Federal prosecutors allege that this nurse practitioner ordered more genetic tests for Medicare beneficiaries than any other provider during 2020
Cases of Medicare fraud involving clinical laboratory testing continue to be prosecuted by the federal Department of Justice. A jury in Miami recently convicted a nurse practitioner (NP) for her role in a massive Medicare fraud scheme for millions of dollars in medically unnecessary genetic testing and durable medical equipment. She faces 75 years in prison when sentenced in December.
In their indictment, federal prosecutors alleged that from August 2018 through June 2021 Elizabeth Mercedes Hernandez, NP, of Homestead, Florida, worked with more than eight telemedicine and marketing companies to sign “thousands of orders for medically unnecessary orthotic braces and genetic tests, resulting in fraudulent Medicare billings in excess of $200 million,” according to a US Department of Justice (DOJ) news release announcing the conviction.
“Hernandez personally pocketed approximately $1.6 million in the scheme, which she used to purchase expensive cars, jewelry, home renovations, and travel,” the press release noted.
Hernandez was indicted in April 2022 as part of a larger DOJ crackdown on healthcare fraud related to the COVID-19 outbreak.
“Throughout the pandemic, we have seen trusted medical professionals orchestrate and carry out egregious crimes against their patients all for financial gain,” said Assistant Director Luis Quesada (above) of the FBI’s Criminal Investigative Division, in a DOJ press release. Clinical laboratory managers would be wise to monitor these Medicare fraud cases. (Photo copyright: Federal Bureau of Investigation.)
Nurse Practitioner Received Kickbacks and Bribes
Federal prosecutors alleged that the scheme involved telemarketing companies that contacted Medicare beneficiaries and persuaded them to request genetic tests and orthotic braces. Hernandez, they said, then signed pre-filled orders, “attesting that she had examined or treated the patients,” according to the DOJ news release.
In many cases, Hernandez had not even spoken with the patients, prosecutors said. “She then billed Medicare as though she were conducting complex office visits with these patients, and routinely billed more than 24 hours of ‘office visits’ in a single day,” according to the news release.
In total, Hernandez submitted fraudulent claims of approximately $119 million for genetic tests, the indictment stated. “In 2020, Hernandez ordered more cancer genetic (CGx) tests for Medicare beneficiaries than any other provider in the nation, including oncologists and geneticists,” according to the news release.
The indictment noted that because CGx tests do not diagnose cancer, Medicare covers them only “in limited circumstances, such as when a beneficiary had cancer and the beneficiary’s treating physician deemed such testing necessary for the beneficiary’s treatment of that cancer. Medicare did not cover CGx testing for beneficiaries who did not have cancer or lacked symptoms of cancer.”
In exchange for signing the orders, Hernandez received kickbacks and bribes from companies that claimed to be in the telemedicine business, the indictment stated.
“These healthcare fraud abuses erode the integrity and trust patients have with those in the healthcare industry … the FBI, working in coordination with our law enforcement partners, will continue to investigate and pursue those who exploit the integrity of the healthcare industry for profit,” said Assistant Director Luis Quesada of the Federal Bureau of Investigation’s Criminal Investigative Division, in the DOJ press release.
Conspirators Took Advantage of COVID-19 Pandemic
Prosecutors alleged that as part of the scheme, she and her co-conspirators took advantage of temporary amendments to rules involving telehealth services—changes that were enacted by Medicare in response to the COVID-19 pandemic.
The indictment noted that prior to the pandemic, Medicare covered expenses for telehealth services only if the beneficiary “was located in a rural or health professional shortage area,” and “was in a practitioner’s office or a specified medical facility—not at a beneficiary’s home.”
But in response to the pandemic, Medicare relaxed the restrictions to allow coverage “even if the beneficiary was not located in a rural area or a health professional shortage area, and even if the telehealth services were furnished to beneficiaries in their home.”
Hernandez was convicted of:
One count of conspiracy to commit healthcare fraud and wire fraud.
