Should their research result in new ways to identify and diagnose disease, doctors and clinical laboratories would do confirmatory testing and then initiate a precision medicine plan.
Dan Roden, MD, Senior Vice President for Personalized Medicine at VUMC and Senior Author of the Circulation study, said in a VUMC news release that the findings support the growing use of genetic information in clinical care.
“The questions we asked were: How many people who had no previous indication for cardiac genetic testing had pathogenic or likely pathogenic variants, and how many of those people actually had a phenotype in the electronic health records?” he explained.
Arrhythmia More Common than Previously Thought
The VUMC researchers drew data for their reports from the eMERGE Phase III study, which investigated the feasibility of population genomic screening by sequencing 109 genes across the spectrum of Mendelian diseases—genetic diseases that are caused by a mutation in a single gene—in more than 20,000 individuals. The scientists returned variant results to the participants and used EHR and follow-up clinical data to ascertain patient phenotypes, according to a Northwestern University Feinberg School of Medicine news release.
The research team looked specifically at the 120 consortium participants that had disease-associated pathogenic or likely pathogenic (P/LP) variants in the arrhythmia-associated genes. An analysis of the EHR data showed that 0.6% of the studied population had a variant that increases risk for potentially life-threatening arrhythmia, and that there was overrepresentation of arrhythmia phenotypes among patients, the VUMC news release noted.
The research team returned results to 54 participants and, with clinical follow-up, made 19 diagnoses (primarily long-QT syndrome) of inherited arrhythmia syndromes. Twelve of those 19 diagnoses were made only after variant results were returned, the study’s authors wrote.
Carlos G. Vanoye, PhD, Research Associate Professor of Pharmacology at Northwestern University (NU), said the study suggests arrhythmia genes may be more common than previously thought.
“A person can carry a disease-causing gene variant but exhibit no obvious signs or symptoms of the disease,” he said in the NU news release. “Because the genes we studied are associated with sudden death, which may have no warning signs, discovery of a potentially life-threatening arrhythmia gene variant can prompt additional clinical work-up to determine risks and guide preventive therapies.”
“The take-home message is that 3% of people will carry a pathogenic or likely pathogenic variant in a disease-causing gene and many others will carry variants of uncertain significance,” said Dan Roden, MD (above), Senior Vice President for Personalized Medicine at VUMC and Senior Author of the Circulation study in the VUMC news release. “We can use genetic testing, electronic health record phenotypes, and in vitro technologies to evaluate and find people who have unrecognized genetic disease and save lives by making earlier diagnoses.” Clinical laboratories will play a key role in making those early diagnoses and in managing personalized medical treatment plans. (Photo copyright: Vanderbilt University.)
Variants of Uncertain Significance
According to the NU news release, the scientists determined the functional consequences of the variants of uncertain significance they found and used that data to refine the assessment of pathogenicity. In the end, they reclassified 11 of the variants: three that were likely benign and eight that were likely pathogenic.
In the JAMA Oncology study, the VUMC scientists and other researchers conducted a phenome-wide association study to find EHR phenotypes associated with variants in 23 hereditary cancer genes. According to the VUMC news release, they identified 19 new associations:
The VUMC study findings could improve disease diagnosis and management for cancer patients and help identify high-risk individuals, the researchers noted in their published report.
In an editorial published in Circulation, titled, “First Steps of Population Genomic Medicine in the Arrhythmia World: Pros and Cons,” the professors noted that using genomic information in the case of potentially lethal inherited arrhythmia syndromes could be “lifesaving,” but questioned the benefits of reporting such secondary findings when patients are undergoing genome sequencing for other indications such as cancer.
“The likelihood that these ‘genetic diagnoses’ are translated into clinical diagnoses have not been completely evaluated,” they wrote. “In addition to the challenge of accurately identifying disease-causing genetic variants, defining the penetrance of such variants is critical to this process, i.e., what proportion of individuals in the general population with apparently pathogenic variants will develop the associated phenotype? If penetrance is low for particular gene/phenotype combinations, the costs associated with clinical screening and the psychological effects on individuals informed that they have potentially life-threatening variants may outweigh the benefits of the few new clinical diagnoses.”
