Clinical laboratory managers and pathology practice administrators should consider how these trends may affect their business and patients when planning for the future.
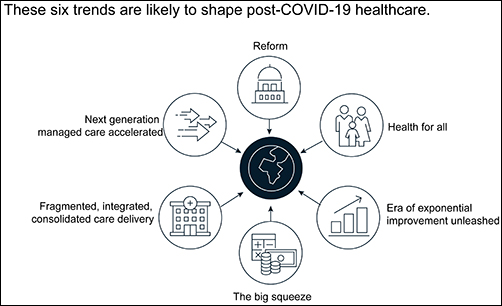
The McKinsey graphic above illustrates the “six trends that are likely to shape post-COVID-19 healthcare.” Clinical laboratories that support health networks struggling with any of these challenges should take steps to prepare for anticipated changes to healthcare delivery. (Graphic copyright: McKinsey and Company.)
1: Healthcare Reform
McKinsey identified three areas where the coronavirus pandemic may impact healthcare reform:
“COVID-19-era waivers that could become permanent.
“Actions that may be taken to strengthen the healthcare system to deal with pandemics.
“Reforms to address the COVID-19-induced crisis.”
McKinsey reports that “the Centers for Medicare and Medicaid Services has introduced more than 190 waivers since the beginning of March 2020.” These waivers can affect all aspects of healthcare, from clinical practice to reimbursement. Some of them, according to McKinsey, are “only relevant during the crisis (for example, the waiver of intensive care unit death reporting). A retrospective assessment of others (for example, expansion of telehealth access) could reveal beneficial innovation worth preserving.”
Several areas that McKinsey says are clearly ripe for reform include improving the resiliency of the healthcare system and the way the system is funded.
Public sector budgets are generally kept strictly separate, each with its own rules and policies that dictate operations. But in his article, “After COVID-19—Thinking Differently About Running the Health Care System,” published in JAMA Health Network, Stuart M. Butler, PhD, Senior Fellow in Economic Studies at the Brookings Institution, wrote, “The intensity of the COVID-19 pandemic … is forcing jurisdictions all across the country to find ways to be nimble so that multiple agencies can work together.”
Thus, McKinsey recommends, “Given the substantial shifts in relative market positioning among industry players that prior reforms have created, leaders would do well to plan ahead now.”
2: Better Access to Healthcare Services
Some people who develop COVID-19 are at far greater risk of hospitalization and death than others, including those who have:
Chronic health conditions, including obesity.
Mental and behavioral health challenges, such as substance abuse.
Unmet social needs, such as food or housing insecurity.
Poor access to healthcare.
McKinsey wrote that these “intersecting health and social conditions,” combined with certain races that have higher risk for severe complications, including Black, Indian, and Hispanic/Latino Americans, “correlated with poorer health outcomes.”
Value-based healthcare, telehealth, and greater attention to the social determinants of health may help address some of these issues, McKinsey notes, but the pandemic has shined a spotlight on how lack of care increases risk for certain populations during a public health crisis.
3: Era of Exponential Improvement Unleashed
Some of the trends that appear to be accelerating as a result of the pandemic are good news. McKinsey cites several benefits, including:
Improved understanding of patients.
Delivery of more convenient and individualized care.
$350-$410 billion in annual revenue by 2025.
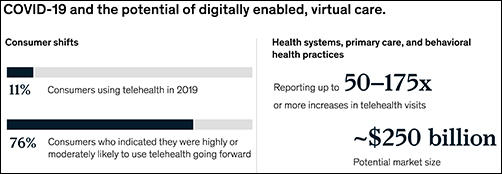
Through telehealth and other types of virtual care enabled by digital technology, “intuitive healthcare ecosystems” may arise and offer a more integrated experience for patients and their caregivers, McKinsey notes.
“While the pace of change in healthcare has lagged other industries in the past, potential for rapid improvement may accelerate due to COVID-19. An example is the exponential uptake of digitally enabled, virtual care,” McKinsey wrote. “Our analysis … showed that health systems, primary care, and behavioral health practices are reporting increases of more than 50–175 times in telehealth visits, and the potential market size for virtual care could reach around $250 billion.”