Four counts of healthcare fraud.
Three counts of making false statements.
Medscape noted that she was acquitted of two counts of healthcare fraud. The trial lasted six days, Medscape reported.
Hernandez’s sentencing hearing is scheduled for Dec. 14.
Co-Conspirators Plead Guilty
Two other co-conspirators in the case, Leonel Palatnik and Michael Stein, had previously pleaded guilty and received sentences, the Miami Herald reported.
Palatnik was co-owner of Panda Conservation Group LLC, which operated two genetic testing laboratories in Florida. Prosecutors said that Palatnik paid kickbacks to Stein, owner of 1523 Holdings LLC, “in exchange for his work arranging for telemedicine providers to authorize genetic testing orders for Panda’s laboratories,” according to a DOJ press release. The kickbacks were disguised as payments for information technology (IT) and consulting services.
“1523 Holdings then exploited temporary amendments to telehealth restrictions enacted during the pandemic by offering telehealth providers access to Medicare beneficiaries for whom they could bill consultations,” the press release states. “In exchange, these providers agreed to refer beneficiaries to Panda’s laboratories for expensive and medically unnecessary cancer and cardiovascular genetic testing.”
Palatnik pleaded guilty to his role in the kickback scheme in August 2021 and was sentenced to 82 months in prison, a DOJ press release states.
Stein pleaded guilty in April and was sentenced to five years in prison, the Miami Herald reported. He was also ordered to pay $63.3 million in restitution.
These federal cases involving clinical laboratory genetic testing and other tests and medical equipment indicate a commitment on the DOJ’s part to continue cracking down on healthcare fraud.
This fourth edition of the annual event will be held virtually with free registration for pathologists and clinical laboratory professionals
In its fourth year, stakeholders in the clinical laboratory community have promoted thought leadership around the Lab Industry at the Project Santa Fe Foundation’s Clinical Lab 2.0 Workshop. Clinical Lab 2.0 (CL 2.0) which identifies new opportunities for medical labs to add value as the healthcare industry transitions from fee-for-service to value-based delivery models. But how does this concept apply during the era of COVID-19? That’s a key question participants will discuss at the 2020 Clinical Lab 2.0 Workshop, a virtual event scheduled for Oct. 26-27 with a focus on Population Health.
“This workshop will help all clinical laboratory leaders and pathologists to better understand, ‘How do we manage a pandemic, identifying high risk pool, where are the care gaps, and how do we better manage in the future proactively?’” said Khosrow Shotorbani, MBA, MT (ASCP), co-founder of the CL2.0 initiative and a regular speaker at the Executive War College, in an exclusive interview with Dark Daily. He is President and Executive Director of the Project Santa Fe Foundation, the organization that promotes the Clinical 2.0 Movement.
The coronavirus pandemic has “truly elevated the value of the clinical laboratory and diagnostics as one essential component of the care continuum,” he noted. “The value of the SARS-CoV-2 test became immense, globally, and the mantra became ‘test to trace to treat.’”
Project Santa Fe Foundation’s website defines Clinical Laboratory 2.0 as an effort to demonstrate “the power of longitudinal clinical lab data to proactively augment population health in a value-based healthcare environment.” The “goals are to improve the clinical outcomes of populations, help manage population risk, and reduce the overall cost of delivering healthcare,” the CL 2.0 website states.
“It’s about harnessing lab test results and other data that have predictive value and can help us proactively identify individuals that need care,” explained Shotorbani. “In the context of population health or value-based care, our labs potentially can utilize the power of this data to risk-stratify a population for which we are responsible or we can identify gaps in care.”
Clinical Lab 2.0 and the SARS-CoV-2 Pandemic
In the context of COVID-19, “Clinical Lab 2.0 argues that there is a hidden universe of value that can help augment what happens between COVID-19 testing and COVID-19 tracing to convert this reactive approach—meaning we wait for the person to get ill—versus considering who may be most at risk if they were to become infected so that our clinical laboratories can help caregivers create proactive isolation or quarantine strategies,” he added.