These latest studies provide further evidence of the value of big data in healthcare and offer another lesson to clinical laboratories and pathologist about the future role data streaming from clinical laboratories and pathology assays may have in the growth of personalized medicine.
New nanotechnology device is significantly faster than typical rapid detection clinical laboratory tests and can be manufactured to identify not just COVID-19 at point of care, but other viruses as well
Researchers at the University of Central Florida (UCF) announced the development of an optical sensor that uses nanotechnology to identify viruses in blood samples in seconds with an impressive 95% accuracy. This breakthrough underscores the value of continued research into technologies that create novel diagnostic tests which offer increased accuracy, faster speed to answer, and lower cost than currently available clinical laboratory testing methods.
The innovative UCF device uses nanoscale patterns of gold that reflect the signature of a virus from a blood sample. UCF researchers claim the device can determine if an individual has a specific virus with a 95% accuracy rate. Different viruses can be identified by using their DNA sequences to selectively target each virus.
According to a UCF Today article, the University of Central Florida research team’s device closely matches the accuracy of widely-used polymerase chain reaction (PCR) tests. Additionally, the UCF device provides nearly instantaneous results and has an accuracy rate that’s a marked improvement over typical rapid antigen detection tests (RADT).
Debashis Chanda, PhD (above), holds up the nanotechnology biosensor he and his team at the University of Central Florida developed that can detect viruses in a blood sample in seconds with 95% accuracy and without the need for pre-preparation of the blood sample. Chanda is professor of physics at the NanoScience Technology Center and the College of Optics and Photonics (CREOL) at UCF. Should this detection device prove effective at instantly detecting viruses at the point of care, clinical laboratories worldwide could have a major new tool in the fight against not just COVID-19, but all viral pathogens. (Photo copyright: University of Central Florida.)
Genetic Virus Detection on a Chip
“The sensitive optical sensor, along with the rapid fabrication approach used in this work, promises the translation of this promising technology to any virus detection, including COVID-19 and its mutations, with high degree of specificity and accuracy,” Debashis Chanda, PhD, told UCF Today. Chanda is professor of physics at the NanoScience Technology Center at UCF and one of the authors of the study. “Here, we demonstrated a credible technique which combines PCR-like genetic coding and optics on a chip for accurate virus detection directly from blood.”
The team tested their device using samples of the Dengue virus that causes Dengue fever, a tropical disease spread by mosquitoes. The device can detect viruses directly from blood samples without the need for sample preparation or purification. This feature enables the testing to be timely and precise, which is critical for early detection and treatment of viruses. The chip’s capability also can help reduce the spread of viruses.
No Pre-processing or Sample Preparation Needed for Multi-virus Testing
The scientists confirmed their device’s effectiveness with multiple tests using varying virus concentration levels and solution environments, including environments with the presence of non-target virus biomarkers.
“A vast majority of biosensors demonstrations in the literature utilize buffer solutions as the test matrix to contain the target analyte,” Chanda told UCF Today. “However, these approaches are not practical in real-life applications because complex biological fluids, such as blood, containing the target biomarkers are the main source for sensing and at the same time the main source of protein fouling leading to sensor failure.”
The researchers believe their device can be easily adapted to detect other viruses and are optimistic about the future of the technology.
“Although there have been previous optical biosensing demonstrations in human serum, they still require off-line complex and dedicated sample preparation performed by skilled personnel—a commodity not available in typical point-of-care applications,” said Abraham Vazquez-Guardado, PhD, a Postdoctoral Fellow at Northwestern University who worked on the study, in the UCS Today article. “This work demonstrated for the first time an integrated device which separated plasma from the blood and detects the target virus without any pre-processing with potential for near future practical usages.”
