Japanese scientists who developed the detection method hope to use it to create ‘easy testing kits that anyone can use’
What do ostriches and humans have in common during the current COVID-19 pandemic? The unexpected answer is that ostrich antibodies can be used to identify humans infected with COVID-19. If proven viable in healthcare settings, the possibility exists that new clinical laboratory tests could be developed based on wearable diagnostics technologies that pathologists would interpret for doctors and patients.
According to Study Finds, scientists at Kyoto Prefectural University in Japan have created a removable mask filter that, when sprayed with a fluorescent dye coated with antibodies extracted from ostrich eggs, will glow under UV light when COVID-19 is detected. The discovery by Yasuhiro Tsukamoto, PhD (above), President of Kyoto Prefectural University, and his researchers could lead to development of low-cost at home COVID-19 testing kits using the same ostrich-antibody-based technique. (Photo copyright: Kyoto Prefectural University/Reuters.)
The KPU scientists conducted a small study with 32 COVID-19 patients over a 10-day span. The surgical-style masks they wore later glowed around the nose and mouth areas but became dimmer over time as their viral load decreased.
“The ostrich antibody for corona placed on the mouth filter of the mask captures the coronavirus in coughing, sneezing, and water,” the researchers explained in Study Finds.
Tsukamoto himself learned he had contracted COVID-19 after wearing a prototype mask and noticing it glowed under UV light. A PCR test later confirmed his diagnosis, Kyodo News reported.
The KPU team “hopes to further develop the masks so they will glow automatically, without special lighting, if the [COVID-19] virus is detected.” Reuters noted in its coverage of the ostrich-antibody masks.
Making Medicine from Ostrich Antibodies
A profile in Audubon noted that Tsukamoto, who also serves as a veterinary medicine professor at Kyoto Prefectural University, made ostriches the focus of his research since the 1990s as he looked for ways to harness the dinosaur-like bird’s properties to fight human infections. He maintains a flock of 500 captive ostriches. Each female ostrich can produce 50 to 100 eggs/year over a 50-year life span.
Tsukamoto’s research focuses on customizing the antibodies in ostrich eggs by injecting females with inactive viruses, allergens, and bacteria, and then extracting the antibodies to develop medicines for humans. Antibodies form in the egg yolks in about six weeks and can be collected without harming the parent or young.
“The idea of using ostrich antibodies for therapeutics in general is a very interesting concept, particularly because of the advantages of producing the antibodies from eggs,” Ashley St. John, PhD, an Associate Professor in Immunology, at Duke-NUS Medical School in Singapore, told Audubon.
While more clinical studies will be needed before ostrich-antibody masks reach the commercial marketplace, Tsukamoto’s team is planning to expand their experiment to 150 participants with a goal of receiving Japanese government approval to begin selling the glowing COVID-detection masks as early as 2022. But they believe the ostrich-antibody technique ultimately may lead to development of an inexpensive COVID-19 testing kit.
“We can mass-produce antibodies from ostriches at a low cost. In the future, I want to make this into an easy testing kit that anyone can use,” Tsukamoto told Kyodo News.
Harvard, MIT Also Working on COVID-19 Detecting Facemask
According to Fast Company, the MIT/Harvard COVID-19-detecting masks use the same core technology as previous paper tests for Ebola and Zika that utilize proteins and nucleic acids embedded in paper that react to target molecules.
Fast Company explained that the mask wearer launches a test by pushing a button to release a small water reservoir embedded in the mask (above). Droplets from their breath are than analyzed by the sensors in the masks, which could be adapted to test for new COVID variants or other respiratory pathogens. In addition to eliminating the use of a nasal swab, the mask-based testing system may compete with clinical laboratory-based results. (Photo copyright: Felice Frankel/MIT.)
“They would especially be useful in situations where local variant outbreaks are occurring, allowing people to conveniently test themselves at home multiple times a day,” he told Fast Company.
“It’s on par specificity and sensitivity that you will get in a state-of-the-art [medical] laboratory, but with no one there,” Luis Ruben Soenksen, PhD, Venture Builder in Artificial Intelligence and Healthcare at MIT and one of the co-authors of the Nature Biotechnology study, told Fast Company.
As the definition of “wearable diagnostic technology” broadens, pathologists and clinical laboratory scientists may see their roles expand to include helping consumers interpret data collected by point-of-care testing technology as well as performing, evaluating, and interpreting laboratory test results that come from non-traditional sources.
