Medical laboratories and anatomic pathologists may need to squeeze into narrow networks to be paid under value-based schemes, especially where Medicare Advantage is concerned
Pathologists have likely heard the arguments in favor of value-based payment versus fee-for-service (FFS) reimbursement models: FFS encourages providers to order medically unnecessary procedures and lab tests. FFS removes incentives for providers to order patient services more carefully. Fraudsters can generate huge volumes of FFS claims that take payers months/years to recognize and stop.
Studies that favor value-based payment schemes support these claims. But do hospitals and other healthcare providers also accept them? And how is value-based reimbursement really doing?
To find out, Chicago-based thought leadership and advisory company 4Sight Health culled data from various organizations’ reports that suggest value-based reimbursement shows signs of growth as well as signs of stagnation.
Value-Based Payment Has Its Ups and Downs
Healthcare journalist David Burda is News Editor and Columnist at 4Sight Health. In his article, “Is Value-Based Reimbursement Mostly Dead or Slightly Alive?” Burda commented on data from various industry reports that indicated value-based reimbursement shows “signs of life.” For example:
More doctors are accepting pay-for-performance payments: 44.5% in 2020, up from 42.3% in 2018, according to an American Medical Association (AMA) biennial report on physician participation in value-based reimbursement, titled, “Policy Research Perspectives: Payment and Delivery in 2020.”
On the other hand, Burda reported that value-based reimbursement also has these declining indicators:
39.3% of provider payments “flowed” through FFS plans in 2020 with no link to cost or quality. This was unchanged since 2019. (HCPLAN report)
19.8% of FFS payments to providers in 2020 were linked to cost or quality, down from 22.5% in 2019. (HCPLAN report)
88% of doctors reported accepting FFS payments in 2019, an increase from 87% in 2018. (AMA report)
Does Today’s Healthcare Industry Support Value-based Care?
A survey of 680 physicians conducted by the Deloitte Center for Health Solutions suggests the answer could be “not yet.” In “Equipping Physicians for Value-Based Care,” Deloitte reported:
“Physician compensation continues to emphasize volume more than value.
“Availability and use of data-driven tools to support physicians in practicing value-based care continue to lag.
“Existing care models do not support value-based care.”
Deloitte analysts wrote, “Physicians increasingly recognize their role in improving the affordability of care. We repeated a question we asked six years ago and saw a large increase in the proportion of physicians who say they have a prominent role in limiting the use of unnecessary treatments and tests: 76% in 2020 vs. 57% in 2014.
“Physicians also recognize that today’s care models are not geared toward value,” Deloitte continued. “They see many untapped opportunities for improving quality and efficiency. They estimate that even today, sizable portions of their work can be performed by nonphysicians (30%) in nontraditional settings (30%) and/or can be automated (18%), creating opportunities for multidisciplinary care teams and clinicians to work at the top of their license.”
Hospital CFOs Also See Opportunities for Value-based Care
This could be problematic for clinical laboratories, according to Robert Michel, Editor-in-Chief of Dark Daily and our sister publication The Dark Report. According to Guidehouse, “Nearly 60% of health systems plan to advance into risk-based Medicare Advantage models in 2022.”
Medicare Advantage (MA) enrollments have escalated over 10 years: 26.4 million people of the 62.7 million eligible for Medicare chose MA in 2021, noted a Kaiser Family Foundation brief that also noted MA enrollment in 2021 was up by 2.4 million beneficiaries or 10% over 2020.
The graph above is taken from the Kaiser Family Foundation report, “Medicare Advantage in 2021: Enrollment Update and Key Trends.” According to the KFF, “In 2021, more than four in 10 (42%) Medicare beneficiaries—26.4 million people out of 62.7 million Medicare beneficiaries overall—are enrolled in Medicare Advantage plans; this share has steadily increased over time since the early 2000s.” Since MA employs narrow networks for its healthcare providers, it’s likely this trend will continue to affect clinical laboratories that may find it difficult to access these providers. (Graphic copyright: Kaiser Family Foundation.)
“The shift from Medicare Part B—where any lab can bill Medicare on behalf of patients for doctor visits and outpatient care, including lab tests—to Medicare Advantage is a serious financial threat for smaller and regional labs that do a lot of Medicare Part B testing. The Medicare Advantage plans often have networks that exclude all but a handful of clinical laboratories as contracted providers,” Michel cautioned. “Moving into the future, it’s incumbent on regional and smaller clinical laboratories to develop value-added services that solve health plans’ pain points and encourage insurers to include local labs in their networks.”