More research and additional studies are needed to develop the University of Central Florida scientists’ technology and prove its efficacy. However, should the new chip prove viable for point-of-care testing, it would give clinical laboratories and microbiologists an ability to test blood samples without any advanced preparation. Combined with the claims for the device’s remarkable accuracy, that could be a boon not only for COVID-19 testing, but for testing other types of viruses as well.
Journalists, researchers, and a growing number of consumers now recognize the often huge variability in the prices different medical laboratories charge for the same lab tests
One step at a time, the Medicare program, private health insurers, and employers are putting policies in place that require providers—including clinical laboratories and pathology groups—to allow patients and consumers to see the prices they charge for their medical services. Recent studies into test price transparency in hospitals and health networks have garnered the attention of journalists, researchers, and patients. These groups are now aware of enormous variations in pricing among providers within the same regions and even within health networks.
Now that hospitals’ medical laboratory test prices are
required to be easily accessible to patients, researchers are beginning to compile
test prices across different hospitals and in different states to document and
publicize the wide variation in what different hospital labs charge for the
same medical laboratory tests.
Journalists are jumping on the price transparency bandwagon
too. That’s because readers show strong interest in stories that cover the
extreme range of low to high prices providers will charge for the same lab
test. This news coverage provides patients with a bit more clarity than
hospitals and other providers might prefer.
Shocking Variations in Price of Healthcare
Services, including Medical Laboratory Tests
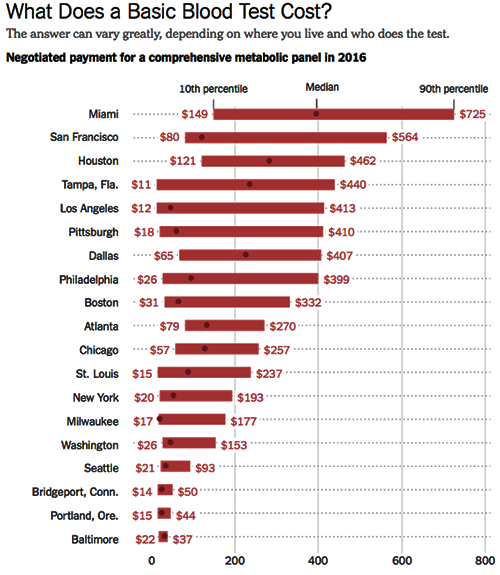
The Health Care Cost Institute (HCCI) in conjunction with the Robert Wood Johnson Foundation (RWJF), examines price levels of various procedures and medical laboratory tests at healthcare institutions across the United States in the first release of a series called Healthy Marketplace Index. According to the HCCI website, “a common blood test in Beaumont, Texas ($443) costs nearly 25 times more than the same test in Toledo, Ohio ($18).”
In April, the New
York Times (NYT) made the wide variation
in how clinical laboratories price their tests the subject of an article titled,
“They Want It to Be Secret: How a Common Blood Test Can Cost $11 or Almost
$1,000.” The article discusses the HCCI findings.
The coverage by these two well-known entities is increasing the
public’s awareness of the broad variations in pricing at clinical laboratories
around the country.
Aside from the large differences in medical laboratory test
prices in different regions, the HCCI found that there are sometimes huge price
variations within a single metro area for the same lab tests. “In just one
market—Tampa, Fla.—the most expensive blood test costs 40 times as much as the
least expensive one,” the NYT notes.
In other industries, those kinds of price discrepancies are
not common. The NYT made a comparatively outrageous example using
ketchup, saying, “A bottle of Heinz ketchup in the most expensive store in a
given market could cost six times as much as it would in the least expensive
store,” adding, however, that most bottles of ketchup tend to cost about the
same.
The graphic above is taken from the New York Times article on test price discrepancies in healthcare. The range of prices for the medical lab test known as a comprehensive metabolic panel are for metropolitan areas only. The data is sourced from the Health Care Cost Institute study. It’s easy to see why patients would be confused by clinical laboratory pricing that varies so widely. (Graphic copyright. The New York Times.)
The CMS mandate designed to make the prices of medical services accessible to healthcare consumers has, in many ways, made things more confusing. For example, most hospitals simply made their chargemaster available to consumers. Chargemasters can be confusing, even to industry professionals, and are filled with codes that make no sense to the average consumer and patient.