Former CEO also testified that she believed company’s proprietary blood-testing technology could perform ‘any’ clinical laboratory blood test
One relevant question in the federal fraud trial of ex-Theranos CEO Elizabeth Holmes was whether she would testify on her own behalf. That question was answered shortly after the government rested its criminal fraud case against the former Silicon Valley clinical laboratory testing company founder. Holmes took the stand in her own defense, a risk her defense team hopes will pay off in her favor.
During her first three days of testimony leading up to the Thanksgiving holiday break, Holmes—who faces 11 counts of fraud and conspiracy related to her tenure as founder and CEO of Theranos—made headlines by admitting she did personally put the logos of pharmaceutical giants Pfizer and Schering-Plough on reports she sent to Theranos investors and executives at Walgreens and Safeway. She expressed regret for doing so to the jury, but claimed her intent was not to deceive but to give credit to others.
“This work was done in partnership with these companies, and I was trying to convey that,” she testified, according to a trial coverage from Ars Technica.
When asked if she realized that others would assume the pharmaceutical companies—not Theranos—were the authors of the report, Holmes replied, “I’ve heard that testimony in this case, and I wish I’d done it differently.”
If found guilty, Holmes—who once claimed Theranos’ Edison proprietary blood-testing technology would to be able to complete as many as 200 clinical laboratory tests using a single finger-stick of blood—could face maximum penalties of 20 years in prison, a $2.75 million fine, and possible restitution.
The illustration above depicts ex-Theranos CEO Elizabeth Holmes testifying on her own behalf. Former Santa Clara County prosecutor Steven Clark, JD, told The Mercury News, “(T)he best person to say what Elizabeth Holmes’ intent was is Elizabeth Holmes, and that’s why I think she’s taking the stand. … I think the jury will like her.” That remains to be seen. But there’s no doubt that Clinical Laboratory Directors should take a strong interest in the outcome of this trail. (Graphic copyright: Vicki Behringer/Reuters.)
Holmes Testifies She Believed the Edison Device Could Perform “Any” Blood Test
In its trail coverage, NPR described Holmes’ first three days of testimony “as having involved deflecting responsibility, pointing to the expertise of the Theranos board of directors, lab staff, and other company employees whom Holmes has suggested were close to how [Theranos’] blood analyzers worked.”
According to Reuters, Holmes’ defense team is arguing that Holmes’ always-rosy forecasts about her company’s technology and finances were based on her belief the proprietary Edison device worked as advertised, which, in turn, was based on feedback from pharmaceutical companies, her own employees, and the military.
During her testimony, Holmes compared a traditional blood-testing device to Theranos’ “3.0” device, which she said would reduce the human-error rate that can occur during blood sampling.
“If we had the ability to automate much of that process, we could reduce the error associated with traditional lab testing,” she told the court.
Reuters reported that Holmes told jurors her confidence in the Theranos device was in part due to how well the unit had performed in studies completed in 2008 and 2009, including those run by drug companies such as Novartis.
The Mercury News described Holmes as speaking with “confidence—and frequently a small smile”—during her opening day of testimony.
Asked by one of her lawyers, “Did you believe that Theranos had developed technology that was capable of performing any blood test?” Holmes responded, “I did.”
Holmes Testifies about Military’s Alleged Use of Edison Device
Prosecutors maintain that Holmes knew Theranos’ proprietary blood-testing technology had serious accuracy issues yet lied about its capabilities and use to lure investors. One of those false claims included allegedly stating the US military was using the Edison device on the battlefield. Earlier in the trial, CNBC reported, prosecution witness Brian Grossman, Chief Investment Officer at PFM Health Sciences, which invested $96 million into Theranos, testified he was told in a 2013 meeting with Holmes and Balwani that Theranos technology was being used in medical-evacuation helicopters.
However, on the witness stand, Holmes described Theranos’ projects with the US military as much more limited in scope than the descriptions outlined by investors testifying for the prosecution.
According to The Wall Street Journal (WSJ), Holmes told jurors a 2010 partnership between Theranos and a US Army Institute of Surgical Research doctor in Texas looked into using the Theranos device to measure blood markers to detect kidney performance. A second project involved the military’s Africa Command, which was determining whether the device could withstand high temperatures. Holmes testified the devices used in Africa “held up well,” though some modifications were needed, and some issues were revealed with the touchscreen.
Should Holmes Have Testified on Her Own Behalf?
Trial experts maintain Holmes’ decision to testify in her own defense could backfire.
“It’s always a risk to put your client on because if they make a mistake they can sink the whole case,” former Santa Clara County prosecutor Steven Clark, JD, told The Mercury News. He added, “what’s at issue here is Elizabeth Holmes’ intent. And the best person to say what Elizabeth Holmes’ intent was is Elizabeth Holmes, and that’s why I think she’s taking the stand. She’s very charismatic. She’s really good on her feet. And I think the jury will like her.
