare, that solution is problematic at best.
According to an EADV press release, the AI software demonstrated a “100% (59/59 cases identified) sensitivity for detecting melanoma—the most serious form of skin cancer.” The AI software also “correctly detected 99.5% (189/190) of all skin cancers and 92.5% (541/585) of pre-cancerous lesions.”
“Of the basal cell carcinoma cases, a single case was missed out of 190, which was later identified at a second read by a dermatologist ‘safety net.’ This further demonstrates the need to have appropriate clinical oversight of the AI,” the press release noted.
AI is being utilized more frequently within the healthcare industry to diagnose and treat a plethora of illnesses. This recent study performed by scientists in the United Kingdom demonstrates that new AI models can be used to accurately diagnose some skin cancers, but that “AI should not be used as a standalone detection tool without the support of a consultant dermatologist,” the press release noted.
“The role of AI in dermatology and the most appropriate pathway are debated,” said Kashini Andrew, MBBS, MSc (above), Specialist Registrar at University Hospitals Birmingham NHS Foundation Trust. “Further research with appropriate clinical oversight may allow the deployment of AI as a triage tool. However, any pathway must demonstrate cost-effectiveness, and AI is currently not a stand-alone tool in dermatology. Our data shows the great promise of AI in future provision of healthcare.” Clinical laboratories and dermatopathologists in the United States will want to watch the further development of this AI application. (Photo copyright: LinkedIn.)
How the NHS Scientists Conducted Their Study
Researchers tested their algorithm for almost three years to determine its ability to detect cancerous and pre-cancerous growths. A group of dermatologists and medical photographers entered patient information into their algorithm and trained it how to detect abnormalities. The collected data came from 22,356 patients with suspected skin cancers and included photos of known cancers.
The scientists then repeatedly recalibrated the software to ensure it could distinguish between non-cancerous lesions and potential cancers or malignancies. Dermatologists then reviewed the final data from the algorithm and compared it to diagnoses from health professionals.
“This study has demonstrated how AI is rapidly improving and learning, with the high accuracy directly attributable to improvements in AI training techniques and the quality of data used to train the AI,” said Kashini Andrew, MBBS, MSc, Specialist Registrar at University Hospitals Birmingham NHS Foundation Trust, and co-author of the study, in EADV press release.
Freeing Up Physician Time
The EADV Congress where the NHS researchers presented their findings took place in October in Berlin. The first model of their AI software was tested in 2021 and that version was able to detect:
85.9% (195 out of 227) of melanoma cases,
83.8% (903 out of 1078) of all skin cancers, and
54.1% (496 out of 917) of pre-cancerous lesions.
After fine-tuning, the latest version of the algorithm was even more promising, with results that included the detection of:
100% (59 out of 59) cases of melanoma,
99.5% (189 out of 190) of all skin cancers, and
92.5% (541 out of 585) pre-cancerous lesions.
“The latest version of the software has saved over 1,000 face-to-face consultations in the secondary care setting between April 2022 and January 2023, freeing up more time for patients that need urgent attention,” Andrew said in the press release.
Still, the researchers admit that AI should not be used as the only detection method for skin cancers.
“We would like to stress that AI should not be used as a standalone tool in skin cancer detection and that AI is not a substitute for consultant dermatologists,” stated Irshad Zaki, B Med Sci (Hons), Consultant Dermatologist at University Hospitals Birmingham NHS Foundation Trust and one of the authors of the study, in the press release.
“The role of AI in dermatology and the most appropriate pathway are debated. Further research with appropriate clinical oversight may allow the deployment of AI as a triage tool,” said Andrew in the press release. “However, any pathway must demonstrate cost-effectiveness, and AI is currently not a stand-alone tool in dermatology. Our data shows the great promise of AI in future provision of healthcare.”
Two People in the US Die of Skin Cancer Every Hour
According to the Skin Cancer Foundation, skin cancer is the most common cancer in the United States as well as the rest of the world. More people in the US are diagnosed with skin cancer every year than all other cancers combined.