The graphic above is taken from the McKinsey and Co. report, which noted, “Proliferation of digitally enabled, virtual care could further contribute to the rise of personalized and intuitive healthcare ecosystems [that] have the potential to deliver an integrated experience to consumers, enhance productivity of providers, engage both formal and informal caregivers, and improve outcomes while lowering cost.” (Graphic copyright: McKinsey and Company.)
4: The Big Squeeze
The pandemic has caused an enormous outflow of cash from the healthcare system, and some experts don’t expect an injection of funding until 2022. “This outflow is expected to be primarily driven by coverage shifts out of employer-sponsored insurance and possible coverage reductions by employers as well as Medicaid rate pressures from states,” McKinsey states.
“We estimate that COVID-19 could depress healthcare industry earnings by between $35 billion and $75 billion compared with baseline expectations,” McKinsey predicted, adding, “Select high-growth segments will remain attractive (for example, virtual care, home health, software and platforms, specialty pharmacy) and will disproportionally drive growth. These high-growth areas are expected to increase more than 10% over the next five years, while other segments may stagnate or decline altogether.”
5: Fragmented, Integrated, Consolidated Care Delivery
McKinsey says, “The shift of care out of hospitals is not new but has been accelerated by COVID-19.” Rather than the hospital being the center of care delivery, patients are increasingly choosing to receive care at a range of sites across many healthcare ecosystems that are connected digitally and through analytics.
Early in the course of the pandemic, visits to ambulatory care facilities dropped nearly 60% by early April. But by mid-May, those visits were beginning to rebound.
In, “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges,” the Commonwealth Fund reported that “the relative decline in visits remains largest among surgical and procedural specialties and pediatrics” but is “smaller in other specialties, such as adult primary care and behavioral health.”
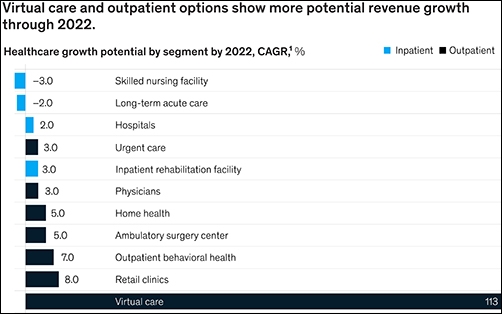
The McKinsey graphic above shows how “virtual care and outpatient options show more potential revenue growth through 2022.” Clinical laboratories that support those healthcare settings, especially ambulatory surgery, behavioral health, and retail clinics, should experience similar growth. (Graphic copyright: McKinsey and Company.)
6: Adoption of Next-Generation Managed Care Is Accelerating
How will COVID-19 affect the managed care industry? McKinsey says the “next generation” of managed care might use Medicare Advantage as a model.
“Payers pursuing the next generation of managed care model (through deep integration with care delivery) demonstrate better financial performance, capturing an additional 50 basis points of earnings before interest, taxes, depreciation, and amortization above expectation,” McKinsey noted, adding, “Employers and payers could consider fundamentally rethinking how employer-sponsored health coverage is structured. Learning from Medicare Advantage could provide inspiration for such a reimagination.”
What Should Clinical Laboratory Managers Do?
The McKinsey article concludes by stating, “While the challenges are numerous, leaders who seize the mindset that “disruptive change provides an opportunity to separate yourself from the pack” will build organizations meaningfully stronger than the ones they ran going into the crisis.”
The McKinsey article authors recommend that healthcare organizations take several proactive steps, including:
Launch a plan-ahead team.
Question your role and your future business model.
Prepare to transform your business.
Reimagine your organization to make faster decisions.
Take action to drive health equity.
Though the McKinsey and Company article covered healthcare in general, many of the authors’ observations and recommendations can apply to clinical laboratories and pathology groups as well and may be valuable in future planning.