Medical laboratories and anatomic pathology groups need to be aware of this trend. Michel says value-based care programs call on clinical laboratories to collaborate with healthcare partners toward goals of closing care gaps.
“Physicians and hospitals in a value-based environment need a different level of service and professional consultation from the lab and pathology group because they are being incented to detect disease earlier and be active in managing patients with chronic conditions to keep them healthy and out of the hospital,” he added.
Value-based reimbursement may eventually replace fee-for-service contracts. The change, however, is slow and clinical laboratories should monitor for opportunities and potential pitfalls the new payment arrangements might bring.
In an out-of-court settlement, two commercial clinical laboratory companies also agreed to reduce their prices for rapid antigen tests as well
How clinical laboratory companies were pricing their COVID-19 tests caught the attention of government authorities in South Africa. Government agencies in that country are establishing what they view as fair clinical laboratory pricing for private COVID-19 PCR (polymerase chain reaction) and rapid antigen tests without turning to litigation or fines.
The Competition Commission (Commission) is an organization charged with reviewing and acting on business practices in South Africa. In a December 11, 2021, news release, the Commission said it had reached a “ground-breaking agreement” with two private laboratories—Ampath and Lancet—to reduce their COVID-19 PCR test prices from 850 South African rand (R850) to R500 (from US$54.43 to US$31.97).
As of December 12, a third private laboratory company that also had been investigated, PathCare, had not agreed to the court settlement, Daily Maverick reported.
Also effective are lower prices for rapid antigen tests, the Commission said in a separate December 23 news release.
COVID Test Prices ‘Unfairly Inflated’
The changes in PCR test prices in South Africa followed a formal complaint by the Council for Medical Schemes which alleged the private pathology labs [the term for clinical laboratories in South Africa] were “supplying” COVID-19 PCR tests at “unfairly inflated, exorbitant, and/or unjustifiable” prices, Daily Maverick reported.
The clinical laboratory companies “exploited consumers by earning excessive profits on essential products or services,” Tembinkosi Bonakele (above), Commissioner of the South Africa Competition Commission, told the Daily Maverick. “It is always encouraging for companies to voluntarily consider reducing prices, especially where the public is detrimentally affected by the prices, as to avoid protracted litigation,” he added. (Photo copyright: Sowetan Live.)
According to the Daily Maverick, as part of the investigation, which began in October 2021, the Commission asked the private clinical laboratory companies for financial statements and costs of COVID-19 testing.
“We did, then, further interrogation in order to strip out what we saw was potentially padding the costing and unrelated costs. And on the basis of that, we came to the figure of R500,” James Hodge, told the Daily Maverick. Hodge is Chief Economist, Economic Research Bureau, and Acting Deputy Commissioner at the Competition Commission South Africa.
For its part, Lancet, Johannesburg, said in a statement that it “Appreciates the spirit of constructive engagement with the Commission which has resulted in an outcome that best serves the people of South Africa as they confront the fourth COVID wave. We are sensitive to the plight of the public and agree that reducing the COVID-19 PCR price is in best national interest.”
Clinical Laboratory Test Prices: Market Dynamics
So, were the prices too high? In the US, clinical laboratories are reimbursed considerably more by Medicare for COVID-19 testing (about $100), as compared to the South Africa private clinical lab prices.
Also, the Centers for Medicare and Medicaid Services (CMS) said in a statement that effective January 2021 it included in that rate an incentive of $25 to labs that provide results within 48 hours.
Medical laboratories are reimbursed $75 for a high throughput COVID-19 test when results are reported beyond 48 hours, CMS added.
Antigen Tests Prices Also Reduced
The Commission said that during its review of COVID-19 PCR test pricing it received a Department of Health Republic of South Africa complaint about prices for rapid antigen test pricing as well.
After another Commission review, PathCare, Lancet, and Ampath agreed to reduce prices for rapid antigen tests to a maximum of R150 or $9.74 (from a range of R250 to R350 or $16.28 to $22.79), a news release noted.