Shotorbani then explained how clinical laboratories have data about comorbidities such as diabetes, asthma, heart disease, and immunosuppression that are associated with more serious cases of COVID-19. “This clinical lab data can be harnessed, associated with demographic and risk data such as age and zip codes to help physicians and others identify patients who would be most at risk from a COVID-19 infection,” he noted.
“Historically, the primary focus of a clinical laboratory was very much on the clinical intervention, contacting the care manager physician, and identifying who’s at risk,” he said. But with COVID-19, Shotorbani sees opportunities to forge relationships with public health specialists to encourage what he describes as “consumer engagement.”
“As medical laboratory professionals, we must evolve to accommodate and support the needs of consumers as they take a more active role in their health,” he continued. “This is moving past simply providing lab test results, but to then be a useful diagnostic and therapeutic resource that helps consumers understand their health conditions and what the best next steps are to manage those conditions.”
Khosrow Shotorbani (above) is President, Executive Director, of the Project Santa Fe Foundation and one of the leaders of the Clinical Laboratory 2.0 movement. He is hopeful that the prominent role of medical laboratories in responding to the coronavirus pandemic will lead to an ongoing “seat at the table” in the higher echelons of healthcare organizations. In normal times, “we reside in basements, and we’re done when we release a result,” he said during an exclusive interview with Dark Daily. “COVID-19 was a kick in the rear to get us upstairs to the C-suite, because healthcare CEOs are under the gun to demonstrate more SARS-CoV-2 testing capacity.” Looking ahead, “we want to make sure that our clinical laboratories stay in that seat and design a future delivery model above and beyond COVID-19, maybe even help health systems, hospitals, and other providers drive their strategies.” (Photo copyright: Albuquerque Business First.)
“None of these are pathologists or come from the lab,” Shotorbani said. “They represent the C-suite and higher organization constituents. These are the healthcare executives who are dealing with their organization’s pain points. As clinical labs, we want to align ourselves to those organizational objectives.”
Pathologist Mark Fung, MD, PhD, will then present a CL 2.0 model for managing COVID-19 or other infectious disease pandemics, followed by a response from the other panelists. Fung is Vice Chair for Population Health in the Department of Pathology and Laboratory Medicine at the Larner College of Medicine at the University of Vermont. He is also on the Project Santa Fe Foundation (PSFF) board of directors.
“Lab 2.0 is a thought leadership organization,” Shotorbani said. “We are developing a template and abstract of this model of clinical laboratory services that other labs can follow while applying some of their own intuition as they make it operational.”
Day Two to the CL 2.0 workshop will feature case studies from the Henry Ford Health System in Detroit and Geisinger Health in Danville, Pa., followed by a discussion with eight PSFF directors. Then, Beth Bailey of TriCore Reference Laboratories in Albuquerque, N.M., will preside over a crowdsourcing session with participation from audience members.
Free Registration for Clinical Laboratories
This will be the first Clinical Lab 2.0 Workshop to be held virtually and registration this year will be free for members of the clinical laboratory community, Shotorbani said. In the past “there has been a hefty tuition to get into this because it’s a very high-touch workshop, especially for senior leaders. But given the critical topic that we’re facing, we felt it was important to waive the cost.”
The Fourth Annual Clinical Lab 2.0 Workshop is partnering this year with the American Society for Clinical Pathology (ASCP), which will provide the software platform for hosting the event, he said. In addition to the live conference sessions, registrants will have access to prerecorded presentations from past workshops. Content will be viewable for six months following the event.
Register for this critical event by clicking here, or by placing this URL in your browser (https://projectsantafefoundation.regfox.com/clinical-lab-20-workshop).