When detected early, the five-year survival rate for melanoma is 99%, but more than two people in the US die of skin cancer every hour. At least one in five Americans will develop skin cancer by the age of 70 and more than 9,500 people are diagnosed with the disease every day in the US.
The annual cost of treating skin cancers in the United States is estimated at $8.1 billion annually, with approximately $3.3 billion of that amount being for melanoma and the remaining $4.8 billion for non-melanoma skin cancers.
More research is needed before University Hospitals Birmingham’s new AI model can be used clinically in the diagnoses of skin cancers. However, its level of accuracy is unprecedented in AI diagnostics. This is a noteworthy step forward in the field of AI for diagnostic purposes that can be used by clinical laboratories and dermatopathologists.
MIT’s deep learning artificial intelligence algorithm demonstrates how similar new technologies and smartphones can be combined to give dermatologists and dermatopathologists valuable new ways to diagnose skin cancer from digital images
According to an MIT press release, “The paper describes the development of an SPL [Suspicious Pigmented Lesion] analysis system using DCNNs [Deep Convolutional Neural Networks] to more quickly and efficiently identify skin lesions that require more investigation, screenings that can be done during routine primary care visits, or even by the patients themselves. The system utilized DCNNs to optimize the identification and classification of SPLs in wide-field images.”
The MIT scientists believe their AI analysis system could aid dermatologists, dermatopathologists, and clinical laboratories detect melanoma, a deadly form of skin cancer, in its early stages using smartphones at the point-of-care.
“Our research suggests that systems leveraging computer vision and deep neural networks, quantifying such common signs, can achieve comparable accuracy to expert dermatologists,” said Luis Soenksen, PhD (above), Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in an MIT press release. “We hope our research revitalizes the desire to deliver more efficient dermatological screenings in primary care settings to drive adequate referrals.” The MIT study demonstrates that dermatologists, dermatopathologists, and clinical laboratories can benefit from using common technologies like smartphones in the diagnosis of disease. (Photo copyright: Wyss Institute Harvard University.)
Improving Melanoma Treatment and Patient Outcomes
Melanoma develops when pigment-producing cells called melanocytes start to grow out of control. The cancer has traditionally been diagnosed through visual inspection of SPLs by physicians in medical settings. Early-stage identification of SPLs can drastically improve the prognosis for patients and significantly reduce treatment costs. It is common to biopsy many lesions to ensure that every case of melanoma can be diagnosed as early as possible, thus contributing to better patient outcomes.
“Early detection of SPLs can save lives. However, the current capacity of medical systems to provide comprehensive skin screenings at scale are still lacking,” said Luis Soenksen, PhD, Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in the MIT press release.
The researchers trained their AI system by using 20,388 wide-field images from 133 patients at the Gregorio Marañón General University Hospital in Madrid, as well as publicly available images. The collected photographs were taken with a variety of ordinary smartphone cameras that are easily obtainable by consumers.
They taught the deep learning algorithm to examine various features of skin lesions such as size, circularity, and intensity. Dermatologists working with the researchers also visually classified the lesions for comparison.
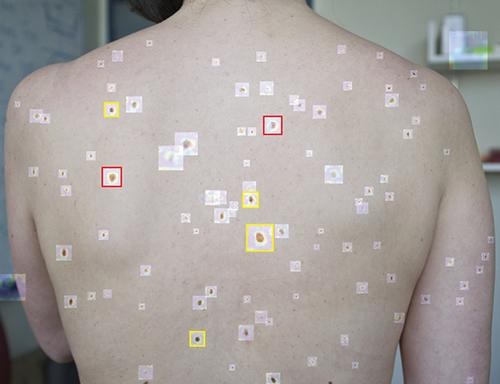
When the algorithm is “shown” a wide-field image like that above taken with a smartphone, it uses deep convolutional neural networks to analyze individual pigmented lesions and screen for early-stage melanoma. The algorithm then marks suspicious images as either yellow (meaning further inspection should be considered) or red (indicating that further inspection and/or referral to a dermatologist is required). Using this tool, dermatopathologists may be able to diagnose skin cancer and excise it in-office long before it becomes deadly. (Photo copyright: MIT.)
