Level 3 bio labs handle Ebola, smallpox and other deadly diseases, and may play a role in research into the human genome
Because of the COVID-19 pandemic, there is a concerted effort to improve public health laboratories and increase the growth of bioresearch. Clinical laboratories across the country are required by law to send specimens of certain infectious diseases to public health labs for testing and analysis. The results of those tests are then reported to the federal Centers for Disease Control and Prevention (CDC), which is working to foster robust connections and relationships between clinical labs and public health labs.
A land transaction for a 1.6-acre purchase between Dallas County and TXRE Properties closed in April. The development of the lab is expected to cost $52 million and should be completed by late 2025 with occupancy as early as January 2026.
The graphic above is an artist rendering of what the new Dallas County Health and Human Services Public Health Laboratory may look like. For some time now, Dallas County has been working to create a hub centered around infrastructure and buildings to be used for bio development and research, public health labs, and even clinical laboratories. (Graphic copyright: 5G Studio Collaborative.)
Continuing Support for HHS
“The large-scale response required for COVID-19 demonstrated the need for the acquisition that will permit the continued support of the HHS efforts in response to the ongoing safety, containment, incident response to emerging and high consequence diseases that could operate at the peak of a crisis without hindering or being hindered by other county operations,” states a Dallas County Commissioners Court Order, D Magazine reported.
“The county currently utilizes owned facilities to provide laboratory services, testing services, and other initiatives,” according to the court order. “These facilities have performance and design shortcomings and have required significant capital expenditure for their ongoing use.
“To avoid leasing space and avoid additional capital investment into deferred and ongoing maintenance, the county has been searching for a suitable location/acquisition to collocate uses/departments into a centralized, efficient, and suitable laboratory,” the court order continued.
Lab Will Conduct Research into Potentially Fatal Diseases
The facility will pursue becoming a Biological Safety Level-3 laboratory. BSL-3 labs typically conduct research or work on microbes that can cause serious and potentially fatal disease through inhalation. These labs are required to be easily decontaminated. They must also have additional safety measures, including interlocked doors, sealed windows, floors, and walls, and filtered ventilation systems.
“The core diagnostic functions are—along with safety—related to identification, containment, security, and incident response to emerging and high consequence diseases,” the court order notes.
A Georgetown University article published last year concluded there are 148 institutions with BSL-3 laboratories in the US. This number was established by identifying and totaling the number of BSL-3 facilities that published research between 2006 and 2021 using PubMed Central, a full-text archive of biomedical and life sciences journal literature at the US National Institutes of Health’s National Library of Medicine (NIH/NLM).
The creation of this new biosafety lab in Dallas is consistent with the trend of investment dollars being poured into research into the human genome. This type of research, along with the creation of new facilities, can directly lead to new biomarkers that can be utilized in clinical laboratory testing and disease prevention.
When people receive COVID-19 testing at an out-of-network facility, federal law requires insurers to pay that clinical laboratory’s posted ‘cash price’ when negotiated prices have not previously been established
In the latest example that some COVID-19 testing companies are charging significantly higher prices than others, The New York Times (NYT) recently reported that one COVID lab company with “more than a dozen testing sites” throughout the US was charging $380 for a COVID-19 rapid test that can be purchased at many drug stores for $20. Sadly, this practice, the NYT also noted, is protected by federal law.
Media reporters and the lay public are not fully aware of the long-established clinical laboratory test payment modalities that govern the daily performance of tests ordered as part of regular healthcare. Thus, when the COVID-19 pandemic hit—along with tens of billions of federal dollars to pay for SARS-CoV-2 tests—it triggered a gold rush of people wanting to get into the clinical laboratory testing business specifically to make money.
It is the bad actors in this group who are tainting the entire clinical laboratory industry with often outrageous business practices that, at best, cross ethical lines—such as overpricing tests to consumers—and at worst, represent fraudulent behavior, such as inducing medically-unnecessary tests, then submitting claims for these tests.
Even as the pandemic appears to be waning, news outlets are reporting instances of insurers being charged higher “cash prices” for tests performed by out-of-network testing laboratories. Worse yet, federal law requires insurers to pay these exorbitant prices and they are not happy about it.
In-Network versus Out-of-Network Pricing
In its report, the NYT noted that the CARES Act (H.R. 748) requires insurers to pay whatever “cash prices” out-of-network labs post online, and that this is leading to “expensive coronavirus tests” that could ultimately be reflected in future “higher insurance premiums” charged to healthcare consumers.
One company the NYT highlighted in its report is GS Labs in Omaha, Neb., a provider of COVID-19 testing throughout the US. The testing company’s COVID-19 Pricing Transparency webpage lists these prices for the following COVID-19 tests:
“Insurers are obligated to pay cash price, unless we come to a negotiated rate,” Christopher Erickson, a GS Labs Partner, told the NYT.
Negotiate or ‘Pay the Provider’s Cash Price’
In Missouri, Blue Cross and Blue Shield of Kansas City (Blue KC) has filed a lawsuit against GS Labs. “This action seeks a judgment declaring Blue KC and our members are not required to pay GS Labs’ unreasonable, inflated reimbursement demands,” according to a Blue KC news release.
However, section 3202 of the Coronavirus Aid, Relief, and Economic Security (CARES) Act “specifies the process for private health insurance plan issuers to reimburse providers of COVID-19 diagnostic tests. Specifically, a reimbursement rate negotiated for such test prior to the public health emergency declared on January 31, 2020, continues to apply for the duration of the emergency. If a reimbursement rate was not negotiated prior to the emergency declaration, an issuer may either negotiate such rate or pay the provider’s cash price.”
In its own news release, GS Labs said it has “countersued Blue KC over the insurance company’s failure to pay $9.7 million for COVID tests covered by federal law.”