Working from tissue slides similar to those used by surgical pathologists, the algorithm accurately detects prostate cancer with an impressive 98% sensitivity
It could be that a new milestone has been reached on the road to using artificial intelligence (AI) to help anatomic pathologists diagnose cancer and other diseases. A research collaboration between a major American university and an Israeli company recently published a study about the ability of an AI algorithm to correctly diagnose prostate cancer.
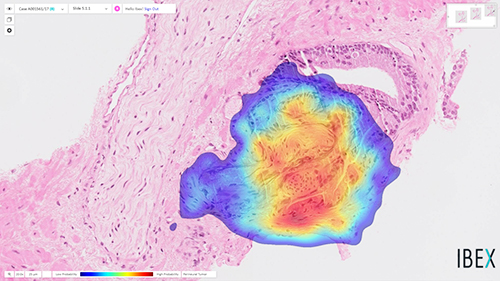
The scientists trained the Galen Prostate AI to recognize prostate cancer by having it examine images from over a million parts of stained tissue slides taken from patient biopsies. Expert pathologists labeled each image to teach the algorithm how to distinguish between healthy and abnormal tissue. The AI was then tested on 1,600 different tissue slide images that had been collected from 100 patients seen at UPMC who were suspected of having prostate cancer.
“Humans are good at recognizing anomalies, but they have their own biases or past experience,” said Rajiv Dhir, MD, Chief Pathologist and Vice Chair of Pathology at UPMC Shadyside Hospital, Professor of Biomedical Informatics at University of Pittsburgh, and senior author of the study, in a UPMC news release. “Machines are detached from the whole story. There’s definitely an element of standardizing care.”
The image above is “of prostate cancer (represented by the heatmap) detected by the Ibex Galen Prostate [AI] solution on a biopsy that was previously diagnosed as benign by the pathologist,” stated an Ibex news release announcing the UPMC study. (Photo copyright: Ibex.)
UPMC Algorithm Goes Beyond Cancer Detection, Exceeds Human Pathologists
The researchers also noted that this is the first algorithm to extend beyond cancer detection. It reported high performance for tumor grading, sizing, and invasion of surrounding nerves—clinically important features of pathology reports.
“Algorithms like this are especially useful in lesions that are atypical,” Dhir said. “A nonspecialized person may not be able to make the correct assessment. That’s a major advantage of this kind of system.”
The algorithm also flagged six slides as potentially containing abnormal tissue that were not flagged by human pathologists. However, the researchers pointed out that this difference does not mean the AI is better than humans at detecting prostate cancer. It is probable, for example, that the pathologists simply saw enough evidence of malignancy elsewhere in the patients’ samples to recommend treatment.
Other Studies Where AI Detected Prostate Cancer
The UPMC researchers are not the first to use AI to detect prostate cancer. In February, The Lancet Oncology published a study from researchers at Radboud University Medical Center (RUMC) in the Netherlands who developed a deep learning AI system that could determine the aggressiveness of prostate cancer in certain patients.
For that research, the RUMC scientists collected 6,000 biopsies from more than 1,200 men. They then showed the biopsy images along with the original pathology reports to their AI system. Using deep learning, the AI was able to detect and grade prostate cancer according to the Gleason Grading System (aka, Gleason Score), which is used to rate prostate cancer and choose appropriate treatment options. The Gleason Score ranges from one to five and most cancers obtain a score of three or higher.
“Systems such as ours can be used in different ways. First, it can be used to screen biopsies and to filter out the easy (benign) cases. This could reduce the workload for pathologists,” said Wouter Bulten, a PhD candidate at Radboud who worked on the study, in an interview with HemOnc Today. “Second, the system can be used as a second opinion after the pathologist’s initial read. The system can flag a case if its opinion differs from that of the pathologist. It also can give feedback during the first read, showing the pathologist where to look. In this case, the pathologist needs only to confirm the opinion of the AI system.”
Can Today’s AI Outperform Human Pathologists?
In their research, the Radboud team discovered that their AI system was able to achieve pathologist-level performance and, in some cases, even performed better than human pathologists. However, they do not foresee AI replacing the need for pathologists, but rather emerging as another method to use in cancer detection and treatment.