“Our system achieved more than 90.3% sensitivity (95% confidence interval, 90 to 90.6) and 89.9% specificity (89.6 to 90.2%) in distinguishing SPLs from nonsuspicious lesions, skin, and complex backgrounds, avoiding the need for cumbersome individual lesion imaging,” the MIT researchers noted in their Science Translational Medicine paper.
In addition, the algorithm agreed with the consensus of experienced dermatologists 88% of the time and concurred with the opinions of individual dermatologists 86% of the time, Medgadget reported.
Modern Imaging Technologies Will Advance Diagnosis of Disease
According to the American Cancer Society, about 106,110 new cases of melanoma will be diagnosed in the United States in 2021. Approximately 7,180 people are expected to die of the disease this year. Melanoma is less common than other types of skin cancer but more dangerous as it’s more likely to spread to other parts of the body if not detected and treated early.
More research is needed to substantiate the effectiveness and accuracy of this new tool before it could be used in clinical settings. However, the early research looks promising and smartphone camera technology is constantly improving. Higher resolutions would further advance development of this type of diagnostic tool.
In addition, MIT’s algorithm enables in situ examination and possible diagnosis of cancer. Therefore, a smartphone so equipped could enable a dermatologist to diagnose and excise cancerous tissue in a single visit, without the need for biopsies to be sent to a dermatopathologist.
Currently, dermatologists refer a lot of skin biopsies to dermapathologists and anatomic pathology laboratories. An accurate diagnostic tool that uses modern smartphones to characterize suspicious skin lesions could become quite popular with dermatologists and affect the flow of referrals to medical laboratories.
Hello primary diagnosis of digital pathology images via artificial intelligence! Goodbye light microscopes!
Digital pathology is poised to take a great leap forward. Within as few as 12 months, image analysis algorithms may gain regulatory clearance in the United States for use in primary diagnosis of whole-slide images (WSIs) for certain types of cancer. Such a development will be a true revolution in surgical pathology and would signal the beginning of the end of the light microscope era.
A harbinger of this new age of digital pathology and automated image analysis is a press release issued last week by Ibex Medical Analytics of Tel Aviv, Israel. The company announced that its Galen artificial intelligence (AI)-powered platform for use in the primary diagnosis of specific cancers will undergo an accelerated review by the Food and Drug Administration (FDA).
FDA’s ‘Breakthrough Device Designation’ for Pathology AI Platform
Ibex stated that “The FDA’s Breakthrough Device Designation is granted to technologies that have the potential to provide more effective treatment or diagnosis of life-threatening diseases, such as cancer. The designation enables close collaboration with, and expedited review by, the FDA, and provides formal acknowledgement of the Galen platform’s utility and potential benefit as well as the robustness of Ibex’s clinical program.”
“All surgical pathologists should recognize that, once the FDA begins to review and clear algorithms capable of using digital pathology images to make an accurate primary diagnosis of cancer, their daily work routines will be forever changed,” stated Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report. “Essentially, as FDA clearance is for use in clinical care, pathology image analysis algorithms powered by AI will put anatomic pathology on the road to total automation.
“Clinical laboratories have seen the same dynamic, with CBCs (complete blood counts) being a prime example. Through the 1970s, clinical laboratories employed substantial numbers of hematechnologists [hematechs],” he continued. “Hematechs used a light microscope to look at a smear of whole blood that was on a glass slide with a grid. The hematechs would manually count and record the number of red and white blood cells.
“That changed when in vitro diagnostics (IVD) manufacturers used the Coulter Principle and the Coulter Counter to automate counting the red and white blood cells in a sample, along with automatically calculating the differentials,” Michel explained. “Today, only clinical lab old-timers remember hematechs. Yet, the automation of CBCs eventually created more employment for medical technologists (MTs). That’s because the automated instruments needed to be operated by someone trained to understand the science and medicine involved in performing the assay.”