“The reduction of COVID-19 rapid antigen test prices will help alleviate the plight of consumers and widen accessibility and affordability of COVID-19 rapid antigen testing, which is a critical part of the initiatives to avoid escalation of the pandemic,” said Bonakele in the news release, which also stated that the Commission would receive financial statements from the three labs every few months.
The Commission also is reviewing a “large retail pharmacy chain’s” rapid antigen prices, which “follows a complaint lodged by the Department of Health (DOH), on December 14 2021, against service providers delivering COVID-19 Rapid Antigen tests in South Africa to consumers,” Cape Town Etc reported. The specific pharmacy chain was not identified.
Data Show COVID Plight in South Africa
More than 21.6 million COVID-19 tests have been offered by healthcare providers in South Africa, and 3.5 million cases were detected, according to the Department of Health, Republic of South Africa.
Considering those data, one wonders if the South African government acted fast enough on test pricing.
For medical laboratory leaders, it’s important to recognize that not only are lab services in the spotlight during the COVID-19 pandemic, business practices and prices also are being monitored by officials in this country.
Though the new technology could speed diagnoses of cancers and other skin diseases, it would also greatly reduce dermatopathology biopsy referrals and revenue
What effect would elimination of tissue biopsies have on dermatopathology and clinical laboratory revenue? Quite a lot. Dermatologists alone account for a significant portion of skin biopsies sent to dermatopathologists. Thus, any new technology that can “eliminate the need for invasive skin biopsies” would greatly reduce the number of histopathological referrals and reduce revenue to those practices.
“What if we could entirely bypass the biopsy process and perform histology-quality staining without taking tissue and processing tissue in a noninvasive way? Can we create images that diagnosticians can benefit from?” asked Aydogan Ozcan, PhD (above), Chancellor’s Professor of Electrical and Computer Engineering at UCLA’s Samueli School of Engineering, one of the scientists who developed UCLA’s new virtual histology method, during an interview with Medical Device + Diagnostic Industry (MD+DI). (Photo copyright: Nature.)
Could Skin Biopsies be Eliminated?
The UCLA researchers believe their innovative deep learning-enabled imaging framework could possibly circumvent the need for skin biopsies to diagnose skin conditions.
“Here, we present a deep learning-based framework that uses a convolutional neural network to rapidly transform in vivo RCM images of unstained skin into virtually-stained hematoxylin and eosin-like images with microscopic resolution, enabling visualization of the epidermis, dermal-epidermal junction, and superficial dermis layers.
“This application of deep learning-based virtual staining to noninvasive imaging technologies may permit more rapid diagnoses of malignant skin neoplasms and reduce invasive skin biopsies,” the researchers added in their published study.
According to the published study, the UCLA team trained their neural network under an adversarial machine learning scheme to transform grayscale RCM images into virtually stained 3D microscopic images of normal skin, basal cell carcinoma, and pigmented melanocytic nevi. The new images displayed similar morphological features to those shown with the widely used hematoxylin and eosin (H&E) staining method.
“In our studies, the virtually stained images showed similar color contrast and spatial features found in traditionally stained microscopic images of biopsied tissue,” Ozcan told Photonics Media. “This approach may allow diagnosticians to see the overall histological features of intact skin without invasive skin biopsies or the time-consuming work of chemical processing and labeling of tissue.”
The framework covers different skin layers, including the epidermis, dermal-epidermis, and superficial dermis layers. It images deeper into tissue without being invasive and can be quickly performed.
“The virtual stain technology can be streamlined to be almost semi real time,” Ozcan told Medical Device + Diagnostic Industry (MD+DI). “You can have the virtual staining ready when the patient is wrapping up. Basically, it can be within a couple of minutes after you’re done with the entire imaging.”
Currently, medical professionals rely on invasive skin biopsies and histopathological evaluations to diagnose skin diseases and cancers. These diagnostic techniques can result in unnecessary biopsies, scarring, multiple patient visits and increased medical costs for patients, insurers, and the healthcare system.
Improving Time to Diagnosis through Digital Pathology
Another advantage of this virtual technology, the UCLA researchers claim, is that it can provide better images than traditional staining methods, which could improve the ability to diagnose pathological skin conditions and help alleviate human error.
“The majority of the time, small laboratories have a lot of problems with consistency because they don’t use the best equipment to cut, process, and stain tissue,” dermatopathologist Philip Scumpia, MD, PhD, Assistant Professor of Dermatology and Dermatopathology at UCLA Health and one of the authors of the research paper, told MD+DI.