“This is the pitch meeting of her life,” Clark added. “She’s going to be explaining herself to 12 people as to what was in her mind.”
Judge Drops One Count Due to Prosecution Error, Government Rests Its Case
Holmes is now charged with nine counts of wire fraud and two counts of conspiracy to commit wire fraud after the government dropped one count of fraud from the indictment. According to WSJ coverage of the trial, US District Judge Edward Davila blocked a patient named in the indictment as “B.B.” from testifying because of a filing error by the prosecution. The judge’s decision resulted in the government dropping one count.
The government rested its case against Holmes on November 19 following testimony from independent journalist Roger Parloff, who wrote a flattering 2014 Fortune magazine story on Holmes. He later redacted his earlier writing in another Fortune article, titled, “How Theranos Misled Me.”
The government alleged Holmes used media publicity as part of her scheme to defraud investors, patients, and physicians. All totaled, 29 witnesses appeared for the prosecution, the WSJ reported.
Former Theranos Chief Operating Officer Ramesh “Sunny” Balwani—Holmes’ one-time boyfriend—faces similar charges of defrauding patients, investors, and physicians. His trial is expected to begin in January 2022.
Clinical laboratory managers and pathologists who have watched the federal court proceedings with keen interest should expect the trial to wrap up at the conclusion of Holmes’ testimony, just in time for the Balwani fraud trial to begin.
Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
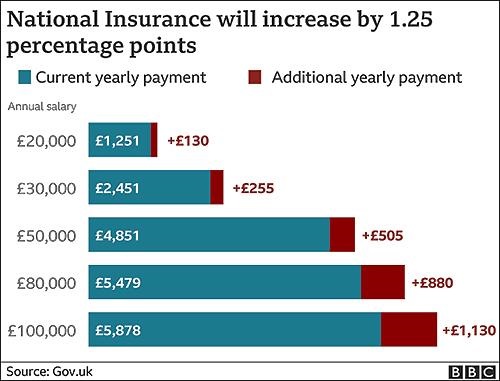
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
Sophisticated cyberattacks have already hit hospitals and healthcare networks in Oregon, California, New York, Vermont, and other states
Attention medical laboratory managers and pathology group administrators: It’s time to ramp up your cyberdefenses. The FBI, the federal Department of Health and Human Services (HHS), and the federal Cybersecurity and Infrastructure Security Agency (CISA) issued a joint advisory (AA20-302A) warning US hospitals, clinical laboratories, and other healthcare providers to prepare for impending ransomware attacks, in which cybercriminals use malware, known as ransomware, to encrypt files on victims’ computers and demand payment to restore access.
The joint advisory, titled, “Ransomware Activity Targeting the Healthcare and Public Health Sector,” states, “CISA, FBI, and HHS have credible information of an increased and imminent cybercrime threat to US hospitals and healthcare providers.” It includes technical details about the threat—which uses a type of ransomware known as Ryuk—and suggests best practices for preventing and handling attacks.
In his KrebsOnSecurity blog post, titled, “FBI, DHS, HHS Warn of Imminent, Credible Ransomware Threat Against U.S. Hospitals,” former Washington Post reporter, Brian Krebs, wrote, “On Monday, Oct. 26, KrebsOnSecurity began following up on a tip from a reliable source that an aggressive Russian cybercriminal gang known for deploying ransomware was preparing to disrupt information technology systems at hundreds of hospitals, clinics, and medical care facilities across the United States. Today, officials from the FBI and the US Department of Homeland Security hastily assembled a conference call with healthcare industry executives warning about an ‘imminent cybercrime threat to US hospitals and healthcare providers.’”
Krebs went on to reported that the threat is linked to a notorious cybercriminal gang known as UNC1878, which planned to launch the attacks against 400 healthcare facilities.
Clinical Labs, Pathology Groups at Risk Because of the Patient Data They Keep
Hackers initially gain access to organizations’ computer systems through phishing campaigns, in which users receive emails “that contain either links to malicious websites that host the malware or attachments with the malware,” the advisory states. Krebs noted that the attacks are “often unique to each victim, including everything from the Microsoft Windows executable files that get dropped on the infected hosts to the so-called ‘command and control’ servers used to transmit data between and among compromised systems.”
Charles Carmakal, SVP and Chief Technology Officer of cybersecurity firm Mandiant told Reuters, “UNC1878 is one of the most brazen, heartless, and disruptive threat actors I’ve observed over my career,” adding, “Multiple hospitals have already been significantly impacted by Ryuk ransomware and their networks have been taken offline.”