“We see our system as an additional tool that the pathologist can use. Although our system performs very well, it still makes mistakes,” stated Bulten. “These mistakes are often different from those a human would make. We believe that when you merge the expertise of the pathologist with the second opinion of an AI system, you get the best of both worlds.”
According to the American Cancer Society, prostate cancer is the second most common cancer among men in the US, after skin cancer. The organization estimates there will be approximately 191,930 new cases of prostate cancer diagnosed and about 33,330 deaths from the disease in the US in 2020.
Though the UPMC study focused only on prostate cancer, the scientists believe their algorithm can be trained to detect other types of cancer as well. AI in clinical diagnostics is clearly progressing, however more studies will be required. Nevertheless, if AI can truly become a useful tool for anatomic pathologists to detect cancer earlier, we may see a welcomed reduction in cancer deaths.
Two national studies find pathologists bill out-of-network more frequently than other hospital-based specialties, and one study links that behavior to insurer reimbursement rates
Surprise bills for out-of-network services continue to be an important issue for healthcare consumers. Now comes a recently-released report from the Health Care Cost Institute (HCCI) claiming that pathologists are the specialists that most often bill for out-of-network hospital charges.
The HCCI study examined the prevalence and frequency of out-of-network billing among six specialties. The sample used for the report included 13.8 million healthcare visits to over 35 thousand hospital-based healthcare providers that occurred in 2017. The types of visits examined for the report were:
emergency medicine,
pathology,
radiology,
anesthesiology,
behavioral health, and
cardiovascular services.
The researchers calculated the percentage of out-of-network claims for both inpatient and outpatient visits to each type of the six specialties.
The study found that, overall, less than half of the specialties billed out-of-network for services obtained at in-network facilities. Providers with at least one out-of-network claim associated with an in-network outpatient visit ranged from 15% for behavioral health to 49% for emergency medicine.
Pathologists’ Out-of-Network Billing
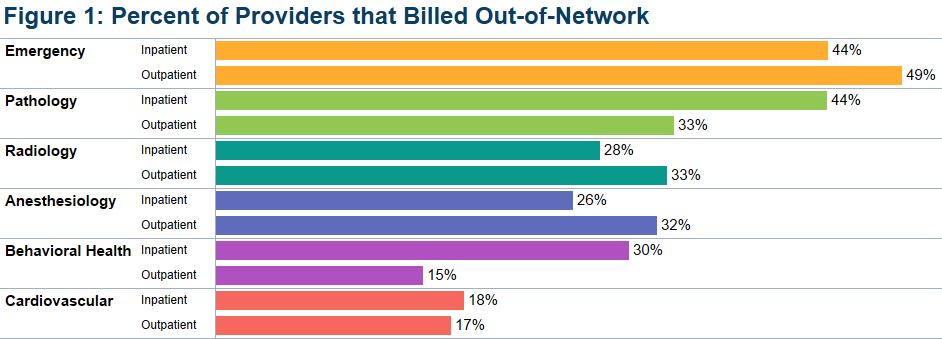
Among the pathologists surveyed, HCCI found 33% had at least one out-of-network claim for an in-network outpatient visit. Providers with at least one out-of-network claim associated with an in-network inpatient visit ranged from 18% for cardiovascular services to 44% for both emergency and pathology services.
HCCI researchers also examined how often individual providers in the six specialties billed out-of-network at least one time and found that the majority billed out of network less than 10% of the time. However, this varied among the specialties with 36% of pathologists who billed out-of-network for inpatient visits, and 20% of pathologists who billed out-of-network for outpatient visits, did so more than 90% of the time.
The graphic above, taken from the latest HCCI report, shows “the share of providers who billed out-of-network at least once for inpatient and outpatient visits” and illustrates the percentage of out-of-network billings by pathologists compared to other hospital-based healthcare specialties. (Graphic copyright: Health Care Cost Institute.)
Pathologists Top List of Out-of-Network Specialists in Previous HCCI report
Last November, HCCI released a similar report that examined the commonality of out-of-network billing for the same six specialties plus surgical services that took place in 2017. Based on their collected data, they also estimated the amount of surprise bills that patients could expect to receive for those services.