A former officer of a Cigna contractor claims the insurer hatched a scheme to submit invalid diagnostic codes and filed the now-unsealed qui tam action in 2017
In a case that could provide a cautionary tale for clinical laboratories, a federal whistleblower lawsuit alleges that Cigna, through its HealthSpring subsidiary, “received billions in overpayments from the federal government” in a scheme involving the insurer’s Medicare Advantage plans. The Qui tam (whistleblower) lawsuit was filed by Robert A. Cutler, a former officer of Cigna contractor Texas Health Management LLC (THM), under the federal False Claims Act.
Cutler alleged that “Cigna-HealthSpring has knowingly defrauded the United States through an intentional and systematic pattern and practice of submitting to CMS invalid diagnosis codes derived from in-home health assessments.” He claimed this took place “from at least 2012 until at least 2017,” and likely thereafter.
Cigna has denied the allegations. “We are proud of our industry-leading Medicare Advantage program and the manner in which we conduct our business,” the insurer stated in an email to HealthPayerIntelligence. “We will vigorously defend Cigna against all unjustified allegations,” Cigna stated.
As the lawsuit explains, Medicare Advantage (MA) plans are administered by private insurers under Medicare Part C. “Rather than pay providers directly based on the medical services provided, Medicare Part C pays MA Organizations a monthly capitated rate for each covered beneficiary, and tasks the MA Plan with paying providers for services rendered to plan members,” the lawsuit states. “MA insurers are generally paid more for providing benefits to beneficiaries with higher-risk scores—generally older and sicker people—and less for beneficiaries with lower-risk scores, who tend to be younger and healthier.”
The lawsuit notes that CMS relies on information—specifically ICD codes—from the insurers to calculate the risk scores.
Cigna’s 360 Program as Described in Lawsuit
Cutler alleged that Cigna defrauded CMS through its “360 Program,” in which primary care providers (PCPs) were encouraged to perform enhanced annual wellness visits that included routine physical exams. He claimed that “Cigna-HealthSpring designed the program so that, in practice, the 360 assessment was a mere data-gathering exercise used to improperly record lucrative diagnoses to fraudulently raise risk scores and increase payments from CMS.”
Cigna-HealthSpring, he alleged in the court documents, offered PCPs financial bonuses to perform the 360 program exams, especially on patients deemed most likely to yield high-risk scores. However, many clinicians declined, so the insurer recruited third-party contract providers, including THM, to send nurse practitioners (NPs) or registered nurses (RNs) to the homes of MA plan members.
For each visit, the NPs and RNs were given health reports listing the beneficiary’s previous diagnoses. “Cigna-HealthSpring intended the document to serve as a ‘cheat-sheet’ list of conditions and diagnoses it expected 360 contractors to capture during the in-home visit,” Cutler alleges. “The list of diagnoses did not indicate the date they were reported or any other information concerning their status.”
During each visit, which typically lasted 30-60 minutes, “NPs and RNs relied primarily on the patient’s self-assessment, i.e., subjectively reported information, as well as current medications to the extent available and, during certain time periods and for certain plan members, limited [clinical] laboratory findings,” Cutler alleged.
NPs were expected to record 20 or more diagnoses per visit, he wrote, including diagnoses based on “weak links” involving medications. “For example, Cigna-HealthSpring encouraged contractors to record atrial fibrillation, deep vein thrombosis, and pulmonary embolus based on the presence of certain classes of anti-coagulation medications on members’ medication lists or in their homes,” he stated.
He also alleged that “Cigna-HealthSpring, in purposeful violation of CMS rules, designed its 360 form to force NPs to capture diagnoses that were uncertain, probable, or merely suspected.”
These diagnoses were subsequently submitted as risk-adjustment data to CMS, he alleged, adding up to “hundreds of thousands of false claims from its six contractors during the relevant period. Although the exact amount will be proven at trial, the United States has paid billions of dollars in improper, inflated payments to Defendants under the MA Plan as a result of this scheme.”