Primary Diagnosis of Cancer with an AI-Powered Algorithm
Surgical pathology is poised to go down a similar path. Use of a light microscope to conduct a manual review of glass slides will be supplanted by use of digital pathology images and the coming next generation of image analysis algorithms. Whether these algorithms are called machine learning, computational pathology, or artificial intelligence, the outcome is the same—eventually these algorithms will make an accurate primary diagnosis from a digital image, with comparable quality to a trained anatomic pathologist.
How much of a threat is automated analysis of digital pathology images? Computer scientist/engineer Ajit Singh, PhD, a partner at Artiman Ventures and an authority on digital pathology, believes that artificial intelligence is at the stage where it can be used for primary diagnosis for two types of common cancer: One is prostate cancer, and the other is dermatology.
On June 17, Ajit Singh, PhD (above), Partner at Artiman Ventures, will lead a special webinar and roundtable discussion for all surgical pathologists and their practice administrators on the coming arrival of artificial intelligence-powered algorithms to aid in the primary diagnosis of certain cancers. Regulatory approval for such solutions may happen by the end of this year. Such a development would accelerate the transition from light microscopes to a fully digital pathology workflow. Singh is shown above addressing the 2018 Executive War College. (Photo copyright: The Dark Report.)
“It is now possible to do a secondary read, and even a first read, in prostate cancer with an AI system alone. In cases where there may be uncertainty, a pathologist can review the images. Now, this is specifically for prostate cancer, and I think this is a tremendous positive development for diagnostic pathways,” he added.
Use of Digital Pathology with AI-Algorithms Changes Diagnostics
Pathologists who are wedded to their light microscopes will want to pay attention to the impending arrival of a fully digital pathology system, where glass slides are converted to whole-slide images and then digitized. From that point, the surgical pathologist becomes the coach and quarterback of an individual patient’s case. The pathologist guides the AI-powered image analysis algorithms. Based on the results, the pathologist then orders supplementary tests appropriate to developing a robust diagnosis and guiding therapeutic decisions for that patient’s cancer.
In his interview with The Dark Report, Singh explained that the first effective AI-powered algorithms in digital pathology will be developed for prostate cancer and skin cancer. Both types of cancer are much less complex than, say, breast cancer. Moreover, the AI developers have decades of prostate cancer and melanoma cases where the biopsies, diagnoses, and downstream patient outcomes create a rich data base from which the algorithms can be trained and tuned.
This webinar is organized as a roundtable discussion so participants can interact with the expert panelists. The Chair and Moderator is Ajit Singh, PhD, Adjunct Professor at the Stanford School of Medicine and Partner at Artiman Ventures.
The panelists (above) represent academic pathology, community hospital pathology, and the commercial sector. They are:
Because the arrival of automated analysis of digital pathology images will transform the daily routine of every surgical pathologist, it would be beneficial for all pathology groups to have one or more of their pathologists register and participate in this critical webinar.
The roundtable discussion will help them understand how quickly AI-powered image analysis is expected be cleared for use by the FDA in such diseases as prostate cancer and melanomas. Both types of cancers generate high volumes of case referrals to the nation’s pathologists, so potential for disruption to long-standing client relationships, and the possible loss of revenue for pathology groups that delay their adoption of digital pathology, can be significant.
On the flip side, community pathology groups that jump on the digital pathology bandwagon early and with the right preparation will be positioned to build stronger client relationships, increase subspecialty case referrals, and generate additional streams of revenue that boost partner compensation within their group.
Also, because so many pathologists are working remotely, Dark Daily has arranged special group rates for pathology practices that would like their surgical pathologists to participate in this important webinar and roundtable discussion on AI-powered primary diagnosis of pathology images. Inquire at info@darkreport.com or call 512-264-7103.