That report found that nationally:
16.5% of visits with emergency room services had an out-of-network claim from an emergency medicine specialist.
12.9% of visits with lab/pathology services had an out-of-network claim from a pathologist.
8.3% of visits with anesthesiology services had an out-of-network claim from an anesthesiologist.
6.7% of visits with behavioral health services had an out-of-network claim from a behavioral health provider.
4.2% of visits with radiology services had an out-of-network claim from a radiologist.
2.1% of visits with surgical services had an out-of-network claim from a surgeon.
2.0% of visits with cardiovascular services had an out-of-network claim from a cardiovascular specialist.
Surgical Services the Most Expensive Out-of-Network Bill
This study also found broad variation in charges between types of services and healthcare settings. The researchers determined that the potential surprise bills for surgical visits due to out-of-network claims were of the greatest magnitude. HCCI estimated that the average potential surprise bill associated with an inpatient surgery was $22,248, while the potential surprise bill associated with an outpatient surgery was $8,493.
Out-of-Network Surprise Billing Varies Widely Depending on Location
The data was further broken down by state. For pathology services, the percentage of visits with out-of-network services in 2017 ranged from 0.3% in Minnesota to 75.3% in Kansas. HCCI researchers estimated the potential surprise bill for out-of-network pathology claims for inpatient services ranged from $14 in Louisiana to $167 in Delaware. The estimated surprise bill for out-of-network outpatient pathology services ranged from $23 in Louisiana to $218 in Wyoming.
Pathologists Also Top Out-of-Network Biller in Yale University Study
A Yale University study into surprise billing released in December and published in the journal Health Affairs found similar results, Modern Healthcare reported. This study examined surprise out-of-network bills incurred by patients who sought care at in-network hospitals for four types of specialists that are not chosen by patients:
pathologists,
anesthesiologists,
radiologists, and
assistant surgeons.
Zack Cooper, PhD (above), is an associate professor of public health at the Yale School of Public Health and one of the study’s authors. He noted in Yale News, “When physicians whom patients do not choose and cannot avoid bill out of network, it exposes people to unexpected and expensive medical bills and undercuts the functioning of US healthcare markets,” adding, “Moreover, the ability to bill out of network allows specialists to negotiate inflated in-network rates, which are passed on to consumers in the form of higher insurance premiums.” (Photo copyright: Yale School of Public Health.)
For the Yale study, the researchers examined employer-sponsored insurance claims from a major commercial insurer for healthcare visits that occurred at in-network hospitals in 2015. They found that 12.3% of cases involving a pathologist were billed out-of-network, which was the highest percentage of the four specialties analyzed. By contrast, 11.8% of anesthesiologists, 11.3% of assistant surgeons, and 5.6% of radiologists billed out-of-network for their services.
The Yale study also found that “the ability of these four specialties to send patients out-of-network bills allowed them to negotiate high in-network payments from insurers, which leads to higher insurance premiums for individuals.”
The Yale study researchers determined that were these specialists unable to bill out-of-network, the particular healthcare plan would save 3.4% of their expenditures or about $40 billion per year, Modern Healthcare reported.
Surprise bills for out-of-network services burden both patients and providers. Insurers want beneficiaries to have access to hospitals and services, but providers in many specialties do not want to contract with those insurers due to low reimbursements.
This disconnect results in providers staying out-of-network and patients receiving surprise bills for out-of-network services even though the hospital was in-network. And pathologists are at the top of the list.
Anatomic pathologists across the country will want to track how government and private payers respond to these findings by amending coverage and reimbursement guidelines in ways that may be unfavorable to the pathology profession.
Centers for Medicare and Medicaid Innovation is considering adding clinical laboratory services to bundled payments in its proposed Oncology Care First model
CMMI, an organization within the Centers for Medicare and Medicaid Services (CMS), is charged with developing and testing new healthcare delivery and payment models as alternatives to the traditional fee-for-service (FFS) model. On November 1, 2019, CMMI released an informal Request for Information (RFI) seeking comments for the proposed Oncology Care First (OCF) model, which would be the successor to the Oncology Care Model (OCM) launched in 2016.