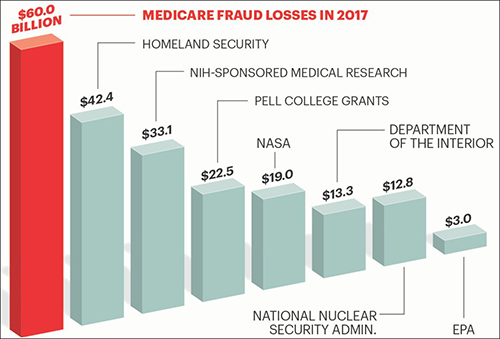
The graphic above is taken from an AARP article, titled, “Medicare Under Assault from Fraudsters,” which states, “The amount of tax dollars that are lost each year to Medicare fraud and waste is greater than the entire annual budget of some of the federal government’s most important programs and departments.” Clinical laboratories also are in danger of being drawn into the federal government’s fraud investigations which can be disruptive to business and revenues. (Graphic copyright: AARP.)
The Federal False Claims Act “allows a private citizen to step into the shoes of and pursue a claim on behalf of the government,” explained the Boyers Law Group of Coral Gables, Fla., in an article for HG.org, which states, the lawsuit “may proceed with or without the assistance of the government.”
If the government chooses to intervene, the whistleblower, known formally as the “relator,” can receive 15% to 25% of the proceeds recovered in the action, the law firm explained in another article for HG.org, adding that, in most cases, the government does not intervene, which increases the potential award to 30%.
In the Cigna case, the US Attorney’s office notified the court on Feb. 25, 2020, that the government had decided not to intervene “at this time.”
Significance for Clinical Laboratories
Regardless of how this case proceeds, medical laboratory managers should remember that they are subject to legal action if internal whistleblowers identify policies or procedures that violate federal fraud and abuse laws. And because it involves coding, it is also a reminder of the importance of documenting diagnoses and clinical laboratory test orders as protection against fraud allegations.
Another benefit of carefully documenting each lab test order is that labs can make the information available when auditors from government or private payers show up and want documentation on the medical necessity of each lab test claim.
Although most clinical laboratories and pathology groups do not use EHR systems, the OIG’s finding should alert them to possible problems with audit integrity of their clients’ EHRs
Electronic Health Record (EHR) systems were supposed to prevent fraud, but a recent report from one federal agency states that the fraud safeguards built into EHR systems are not in engaged by a majority of users.
Issue does not directly affect clinical laboratories and pathology groups, but puts spotlight on some hospitals and physicians who frequently use these codes.
Could increased use of electronic health records (EHR) systems be causing more hospitals and physicians to commit fraud because of upcoding? That’s the assertion of certain federal health officials. They attribute the increased proportion of Medicare claims for more complex and more expensive services by some providers to be, in some part, acts of fraud.
Most pathologists and clinical laboratory managers will notice the irony in these allegations that providers are upcoding services to Medicare patients in fraudulent ways. After all, the federal government is currently paying billions of dollars in financial incentives to encourage providers to implement and use certified EHR systems with the goal of lowering healthcare costs, while improving patient outcomes.
OIG Audit Findings Are Source of Fraud Allegations
Insinuations of provider fraud came after the public learned of findings of an audit done by Health and Human Services’ Office of Inspector General (OIG). The OIG determined that payments for more complex Level 5 E/M services increased by 21% between 2001 and 2010. During that same period, payments for medium-complexity patient services decreased by 11%.
For all of 2010, the Centers for Medicare and Medicaid Services (CMS) paid out $33.5 billion for E/M billings. This was about one-third of Medicare Part B payments for physician services. These numbers were part of a story published in Modern Healthcare.
Now that much larger numbers of physicians and hospitals are using electronic health record (EHR) systems, Medicare has noticed a steady increase in the proportion of claims submitted at higher and more complex codes, increasing reimbursement. In response to one federal government audit, Kathleen Sebellius, Secretary of Health and Human Services (r) and Attorney General Eric Holder (l) held a joint press conference to announce to healthcare providers that there would be stricter audits of providers who are using billing codes for complex patient visits with greater frequency. (Photo by Manuel Balce Ceneta, copyright Associated Press.)