According to a legal expert who spoke with the NYT, GS Labs has grounds for its test charges due to the CARES Act. “Whatever price the lab puts on their public facing website, that is what has to be paid. I don’t read a whole lot of wiggle room in it,” said Sabrina Corlette, JD, Research Professor and Co-Director of the Center on Health Insurance Reforms at Georgetown University.
“Unfortunately,” noted Loren Adler (above), Associate Director of the USC-Brookings Schaeffer Initiative for Health Policy, in a blog post, “this ‘cash price’ is not a market-determined price—it is irrelevant to patients because all options have to be made free to them by law, so there is little constraint on how high this is set by testing entities. Nor is there any reason for out-of-network entities to accept any less than this amount (other than a desire to contract in the future with the insurer for fear of a public relations backlash). Moreover, in theory the patient can still be surprise balance billed if the provider’s charge is higher than this ‘cash price,’ though it is unclear why any provider would list a ‘cash price’ lower than their charge.” (Photo copyright: The Brookings Institution.)
In his analysis, Adler suggested the law be revised to require commercial insurers to pay for COVID-19 testing at Medicare prices.
Patient Receives a $54,000 ‘Surprise’ Bill for COVID-19 Out-of-Network Test
The patient, Travis Warner, reportedly has insurance from Molina Healthcare through the federal Health Insurance Marketplace. After an employee at his company tested positive for COVID-19, Warner drove 30 miles outside of Dallas in search of COVID-19 testing sites. He eventually visiting an out-of-network free-standing emergency room in Lewisville where he received PCR diagnostic and rapid antigen tests. The results of the tests were negative for COVID-19. But the bill was a shock.
The total bill came to $56,384. Molina Healthcare paid its negotiated rate of $16,915.20 for the testing and facility fee, leaving Warner responsible for the remaining $54,000!
In the end, Warner did not have to pay the bill. Molina resolved the charge with SignatureCare and, in a statement to KHN, wrote, “This matter was a provider billing error, which Molina identified and corrected.”
For its part, SignatureCare Emergency Centers, with freestanding centers throughout Texas, said it has a “robust audit process” to flag errors and processed “thousands of records a day” at the height of the pandemic, according to KHN, which reported the business showing a $175 price for a COVID-19 test on its website.
“If the insurance company is paying astronomical sums of money for your care, that means in turn that you are going to be paying higher (insurance) premiums,” Adler told KHN.
Insurance Group Finds Price Gouging
“Price gouging on COVID-19 tests by certain providers continues to be a widespread problem,” according to a statement by America’s Health Insurance Plans (AHIP), a national association representing insurers.
AHIP has studied COVID-19 test prices since April 2020. It released a survey earlier this year which found COVID-19 test prices were on average $130. However, AHIP also found that out-of-network providers charged “significantly higher” (more than $185) for more than half (54%) of COVID-19 tests (PCR, antigen, antibody) in March 2021—a 12% increase since 2020. More than 27% of COVID-19 tests in March 2021 were done out-of-network, a 6% increase since 2020.
However, in, “COVID-19 Lab Test Prices Give Some Health Plans ‘Indigestion’,” Dark Daily’s sister publication, The Dark Report, wrote, “Interestingly, [AHIP] researchers reported that the share of COVID-19 tests claims submitted from ‘high-cost locations’—identified as hospitals and emergency departments—declined from 18% in the first three months of the pandemic to only 5% during the first three months of 2021.”
Niall Brennan, President and CEO of the Health Care Cost Institute (HCCI), told KHN, “People are going to charge what they think they can get away with. Even a perfectly well-intentioned provision like [the CARES Act] can be hijacked by certain unscrupulous providers for nefarious purposes.”
Of course, most medical laboratories priced their tests fairly and have performed them in an efficient and professional manner during the pandemic. So, it is unfortunate to learn through AHIP’s survey findings and the media that some COVID-19 testing providers are posting prices that may confuse patients and affect their health insurance premiums.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
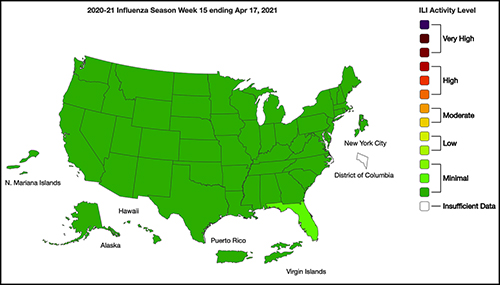
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
Pathologists and medical lab scientists may do more consults with interdisciplinary teams in connection with biomarker-based phase I clinical trial selection
Scientists are beginning to incorporate next-generation gene sequencing into a growing number of clinical trials. This is an important development because knowledge developed in clinical trials often forms the foundation for the evidence-based medicine guidelines issued following a successful clinical trial.
Further, these new uses for gene sequencing can directly lead to new opportunities for clinical laboratories and pathology groups. That’s because the increased use of gene sequencing for patients participating in clinical trials may well provide the necessary evidence to support new molecular diagnostics assays and genetic tests that physicians would use in support of therapeutic drugs cleared for market. (more…)
Mobile testing truck makes DNA testing approachable and accessible to the community while competing with established clinical laboratories
You may have seen recent news coverage of a van cruising the streets of New York City that was offering on-the-spot DNA testing with signs plastered on sides reading “Who’s Your Daddy”—“DNA Testing.” Certainlyany passing pathologist or clinical chemist might do a double take.
According to abc News coverage of the story, passersby can hail the 28-foot recreational vehicle to have their DNA tested. Of course, no testing is performed in the mobile van. Rather, a technician collects a sample from the customer, packages it, and sends it to a laboratory in Ohio for testing. Results come back in three to five days. Prices for the testing service start at $299. (more…)