“The inefficiency and variation in oncology care in the
United States is well documented, with avoidable hospitalizations and emergency
department visits occurring frequently, high service utilization at the end of
life, and use of high-cost drugs and biologicals when lower-cost, clinically
equivalent options exist,” the CMMI RFI states.
With the proposed new model, “the Innovation Center aims to build on the lessons learned to date in OCM and incorporate feedback from stakeholders,” the RFI notes.
How the Oncology Care First Model Works
The OCF program, which is voluntary, will be open to
physician groups and hospital outpatient departments. CMMI anticipates that
testing of the model will run from January 2021 through December 2025.
It will offer two payment mechanisms for providers that
choose to participate:
A Monthly Population Payment (MPP) would apply
to a provider’s Medicare beneficiaries with “cancer or a cancer-related
diagnosis,” the RFI states. It would cover Evaluation and Management (EM)
services as well as drug administration services and a set of “Enhanced
Services,” including 24/7 access to medical records.
Of particular interest to medical laboratories, the RFI also
states that “we are considering the inclusion of additional services in the monthly
population payment, such as imaging or medical laboratory services, and seek
feedback on adding these or other services.”
In addition, providers could receive a
Performance-Based Payment (PBP) if they reduce expenditures for patients
receiving chemotherapy below a “target amount” determined by past Medicare
payments. If providers don’t meet the threshold, they could be required to
repay CMS.
Practices that wish to participate in the OCF model must go through an application process. It is also open to participation by private payers. CMS reports that 175 practices and 10 payers are currently participating in the 2016 Oncology Care Model (OCM).
“We want better quality care for patients,” explained Lara Strawbridge, MPH (above), Director of the CMMI Division of Ambulatory Payment Models, during a US Department of Health and Human Services public listening session on Nov. 8. “We hope that at the same time, costs are maintained or reduced.” The new OCF payment model will feature a Monthly Population Payment mechanism that could include reimbursements for medical laboratory services, which has some medical laboratory organizations concerned. (Photo copyright: Center for Medicare and Medicaid Innovation.)
Medical Lab Leaders Concerned about the CMMI OCF Model
One group raising concerns about the inclusion of medical laboratory service reimbursements in the Monthly Population Payment scheme is the Personalized Medicine Coalition. “Laboratory services are crucial to the diagnosis and management of many cancers and are an essential component of personalized medicine,” wrote Cynthia A. Bens, the organization’s senior VP for public policy, in an open letter to CMMI Acting Director Amy Bassano. “We are concerned that adding laboratory service fees to the MPP may cause providers to view them as expenses that are part of the total cost of delivering care, rather than an integral part of the solution to attain high-value care,” Bens wrote.
She advised CMMI to “seek further input from the laboratory
and provider communities on how best to contain costs within the OCF model,
while ensuring the proper deployment of diagnostics and other laboratory
services.”
Members of the coalition include biopharma companies, diagnostic companies, patient advocacy groups, and clinical laboratory testing services. Lab testing heavyweights Quest Diagnostics (NYSE:DGX) and Laboratory Corporation of America (NYSE:LH) are both members.
CMS ‘Doubles Down’ on OCM
The proposal received criticism from other quarters as well. “While private- and public-sector payers would be well served to adopt and support a VBP [value-based payment] program for cancer care, we need to better understand some of the shortcomings of the original OCM design and adopt lessons learned from other successful VBP models to ensure uptake by providers and ultimately better oncology care for patients,” wrote members of the Oncology Care Model Work Group in a Health Affairs blog post. They added that with the new model, “CMS seems to double down on the same design as the OCM.”
Separately, CMMI has proposed a controversial Radiation
Oncology (RO) alternative payment model (APM) that would be mandatory for
practices in randomly-selected metro areas. The agency estimates that it would
apply to approximately 40% of the radiotherapy practices in the US.
These recent actions should serve to remind pathologists and
clinical laboratories that CMS continues to move away from fee-for-service and
toward value-based care payment models, and that it is critical to plan for
changing reimbursement strategies.