John Riggi (above), senior cybersecurity adviser to the American Hospital Association (AHA), told the AP, “We are most concerned with ransomware attacks which have the potential to disrupt patient care operations and risk patient safety. We believe any cyberattack against any hospital or health system is a threat-to-life crime and should be responded to and pursued as such by the government.” Hospital-based medical laboratories and independent clinical laboratories that interface with hospital networks should be assess their vulnerability to cyberattacks and take appropriate steps to protect their patients’ data. (Photo copyright: American Hospital Association.)
Multiple Healthcare Provider Networks Under Attack
Hospitals in Oregon, California, and New York have already been hit by the attacks, Reuters reported. “We can still watch vitals and getting imaging done, but all results are being communicated via paper only,” a doctor at one facility told Reuters, which reported that “staff could see historic records but not update those files.”
Some of the hospitals that have reportedly experienced cyberattacks include:
In October, the Associated Press (AP) reported that a recent cyberattack disrupted computer systems at six hospitals in the University of Vermont (UVM) Health Network. The FBI would not comment on whether that attack involved ransomware, however, it forced the UVM Medical Center to shut down its computer system and reschedule elective procedures.
Threat intelligence analyst Allan Liska of US cybersecurity firm Recorded Future told Reuters, “This appears to have been a coordinated attack designed to disrupt hospitals specifically all around the country.”
He added, “While multiple ransomware attacks against healthcare providers each week have been commonplace, this is the first time we have seen six hospitals targeted in the same day by the same ransomware actor.”
An earlier ransomware attack in September targeted 250 healthcare facilities operated by Universal Health Services Inc. (UHS). A clinician at one facility reported “a high-anxiety scramble” where “medical staff could not easily see clinical laboratory results, imaging scans, medication lists, and other critical pieces of information doctors rely on to make decisions,” AP reported.
Outside of the US, a similar ransomware attack in October at a hospital in Düsseldorf, Germany, prompted a homicide investigation by German authorities after the death of a patient being transferred to another facility was linked to the attack, the BBC reported.
CISA, FBI, HHS, Advise Against Paying Ransoms
To deal with the ransomware attacks, CISA, FBI, and HHS advise against paying ransoms. “Payment does not guarantee files will be recovered,” the advisory states. “It may also embolden adversaries to target additional organizations, encourage other criminal actors to engage in the distribution of ransomware, and/or fund illicit activities.” The federal agencies advise organizations to take preventive measures and adopt plans for coping with attacks.
The advisory suggests:
Training programs for employees, including raising awareness about ransomware and phishing scams. Organizations should “ensure that employees know who to contact when they see suspicious activity or when they believe they have been a victim of a cyberattack.”
Regular backups of data and software. These should be “maintained offline or in separated networks as many ransomware variants attempt to find and delete any accessible backups.” Personnel should also test the backups.
Continuity plans in case information systems are not accessible. For example, organizations should maintain “hard copies of digital information that would be required for critical patient healthcare.”
“Without planning, provision, and implementation of continuity principles, organizations may be unable to continue operations,” the advisory states. “Evaluating continuity and capability will help identify continuity gaps. Through identifying and addressing these gaps, organizations can establish a viable continuity program that will help keep them functioning during cyberattacks or other emergencies.”
Dark Daily Publisher and Editor-in-Chief, Robert Michel, suggests that clinical laboratories and anatomic pathology groups should have their cyberdefenses assessed by security experts. “This is particularly true because the technologies and methods used by hackers change rapidly,” he said, “and if their laboratory information systems have not been assessed in the past year, then this proactive assessment could be the best insurance against an expensive ransomware attack a lab can purchase.”
Schwan’s concerns about inaccurate or unreliable COVID-19 serology tests were supported when the FDA issued more restrictive rules for these medical laboratory tests on May 4
During a conference call with investors about the company’s first-quarter results, Schwan said of the recently-launched COVID-19 antibody assays, “These tests are not worth anything, or have very little use,” according to reporting from Reuters and other publications. “Some of these companies, I tell you, this is ethically very questionable to get out with this stuff.”
On May 3, Roche announced that its own Elecsys Anti-SARS-CoV-2 antibody test for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, had obtained an emergency use authorization (EUA) from the federal Food and Drug Administration (FDA). In its news release, Roche stated that “the serology test has a specificity greater than 99.8% and sensitivity of 100% (14 days post-PCR confirmation).”
In a separate interview with Bloomberg, Schwan said about antibody testing, “It is very important to pick the right test and then to validate those tests with enough patients.” He then returned to the issue of poor quality in some antibody tests for the SARS-CoV-2 virus, saying, “Unfortunately, there are a number of tests already out there in the market which are not reliable simply because they haven’t been tested sufficiently.”