“What ends up happening is we get tissue on a histology slide that’s basically unevenly stained, unevenly put on the microscope, and it gets distorted,” he added, noting that this makes it very hard to make a diagnosis.
Scumpia also added that this new technology would allow digital images to be sent directly to the pathologist, which could reduce processing and laboratory times.
“With electronic medical records now and the ability to do digital photography and digital mole mapping, where you can obtain a whole-body imaging of patients, you could imagine you can also use one of these reflectance confocal devices. And you can take that image from there, add it to the EMR with the virtual histology stain, which will make the images more useful,” Scumpia said. “So now, you can track lesions as they develop.
“What’s really exciting too, is that there’s the potential to combine it with other artificial intelligence, other machine learning techniques that can give more information,” Scumpia added. “Using the reflectance confocal microscope, a clinician who might not be as familiar in dermatopathology could take images and send [them] to a practitioner who could give a more expert diagnosis.”
Faster Diagnoses but Reduced Revenue for Dermatopathologists, Clinical Labs
Ozcan noted that there’s still a lot of work to be done in the clinical assessment, validation, and blind testing of their AI-based staining method. But he hopes the technology can be propelled into a useful tool for clinicians.
“I think this is a proof-of-concept work, and we’re very excited to make it move forward with further advances in technology, in the ways that we acquire 3D information [and] train our neural networks for better and faster virtual staining output,” he told MD+DI.
Though this new technology may reduce the need for invasive biopsies and expedite the diagnosis of skin conditions and cancers—thus improving patient outcomes—what affect might it have on dermatopathology practices?
More research and clinical studies are needed before this new technology becomes part of the diagnosis and treatment processes for skin conditions. Nevertheless, should virtual histology become popular and viable, it could greatly impact the amount of skin biopsy referrals to pathologists, dermatopathologists, and clinical laboratories, thus diminishing a great portion of their revenue.
Former CEO also testified that she believed company’s proprietary blood-testing technology could perform ‘any’ clinical laboratory blood test
One relevant question in the federal fraud trial of ex-Theranos CEO Elizabeth Holmes was whether she would testify on her own behalf. That question was answered shortly after the government rested its criminal fraud case against the former Silicon Valley clinical laboratory testing company founder. Holmes took the stand in her own defense, a risk her defense team hopes will pay off in her favor.
During her first three days of testimony leading up to the Thanksgiving holiday break, Holmes—who faces 11 counts of fraud and conspiracy related to her tenure as founder and CEO of Theranos—made headlines by admitting she did personally put the logos of pharmaceutical giants Pfizer and Schering-Plough on reports she sent to Theranos investors and executives at Walgreens and Safeway. She expressed regret for doing so to the jury, but claimed her intent was not to deceive but to give credit to others.
“This work was done in partnership with these companies, and I was trying to convey that,” she testified, according to a trial coverage from Ars Technica.
When asked if she realized that others would assume the pharmaceutical companies—not Theranos—were the authors of the report, Holmes replied, “I’ve heard that testimony in this case, and I wish I’d done it differently.”
If found guilty, Holmes—who once claimed Theranos’ Edison proprietary blood-testing technology would to be able to complete as many as 200 clinical laboratory tests using a single finger-stick of blood—could face maximum penalties of 20 years in prison, a $2.75 million fine, and possible restitution.
The illustration above depicts ex-Theranos CEO Elizabeth Holmes testifying on her own behalf. Former Santa Clara County prosecutor Steven Clark, JD, told The Mercury News, “(T)he best person to say what Elizabeth Holmes’ intent was is Elizabeth Holmes, and that’s why I think she’s taking the stand. … I think the jury will like her.” That remains to be seen. But there’s no doubt that Clinical Laboratory Directors should take a strong interest in the outcome of this trail. (Graphic copyright: Vicki Behringer/Reuters.)
Holmes Testifies She Believed the Edison Device Could Perform “Any” Blood Test
In its trail coverage, NPR described Holmes’ first three days of testimony “as having involved deflecting responsibility, pointing to the expertise of the Theranos board of directors, lab staff, and other company employees whom Holmes has suggested were close to how [Theranos’] blood analyzers worked.”