“This policy is a tiny step forward but falls far short of what’s needed. The posted prices are fanciful, inflated, difficult to decode and inconsistent, so it’s hard to see how an average person would find them useful,” Jeanne Pinder, Founder and Chief Executive of Clear Health Costs, a consumer health research organization, told the NYT in an article on how hospitals are complying with the mandate to publish prices.
In addition to the pricing information being difficult for
consumers to parse, it also may lead them to believe they would need to pay
much more for a given procedure than they would actually be billed, resulting
in patients opting to not get care they actually need.
Why Having a Strategy Is Critically
Important for Clinical Laboratories
Clinical laboratories are in a particularly precarious position in all of this pricing confusion. For one thing, most hospital-based medical laboratories don’t have a way to communicate directly with consumers, so they don’t have a way to explain their pricing. Additionally, articles and studies such as those in the NYT and from the HCCI, which describe drastic price variations for the same tests, tend to cast clinical laboratories in a somewhat sinister light.
To prepare for this, medical laboratory personnel should be
trained in how to address customer requests for pricing and how to explain
variations in test prices among labs, before such requests become problematic. Lab
staff should be able to explain how patients can find out the cost of a given
test, and what choices they have regarding specific tests.
In 2016, Dark Daily’s sister-publication, The Dark Report (TDR), dedicated an entire issue to the impact of reference pricing on the clinical laboratory industry. In that issue, TDR reported on how American supermarket chain Safeway helped guide their employees to lower-priced clinical laboratories for lab tests, resulting in $2.7 million savings for the company in just 24 months. Safeway simply implemented reference pricing; the company analyzed lab test prices of 285 tests for all of the labs in its network, and then set the maximum amount it would pay for any given test at the 60th percentile.
If a Safeway employee selected a medical laboratory with prices less than the 60th percentile, the normal benefits and co-pays applied. But if a Safeway employee went to clinical laboratories that charged more than the 60th percentile level, they were required to pay both their deductible and the amount above Safeway’s maximum.
Safeway’s strategy revealed wide variation in testing
prices, just as the HCCI report found. This means that employers can be added
to the list of those who are paying much closer attention to medical laboratory
test pricing than they have in the past. These are developments that should
motivate forward-looking pathologists and clinical laboratory executives to act
sooner rather than later to craft an effective strategy for responding to consumer
and patient requests for lab test price transparency.
Goal is to enable gene sequencing data to reside in EMRs, which would provide pathologists and clinical lab professionals with an opportunity to add value
More federal grant money is available to speed up research designed to make it possible to incorporate genome information into the electronic medical record (EMR). This is a development that can have both positive and negative consequences for clinical laboratories and anatomic pathology groups.
The National Institutes of Health (NIH) is awarding more than $48.6 million in grants to researchers seeking to better understand the clinical implications of genomic information and determine the best ways to deliver news to patients when their genetic data indicates they may be predisposed to certain diseases or medical conditions.
The grants are administered by the National Human Genome Research Institute (NHGRI) and represent the third phase of the Electronic Medical Records and Genomics (eMERGE) program. This is a national consortium working to move genomics research closer to clinical application by identifying the potential medical effects of rare genomic variants in about 100 clinically-relevant genes. (more…)
Accelerating pace of hospital consolidation brings new pressure to pathologists and clinical laboratory directors to maximize the value of pathology services
Large and financially-stable multi-hospital health systems are racing to form regional mega-systems. It’s a strategy to get ahead of the Affordable Care Act’s (ACA) mandate to improve quality and increase efficiency through coordinated care across the entire care continuum.
This growing national trend means further consolidation of clinical laboratory testing services within the merging organizations. For pathology groups, the new super-systems may encourage the different pathology groups within the system to consolidate into a single practice entity. This would help improve how pathology services are more deeply integrated into the care continuum. It would also facilitate contract negotiations between the pathologists and the parent health system. (more…)