Pathologists can be paid for their role in identifying and recruiting patients for basket studies and reporting results of medical laboratory tests
Anatomic
pathologists who biopsy, report, and diagnosis cancer will benefit from a
better understanding of basket
studies and their application in developing cancer treatment therapies. Such
studies can lead to more documentation of the effectiveness of various therapies
for cancers with specific gene
signatures.
The US
National Library of Clinical Medicine defines basket studies as “a new sort
of clinical studies to identify patients with the same kind of mutations and
treat them with the same drug, irrespective of their specific cancer type. In
basket studies, depending on the mutation types, patients are classified into ‘baskets.’
Targeted therapies that block that mutation are then identified and assigned to
baskets where patients are treated accordingly.”
“Historically, cancer clinical trials have been centered on the treatment of cancer based on the anatomic location in the body, like breast cancer or brain cancer or lung cancer. A basket study is a novel trial design that includes patients with a certain molecular aberration regardless of location or tissue of origin of cancer in the body. The genomic revolution in oncology has fueled these studies,” Vivek Subbiah, MD, Associate Professor and Medical Director, Clinical Center for Targeted Therapy ( Phase 1 trials program), at the University of Texas MD Anderson Cancer Center in Houston, told Cancer Therapy Advisor. (Photo copyright: MD Anderson Cancer Center.)
Basket Studies Get Results
During a basket study, researchers may find that a drug’s
effectiveness at targeting “a genetic mutation at one site can also treat the
same genetic mutation in cancer in another area of the body,” noted Pharmacy
Times, which also pointed out basket studies are often starting points for
larger oncology trials about drugs.
For example, it was a basket study which found that vemurafenib (marketed as
Zelboraf), intended for treatment of V600E, a mutation of the BRAF gene, may also treat Erdheim-Chester
disease (a rare blood disorder) in patients who have the BRAF V600 gene
mutation, Pharmacy Times reported.
Additionally, the US Food and Drug Administration’s approval
of the cancer drug Vitrakvi (larotrectinib), an oral TRK
inhibitor, marked the first treatment to receive a “tumor-agnostic
indication at time of initial FDA approval,” a Bayer
news release stated. The drug’s efficacy, Pharmacy Times noted, was
found in a “pivotal” basket study.
Basket Studies, a Master Protocol Trial Design
The basket study technique is an example of a master protocol trial design. The FDA defines a master protocol as “a protocol designed with multiple substudies, which may have different objectives and involves coordinated efforts to evaluate one or more investigational drugs in one or more disease subtypes within the overall trial structure. A master protocol may be used to conduct the trial(s) for exploratory purposes or to support a marketing application and can be structured to evaluate, in parallel, different drugs compared to their respective controls or to a single common control.”
Other master protocols include umbrella studies and platform
studies, according to Cancer Therapy Advisor, which noted that each
master protocol trial design has its own unique objectives:
Umbrella studies look at the effectiveness of
multiple drugs on one type of cancer;
Platform trials investigate the effectiveness of
multiple therapies on one disease on an ongoing basis; and
Basket studies focus on the effectiveness of one
therapy on patients with different cancers based on a biomarker.
“In contrast to traditional trials designs, where a single
drug is tested in a single disease population in one clinical trial, master
protocols use a single infrastructure, trial design, and protocol to
simultaneously evaluate multiple drugs and or disease populations in multiple
substudies, allowing for efficient and accelerated drug development,” states
the FDA draft guidance, “Master
Protocols: Efficient Clinical Trial Design Strategies to Expedite Development
of Oncology Drugs and Biologics.”
Final FDA guidance on master protocols design is expected early in 2020, an FDA spokesperson told Cancer Therapy Advisor.
While master protocol studies show promise, they generally
have small sample sizes, noted researchers of a study published in the journal Trials.
And some researchers have ethical concerns about basket studies.
Nevertheless, basket studies appear to hold promise for precision medicine.
Anatomic pathologists may want to follow some of them or find a way to get
involved through identifying clinical laboratory tests and reporting the results.