In reference to the initial release of serological COVID-19 antibody tests, CEO Severin Schwan (above) said during Roche Holding’s first quarter earnings call that, “It’s a disaster. These tests are not worth anything, or have very little use,” reported CNBC. He added, “This is really what matters. Every kind of amateur could produce an antibody test. The two of us could do it overnight in the garage. That’s not the problem. The question is, does it really work? And for that, you have to do testing and validation.” (Photo copyright: Reuters/Arnd Wiegmann.)
A ‘Wild West’ of Unregulated Assays
Prior to issuing tougher rules for how a manufacturer can market a COVID-19 serological test, the FDA had listed about 200 serological tests designed to identify antibodies produced by the human immune system in response to a SARS-CoV-2 infection. This is the process of seroconversion, which is the development of detectable antibodies in a patient’s blood against a pathogen. Detection of IgG antibodies indicates exposure to SARS-CoV-2, according to ARUP Laboratories.
Public health experts have raised questions about the proliferation of such tests for the new coronavirus. Under the FDA’s previous March 16 rules—which were more relaxed than those FDA applied when granting EUAs—the agency was swamped with requests to review more than 200 COVID-19 antibody tests. The looser regulations resulted in nearly no oversight of those tests, reported the Associated Press (AP).
In comments to the AP, Eric Blank, DrPH, Senior Director of Public Health Systems and Programs for the Association for Public Health Laboratories (APHL), said, “Right now it’s a wild west show out there. It really has created a mess that’s going to take a while to clean up.”
“In the meantime,” Blank added, “you’ve got a lot of companies marketing a lot of stuff and nobody has any idea of how good it is.” Blank confirmed to Dark Daily that he made these comments and stands by them.
Calls for Closer Scrutiny of Serological Antibody Tests
In response to the FDA’s March 16 rules for COVID-19 serology tests, APHL requested the federal agency to review its looser approach to reviewing these tests. The impact of the FDA’s much tougher COVID-19 serological testing rules released on May 4 was immediate.
In a press release issued on May 2, the FDA said, “to date, the FDA has authorized 105 tests under EUAs, which include 92 molecular tests, 12 antibody tests, and one antigen test.”
Clinical laboratories in the United States still face difficult challenges if they plan to launch their own COVID-19 serology testing programs. They must select one or more tests from among the antibody and antigen tests that have an FDA EUA. However, data for each of these tests is not as comprehensive as is the data for diagnostic test kits reviewed by the FDA and cleared for market under the pre-market approval process.
This webinar was conducted by James O. Westgard, PhD, and Sten Westgard of Westgard QC, Inc., and the full program is available for free download by clicking here, or by placing this URL in your web browser: https://www.darkdaily.com/webinar/quality-issues-your-clinical-laboratory-should-know-before-you-buy-or-select-covid-19-serology-tests/.
In the webinar recording, the Westgards provide a detailed overview of what elements are required for a clinical lab to have confidence that its COVID-19 serology testing program is producing accurate, reliable results. They explain that labs must understand the unique aspects of the populations they are testing in their communities. All of these factors can then be used by labs to evaluate the different COVID-19 serology tests available for them to purchase, and to select the test that best fits their lab’s capabilities and the characteristics of the patient population that will be tested.
Another important requirement for clinical laboratories to understand is the list of steps necessary to bring up a COVID-19 serological testing program. That starts with validating the test, then bringing it into daily production. As that happens, issues associated with quality control (QC), proficiency testing (PT), and regulatory compliance take center stage, so that the clinical lab has high confidence in the accuracy and reproducibility of the COVID-19 serology test results they are using in patient care or in support of employers who are screening employees for COVID-19.
To register for the June 11 webinar, click here, or place this URL in your web browser: https://www.darkdaily.com/webinar/achieving-high-confidence-levels-in-the-quality-and-accuracy-of-your-clinical-labs-chosen-covid-19-serology-tests/.
New COVID-19 Intelligence from Dark Daily
Announcing Dark Daily’s new COVID-19 STAT Intelligence Briefings! This free service for clinical laboratories, anatomic pathology groups, and diagnostics companies features:
daily breaking news,
business intelligence, and
innovations that clinical labs are using to respond to the COVID-19 pandemic.
This critical information includes effective ways labs can restore their cash flow to pre-pandemic levels and get test claims paid by government and private payers.
One popular feature is the COVID-19 Live! conference calls that happen every Tuesday and Thursday for 30 minutes at 1 PM, EDT. Visit the COVID-19 STAT Intelligence Briefings website and join us for the live calls.