According to Reuters, Holmes’ defense team is arguing that Holmes’ always-rosy forecasts about her company’s technology and finances were based on her belief the proprietary Edison device worked as advertised, which, in turn, was based on feedback from pharmaceutical companies, her own employees, and the military.
During her testimony, Holmes compared a traditional blood-testing device to Theranos’ “3.0” device, which she said would reduce the human-error rate that can occur during blood sampling.
“If we had the ability to automate much of that process, we could reduce the error associated with traditional lab testing,” she told the court.
Reuters reported that Holmes told jurors her confidence in the Theranos device was in part due to how well the unit had performed in studies completed in 2008 and 2009, including those run by drug companies such as Novartis.
The Mercury News described Holmes as speaking with “confidence—and frequently a small smile”—during her opening day of testimony.
Asked by one of her lawyers, “Did you believe that Theranos had developed technology that was capable of performing any blood test?” Holmes responded, “I did.”
Holmes Testifies about Military’s Alleged Use of Edison Device
Prosecutors maintain that Holmes knew Theranos’ proprietary blood-testing technology had serious accuracy issues yet lied about its capabilities and use to lure investors. One of those false claims included allegedly stating the US military was using the Edison device on the battlefield. Earlier in the trial, CNBC reported, prosecution witness Brian Grossman, Chief Investment Officer at PFM Health Sciences, which invested $96 million into Theranos, testified he was told in a 2013 meeting with Holmes and Balwani that Theranos technology was being used in medical-evacuation helicopters.
However, on the witness stand, Holmes described Theranos’ projects with the US military as much more limited in scope than the descriptions outlined by investors testifying for the prosecution.
According to The Wall Street Journal (WSJ), Holmes told jurors a 2010 partnership between Theranos and a US Army Institute of Surgical Research doctor in Texas looked into using the Theranos device to measure blood markers to detect kidney performance. A second project involved the military’s Africa Command, which was determining whether the device could withstand high temperatures. Holmes testified the devices used in Africa “held up well,” though some modifications were needed, and some issues were revealed with the touchscreen.
Should Holmes Have Testified on Her Own Behalf?
Trial experts maintain Holmes’ decision to testify in her own defense could backfire.
“It’s always a risk to put your client on because if they make a mistake they can sink the whole case,” former Santa Clara County prosecutor Steven Clark, JD, told The Mercury News. He added, “what’s at issue here is Elizabeth Holmes’ intent. And the best person to say what Elizabeth Holmes’ intent was is Elizabeth Holmes, and that’s why I think she’s taking the stand. She’s very charismatic. She’s really good on her feet. And I think the jury will like her.
“This is the pitch meeting of her life,” Clark added. “She’s going to be explaining herself to 12 people as to what was in her mind.”
Judge Drops One Count Due to Prosecution Error, Government Rests Its Case
Holmes is now charged with nine counts of wire fraud and two counts of conspiracy to commit wire fraud after the government dropped one count of fraud from the indictment. According to WSJ coverage of the trial, US District Judge Edward Davila blocked a patient named in the indictment as “B.B.” from testifying because of a filing error by the prosecution. The judge’s decision resulted in the government dropping one count.
The government rested its case against Holmes on November 19 following testimony from independent journalist Roger Parloff, who wrote a flattering 2014 Fortune magazine story on Holmes. He later redacted his earlier writing in another Fortune article, titled, “How Theranos Misled Me.”
The government alleged Holmes used media publicity as part of her scheme to defraud investors, patients, and physicians. All totaled, 29 witnesses appeared for the prosecution, the WSJ reported.
Former Theranos Chief Operating Officer Ramesh “Sunny” Balwani—Holmes’ one-time boyfriend—faces similar charges of defrauding patients, investors, and physicians. His trial is expected to begin in January 2022.
Clinical laboratory managers and pathologists who have watched the federal court proceedings with keen interest should expect the trial to wrap up at the conclusion of Holmes’ testimony, just in time for the Balwani fraud trial to begin.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
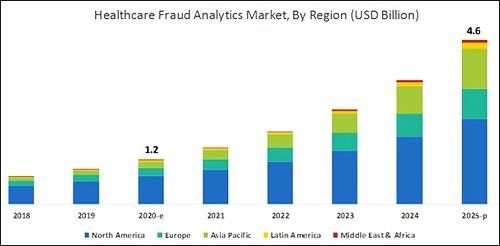
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.