Taft Foley, III, says he got the idea for the mobile lab after waiting on a COVID-19 testing line that went ‘around the entire building’
In a remarkable example of ingenuity and observation, Texas high school student Taft Foley, III, is bringing COVID-19 testing to underserved patients, wherever they may be. He launched a medical lab company, then developed a mobile clinical laboratory which performs rapid antigen tests that can detect the presence of antigen in about 15 minutes.
Foley—who recently became an EMT after graduating from the Texas EMS Academy—designed his mobile medical lab to use Quidel Sofia SARS Antigen FIA tests (nasal swabs). Results are sent to patients by text or e-mail. Foley also works with CLIA-certified Baylor Genetics Laboratories on COVID-19 (SARS-CoV-2) RT-PCR molecular testing, which gives his customers results in 24 to 48 hours, Forbes reported.
Foley, who is 18-years-old and an Eagle Scout, said he got the idea to launch the mobile COVID-19 testing business after he went for a coronavirus test and had to wait on a line that “wrapped around the entire building,” ABC13 reported. “I said to myself, ‘There needs to be a better way,’” Foley told ABC13.
Forbes reported that Texas Mobile Medical Labs allocates a portion of test fees paid ($100 to $150/test) to help provide tests to the homeless and others who need them, such as veterans and senior citizens.
“The (majority of) tests have been done at businesses who appreciate our mobile capabilities. We arrive and test all employees onsite and have their results back in 15 minutes,” Foley told Forbes.
After raising $60,000 through events and sale of personal items, Taft Foley, III (above), purchased a van and rapid antigen tests, reported The Kinkaid Falcon. “I think that that idea is hopefully going to galvanize a lot of good things, because we as humans, we’re good at learning from one another. If my idea is good enough to inspire others to create their own businesses and ideas for the betterment of the community, then I’m all for it,” Foley told the Falcon. (Photo copyright: Texas Mobile Medical Labs.)
Other States with Mobile COVID-19 Testing
Texas is not the only state where savvy entrepreneurs like Foley and health agencies are offering mobile COVID-19 testing.
In May, Florida Gov. Ron DeSantis announced Statlab Mobile, a COVID-19 mobile laboratory out of Miami that tests people in skilled nursing and long-term care facilities and other areas of the Sunshine State.
“We believe this will be a game-changer (in long-term care),” DeSantis told the Miami Herald.
“The idea was to bring help to those who are vulnerable, those who can’t otherwise get the kind of medical information they would otherwise love to have,” Bryan Wilson, Statlab Chief Executive Officer, told Patch, which noted the tests are free.
Mobile medical laboratories are being deployed to help handle surges of COVID-19 cases in Massachusetts, New Jersey, and Arizona, as well.
In Massachusetts, testing vans operated by American Family Care (AFC), an urgent care provider, started heading out in November to schools and businesses state-wide with a goal to test at least 100 to 150 people daily for COVID-19, according to The Reminder.
The vans are staffed by medical providers who test people with Abbott’s BinaxNOW COVID-19 Ag Card, AFC told The Reminder. The rapid antigen test offers results in 15 minutes.
In September, Dark Daily reported that the US federal Department of Health and Human Services (HHS) awarded a $760 million contract to Abbott for 150 million rapid antigen tests to aid in detection of COVID-19 as workplaces and schools reopen.
“We’ve had several companies who would like to schedule their employees to be tested on a regular basis. But they also want to be able to make sure that if there is a potential contamination within their businesses, they have a resource to utilize to make sure they can test people right away,” Jim Brennan, Owner/CEO of Medvest, LLC, AFC urgent care’s parent company, told The Reminder.
And in Phoenix, a COVID-19 mobile medical van provides testing to underserved communities. The City of Phoenix, along with staff from the Vincere Cancer Center, use Quidel’s Sofia SARS Antigen FIA test at public and private locations and at family services centers, AZ Central reported.
Clearly, mobile COVID-19 testing labs are here to stay. They serve seniors and vulnerable populations challenged to access clinical laboratory testing at traditional locations and at COVID-19 drive-through sites. And on larger scales, mobile medical laboratories have become key resources to address coronavirus case surges and to conveniently test people at businesses and schools to help identify symptomatic individuals who should be quarantined.
Clinical laboratory managers may be impressed by how quickly mobile testing companies and entrepreneurs form partnerships with public health agencies toward making COVID-19 tests available to all at places where people live and work.
