Scientists reported positive Phase 1 trial results of their “intratumoral microdevice” in patients with glioma tumors
Here is an example of new microtechnology which has the potential to greatly shorten the time and improve the ability of physicians to determine which anti-cancer drug is most effective for an individual patient’s glioblastoma. As it is further developed, this technology could give anatomic pathologists and clinical laboratories an increased role in assessing the data produced by microdevices and helping physicians determine the most appropriate anti-cancer drug for specific patients.
In a news release, researchers at Brigham and Women’s Hospital (BWH) in Boston said they have developed an implantable “intratumoral microdevice” (IMD) that functions as a “lab in a patient,” capable of gauging the effectiveness of multiple drugs that target brain tumors. In a Phase 1 clinical trial, they tested the IMD on six patients with glioma tumors.
“In order to make the greatest impact on how we treat these tumors, we need to be able to understand, early on, which drug works best for any given patient,” study co-author Pier Paolo Peruzzi, MD, PhD, told the Harvard Gazette. “The problem is that the tools that are currently available to answer this question are just not good enough. So, we came up with the idea of making each patient their own lab, by using a device which can directly interrogate the living tumor and give us the information that we need.”
Peruzzi is Principal Investigator at the Harvey Cushing Neuro-Oncology Laboratories and Assistant Professor of Neurosurgery at Harvard Medical School.
“Our goal is for the placement of these devices to become an integral part of tumor surgery,” said Pier Paolo Peruzzi, MD PhD (above) of Brigham and Women’s Hospital and Harvard Medical School in an article he co-wrote for Healio. “Then, with the data that we have from these microdevices, we can choose the best systemic chemotherapy to give to that patient.” Pathologists and clinical laboratories may soon play a role in helping doctors interpret data gathered by implantable microdevices and choose the best therapies for their patients. (Photo copyright: Dana-Farber Cancer Institute.)
New Perspective on Tumor Treatments
In a news story he co-wrote for Healio, Peruzzi explained that the microdevice—about the size and shape of a grain of rice—contains up to 30 tiny reservoirs that the researchers fill with the drugs they want to test. Surgeons implant the device during a procedure to remove the tumors.
The surgery takes two to three hours to perform, and during that time, the device releases “nanodoses” of the drugs into confined areas of the tumor. Near the end of the procedure, the device is removed along with tissue specimens. The researchers can then analyze the tissue to determine the effectiveness of each drug.
“This is not in the lab, and not in a petri dish,” Peruzzi told Harvard Gazette. “It’s actually in real patients in real time, which gives us a whole new perspective on how these tumors respond to treatment.”
The Healio story notes that gliomas are “among the deadliest brain cancers and are notoriously difficult to treat.” With current approaches, testing different therapies has posed a challenge, Peruzzi wrote.
“Right now, the only way these drugs are tested in patients is through what are called window-of-opportunity studies, where we give one drug to the patient before we resect the tumor and analyze the effect of the drug,” he said. “We can only do this with one drug at a time.”
Determining Safety of Procedure
The primary goal of the Phase 1 trial was to determine the safety of the procedure, Peruzzi noted. “To be in compliance with standard clinical practice and minimize risks to the patients, we needed to integrate the placement and retrieval of the device during an otherwise standard operation.”
The trial consisted of three men and three women ranging from 27 to 86 years old, with a median age of 76. Five were diagnosed with glioblastoma and one with grade 4 astrocytoma.
“None of the six enrolled patients experienced adverse events related to the IMD, and the exposed tissue was usable for downstream analysis for 11 out of 12 retrieved specimens,” the researchers wrote in Science Translational Medicine. They noted that application of the IMD added about 32 minutes to the time required for the surgery, equating to a cost increase of $7,800.
One drug they tested was temozolomide (TMZ), “the most widely used agent in this patient population,” they wrote. “Several patients in our trial received it systemically, either before or after IMD insertion, as part of the standard of care. Thus, although our trial was not designed to choose chemotherapy agents based on IMD data, we still could compare the observed clinical-radiological response to systemic TMZ with the patient-specific response to TMZ in the IMD-exposed tissue.”
One patient, the researchers noted, had not benefited from the drug “in concordance with the poor tissue response observed in the IMD analysis.” But in another patient, a 72-year-old woman, “IMD analysis showed a marked response to TMZ,” and she survived for 20 months after receiving the treatment “with radiological evidence of tumor response. This was despite having a subtotal tumor resection, in itself an unfavorable prognostic factor. The patient expired because of an unrelated cardiovascular event, although she had remained neurologically stable.”
Drug Duration Limitation
One limitation of the study was that testing the device during the tumor removal procedure limited the duration of the drug treatments, Peruzzi said. The Harvard Gazette noted that following their initial study, the researchers were testing a variation of the procedure in which the device is implanted three days before the main surgery in a minimally invasive technique. This gives the drugs more time to work.
Cancer researchers have theorized that common treatments for tumors can impair the immune system, Peruzzi wrote in Healio. “One thing we want to look at is which drugs can kill the tumor without killing the immune system as well,” he noted.