ELISA tests at Icahn School of Medicine contradict earlier studies which found that antibodies developed to combat the SARS-CoV-2 coronavirus are short-lived
Medical laboratories at the forefront of the COVID-19 pandemic will be intrigued to learn that antibodies produced by the body to combat the coronavirus infection may actually provide long-term immunity, contrary to previous studies that found otherwise.
A recent study from the Icahn School of Medicine at Mount Sinai found that the protection may be more robust than previously believed. This may surprise many clinical laboratory scientists and clinical pathologists. Since the outbreak of the pandemic, multiple studies have been published with conflicting findings about the strength of the immune response to SARS-CoV-2 and the length of immunity provided after an infection.
In a Mount Sinai news release, however, Florian Krammer, PhD, microbiologist and Professor of Vaccinology in the Department of Microbiology at the Icahn School of Medicine at Mount Sinai, and a senior author of the paper, said, “While some reports have come out saying antibodies to this virus go away quickly, we have found just the opposite—that more than 90% of people who were mildly or moderately ill produce an antibody response strong enough to neutralize the virus, and the response is maintained for many months.”
The researchers published the findings of their study—which was based on an internally-developed antibody test—in Science.
The study concludes, “Although this cannot provide conclusive evidence that these antibody responses protect from reinfection, we believe it is very likely that they will decrease the odds ratio of reinfection and may attenuate disease in the case of breakthrough infection. We believe it is imperative to swiftly perform studies to investigate and establish a correlate of protection from infection with SARS-CoV-2.”
Florian Krammer, PhD (above), runs the Krammer Laboratory in the Department of Microbiology at the Icahn School of Medicine at Mount Sinai in New York. He noted that the longevity and neutralizing effects of antibody response are “critically important to enabling us to effectively monitor seroprevalence in communities, and to determining the duration and levels of antibody that protect us from reinfection.” Antibody response, he added, is also “essential for effective vaccine development.” (Photo copyright: Icahn School of Medicine at Mount Sinai.)
Details of the Icahn School of Medicine Study
The study arose from an effort by Mount Sinai to identify potential donors for a convalescent plasma therapy program. Beginning in late March, the health system used an enzyme-linked immunosorbent assay (ELISA) to screen thousands of individuals for presence of antibodies to the spike protein in the SARS-CoV-2 virus. The virus uses the spike protein to bind to a receptor in host cells, the researchers noted, making it “the main, and potentially only target for neutralizing antibodies.”
Screened patients either had confirmed cases of COVID-19, as determined by a polymerase chain reaction (PCR) test, or suspected cases, “defined as being told by a physician that symptoms may be related to SARS-CoV-2 or exposure to someone with confirmed SARS-CoV-2 infection,” the researchers wrote. The Mount Sinai health system also offered the test to employees.
Samples from each person were diluted in five discrete titers (concentrations) ranging from 1:80 to 1:2880, and each was tested for detectable presence of the antibodies. This allowed the researchers to categorize the samples as low, moderate, or high:
Low titers: 1:80 or 1:160
Moderate titers: 1:320
High titers: 1:960 or >1:2880
Between the start of the program and early October, the health system screened 72,401 people, of whom 30,082 tested positive for at least the lowest levels of antibodies. Among those who tested positive, a large majority fell into the moderate or high categories:
1:80: 690 (2.29%)
1:160: 1453 (4.83%)
1:320: 6765 (22.49%)
1:960: 9564 (31.79%)
1:2880: 11610 (38.60%)
The researchers also wanted to see whether the antibodies offered actual protection against the virus. So, they selected 120 samples and ran a quantitative microneutralization assay. In the lowest of the three categories, 50% of the samples showed neutralizing activity. That rose to 90% in the moderate category and 100% in the high category.
Finally, to determine how long protection might last, the researchers recalled 121 plasma donors for additional tests at two different points during the study. The researchers reported a slight drop in antibody levels about three months after onset of symptoms, and then a larger drop after five months. But antibodies were still present in most samples.
“It is still unclear if infection with SARS-CoV-2 in humans protects from reinfection and for how long,” the researchers wrote. “We know from work with common human coronaviruses that neutralizing antibodies are induced, and these antibodies can last for years and provide protection from reinfection or attenuate disease, even if individuals get reinfected.”
Previous ‘Conflicting’ Research
As previously noted, other studies raised doubts about the longevity of the antibodies produced by the body’s immune system. For example, the Mount Sinai researchers cited a study from China published in Nature Medicine that looked at the immune responses of 37 symptomatic patients and an equal number of asymptomatic individuals with laboratory-confirmed cases of the COVID-19 disease. In the latter group, 40% had no detectable levels of IgG antibodies after eight weeks.
The study also found a decrease in neutralizing antibodies in 30 of the asymptomatic individuals (81.1%) and 23 of the symptomatic individuals (62.2%) over the same period.
However, the Mount Sinai researchers pointed out that the antibody test in the Chinese study targeted a different protein. “The same paper also reported relatively stable (slightly declining) neutralizing antibody titers, which shows much higher concordance with our present findings,” they wrote. “Thus, the stability of the antibody response over time may also depend on the target antigen.”
A different study from England saw a 26% decline in antibodies over three months, CNN reported. That study, conducted by Imperial College London and Ipsos MORI, a market research firm, was based on responses from more than 365,000 randomly selected people who had self-administered a lateral flow antibody test.
But the seemingly conflicting studies from New York and the UK may not be contradictory, CNN reported. “People’s bodies produce an army of immune compounds in response to an infection and some are overwhelming at first, dying off quickly, while others build up more slowly. Measurements that show a waning antibody response in the first months after infection might be measuring this first wave—but there’s a second team building its forces in the background.”
In the same CNN report, Ania Wajnberg, MD, Director of Clinical Antibody Testing at Mount Sinai Hospital and co-author of the Icahn Mount Sinai study, said, “The serum antibody titer we measured in individuals initially were likely produced by plasmablasts—cells that act as first responders to an invading virus and come together to produce initial bouts of antibodies whose strength soon wanes.”
She added, “The sustained antibody levels that we subsequently observed are likely produced by long-lived plasma cells in the bone marrow. This is similar to what we see in other viruses and likely means they are here to stay. We will continue to follow this group over time to see if these levels remain stable as we suspect and hope they will.”
Does this mean that most people who get infected with the COVID-19 coronavirus will retain an immunity to the disease? Maybe. In the Icahn Mount Sanai study, Florian Kramer wrote, “More than 90% of people who were mildly or moderately ill produce an antibody response strong enough to neutralize the virus, and the response is maintained for many months.”
Thus, clinical laboratories engaged in serological testing may be asked to perform follow-up antibody tests to see if we do indeed create long-term immunity to COVID-19. Further, pathologists and medical laboratory scientists will want to follow future studies published in peer-reviewed journals to see if the findings of the Mount Sinai study are replicated at other sites.
CEOs of NorDx Laboratories, Sonora Quest Laboratories, and HealthPartners/Park Nicollet Laboratories expect demand for SARS-CoV-2 tests to only increase in coming months
The short answer is that large volumes of COVID-19 testing will be needed for the remaining weeks of 2020 and substantial COVID-19 testing will occur throughout 2021 and even into 2022. This has major implications for all clinical laboratories in the United States as they plan budgets for 2021 and attempt to manage their supply chain in coming weeks. The additional challenge in coming months is the surge in respiratory virus testing that is typical of an average influenza season.
Stan Schofield (above center), President of NorDx, a regional laboratory corporation that supports an integrated delivery system at MaineHealth in Portland, Maine.
Rick L. Panning (above right), MBA, MLS(ASCP)CM, retired as of Oct. 2 from the position of Senior Administrative Director of Laboratory Services for HealthPartners and Park Nicollet in Minneapolis-St. Paul, Minnesota.
Each panelist was asked how his parent health system and clinical laboratory was preparing to respond to the COVID-19 pandemic through the end of 2020 and into 2021.
First to answer was Panning, whose laboratory serves the Minneapolis-Saint Paul market.
A distinguishing feature of healthcare in the Twin Cities is that it is at the forefront of operational and clinical integration. Competition among health networks is intense and consumer-focused services are essential if a hospital or physician office is to retain its patients and expand market share.
Panning first explained how the pandemic is intensifying in Minnesota. “Our state has been on a two-week path of rising COVID-19 case numbers,” he said. “That rise is mirrored by increased hospitalizations for COVID-19 and ICU bed utilization is going up dramatically. The number of hospitalized COVID-19 patients has doubled during this time and Minnesota is surrounded by states that are even in worse shape than us.”
These trends are matched by the outpatient/outreach experience. “We are also seeing more patients use virtual visits to our clinics, compared to recent months,” noted Panning. “About 35% of clinical visits are virtual because people do not want to physically go into a clinic or doctor’s office.