Future studies will determine the effectiveness of implanting microdevices into tumors to test therapies in vivo. Should they become viable, clinical laboratories and anatomic pathologists will likely be involved in receiving, interpreting, storing, and transmitting the data gathered by these devices to the patient’s doctors.
Working from tissue slides similar to those used by surgical pathologists, the algorithm accurately detects prostate cancer with an impressive 98% sensitivity
It could be that a new milestone has been reached on the road to using artificial intelligence (AI) to help anatomic pathologists diagnose cancer and other diseases. A research collaboration between a major American university and an Israeli company recently published a study about the ability of an AI algorithm to correctly diagnose prostate cancer.
The scientists trained the Galen Prostate AI to recognize prostate cancer by having it examine images from over a million parts of stained tissue slides taken from patient biopsies. Expert pathologists labeled each image to teach the algorithm how to distinguish between healthy and abnormal tissue. The AI was then tested on 1,600 different tissue slide images that had been collected from 100 patients seen at UPMC who were suspected of having prostate cancer.
“Humans are good at recognizing anomalies, but they have their own biases or past experience,” said Rajiv Dhir, MD, Chief Pathologist and Vice Chair of Pathology at UPMC Shadyside Hospital, Professor of Biomedical Informatics at University of Pittsburgh, and senior author of the study, in a UPMC news release. “Machines are detached from the whole story. There’s definitely an element of standardizing care.”
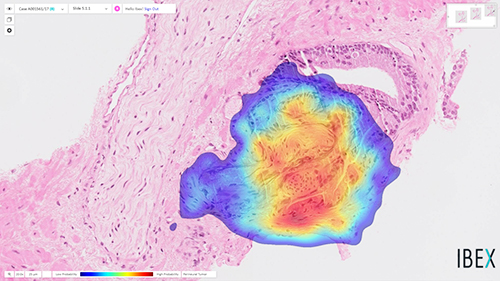
The image above is “of prostate cancer (represented by the heatmap) detected by the Ibex Galen Prostate [AI] solution on a biopsy that was previously diagnosed as benign by the pathologist,” stated an Ibex news release announcing the UPMC study. (Photo copyright: Ibex.)
UPMC Algorithm Goes Beyond Cancer Detection, Exceeds Human Pathologists
The researchers also noted that this is the first algorithm to extend beyond cancer detection. It reported high performance for tumor grading, sizing, and invasion of surrounding nerves—clinically important features of pathology reports.
“Algorithms like this are especially useful in lesions that are atypical,” Dhir said. “A nonspecialized person may not be able to make the correct assessment. That’s a major advantage of this kind of system.”
The algorithm also flagged six slides as potentially containing abnormal tissue that were not flagged by human pathologists. However, the researchers pointed out that this difference does not mean the AI is better than humans at detecting prostate cancer. It is probable, for example, that the pathologists simply saw enough evidence of malignancy elsewhere in the patients’ samples to recommend treatment.
Other Studies Where AI Detected Prostate Cancer
The UPMC researchers are not the first to use AI to detect prostate cancer. In February, The Lancet Oncology published a study from researchers at Radboud University Medical Center (RUMC) in the Netherlands who developed a deep learning AI system that could determine the aggressiveness of prostate cancer in certain patients.
For that research, the RUMC scientists collected 6,000 biopsies from more than 1,200 men. They then showed the biopsy images along with the original pathology reports to their AI system. Using deep learning, the AI was able to detect and grade prostate cancer according to the Gleason Grading System (aka, Gleason Score), which is used to rate prostate cancer and choose appropriate treatment options. The Gleason Score ranges from one to five and most cancers obtain a score of three or higher.
“Systems such as ours can be used in different ways. First, it can be used to screen biopsies and to filter out the easy (benign) cases. This could reduce the workload for pathologists,” said Wouter Bulten, a PhD candidate at Radboud who worked on the study, in an interview with HemOnc Today. “Second, the system can be used as a second opinion after the pathologist’s initial read. The system can flag a case if its opinion differs from that of the pathologist. It also can give feedback during the first read, showing the pathologist where to look. In this case, the pathologist needs only to confirm the opinion of the AI system.”
Can Today’s AI Outperform Human Pathologists?
In their research, the Radboud team discovered that their AI system was able to achieve pathologist-level performance and, in some cases, even performed better than human pathologists. However, they do not foresee AI replacing the need for pathologists, but rather emerging as another method to use in cancer detection and treatment.
“We see our system as an additional tool that the pathologist can use. Although our system performs very well, it still makes mistakes,” stated Bulten. “These mistakes are often different from those a human would make. We believe that when you merge the expertise of the pathologist with the second opinion of an AI system, you get the best of both worlds.”
According to the American Cancer Society, prostate cancer is the second most common cancer among men in the US, after skin cancer. The organization estimates there will be approximately 191,930 new cases of prostate cancer diagnosed and about 33,330 deaths from the disease in the US in 2020.
Though the UPMC study focused only on prostate cancer, the scientists believe their algorithm can be trained to detect other types of cancer as well. AI in clinical diagnostics is clearly progressing, however more studies will be required. Nevertheless, if AI can truly become a useful tool for anatomic pathologists to detect cancer earlier, we may see a welcomed reduction in cancer deaths.