“Given these recent developments, we’ve had to expand our network of specimen collection sites because of social distancing requirements,” explained Panning. “Each patient collection requires more space, along with more time to clean and sterilize that space before it can be used for the next patient. Our lab and our parent health system are focused on what we call crisis standards of care.
“For all these reasons, our planning points to an ongoing demand for COVID-19 testing,” he added. “Influenza season is arriving, and the pandemic is accelerating. Given that evidence, and the guidance from state and federal officials, we expect our clinical laboratory will be providing significant numbers of COVID-19 tests for the balance of this year and probably far into 2021.”
COVID-19 Vaccine Could Increase Antibody and Rapid Molecular Testing
Arizona is seeing comparable increases in new daily COVID-19 cases. “There’s been a strong uptick that coincides with the governor’s decision to loosen restrictions that allowed bars and exercise clubs to open,” stated Dexter. “We’ve gone from a 3.8% positivity rate up to 7% as of last night. By the end of this week, we could be a 10% positivity rate.”
Looking at the balance of 2020 and into 2021, Dexter said, “Our lab is in the midst of budget planning. We are budgeting to support an increase in COVID-19 PCR testing in both November and December. Arizona state officials believe that COVID-19 cases will peak at the end of January and we’ll start seeing the downside in February of 2021.”
The possible availability of a SARS-CoV-2 vaccine is another factor in planning at Dexter’s clinical laboratory. “If such a vaccine becomes available, we think there will be a significant increase in antibody testing, probably starting in second quarter and continuing for the balance of 2021. There will also be a need for rapid COVID-19 molecular tests. Today, such tests are simply unavailable. Because of supply chain difficulties, we predict that they won’t be available in sufficient quantities until probably late 2021.”
COVID-19 Testing Supply Shortages Predicted as Demand Increases
At NorDx Laboratories in Portland, Maine, the expectation is that the COVID-19 pandemic will continue even into 2022. “Our team believes that people will be wearing masks for 18 more months and that COVID-19 testing with influenza is going to be the big demand this winter,” observed Schofield. “The demand for both COVID-19 and influenza testing will press all of us up against the wall because there are not enough reagents, plastics, and plates to handle the demand that we see building even now.
“Our hospitals are already preparing for a second surge of COVID-19 cases,” he said.
COVID-19 patients will be concentrated in only three or four hospitals. The other hospitals will handle routine work. Administration does not want to have COVID-19 patients spread out over 12 or 14 hospitals, as happened last March and April.
“Administration of the health system and our clinical laboratory think that the COVID-19 test volume and demand for these tests will be tough on our lab for another 12 months. This will be particularly true for COVID-19 molecular tests.”
As described above, the CEOs of these three major clinical laboratories believe that the demand for COVID-19 testing will continue well into 2021, and possibly also into 2022. A recording of the full session was captured by the virtual Executive War College and, as a public service to the medical laboratory and pathology profession, access to this recording will be provided to any lab professional who contacts info@darkreport.com and provides their email address, name, title, and organization.
Robert L. Michel, Panelist—Publisher, Editor-in-Chief, The Dark Report and Dark Daily, Spicewood, Texas.
Given the importance of sound strategic planning for all clinical laboratories and pathology groups during their fall budget process, the virtual Executive War College is opening this session to all professionals in laboratory medicine, in vitro diagnostics, and lab informatics.
Financial losses for hospitals and health systems due to cancelled procedures and coronavirus expenses will lead to changes in healthcare delivery, operations, and clinical laboratory test ordering
COVID-19 is reshaping how people work, shop, and go to school. Is healthcare the next target of the coronavirus-induced transformation? According to two experts, the COVID-19 pandemic is pushing hospitals and health systems toward a “fundamental and likely sustained transformation,” which means clinical laboratories must be prepared to adapt to new provider needs and customer demands.
Burik and Fisher called attention to the staggering $50 billion-per-month loss for hospitals and health systems that was first revealed in an American Hospital Association (AHA) report published in May. The AHA report estimated a $200 billion loss from March 1, 2020, to June 30, 2020, due to increased COVID-19 expenses and cancelled elective and non-elective surgeries.
Adding to the financial carnage is the expectation that patient volumes will be slow to return. In “Hospitals Forecast Declining Revenues and Elective Procedure Volumes, Telehealth Adoption Struggles Due to COVID-19,” Burik said, “Healthcare has largely been insulated from previous economic disruptions, with capital spending more acutely affected than operations. But this time may be different since the COVID-19 crisis started with a one-time significant impact on operations that is not fully covered by federal funding.
“Providers face a long-term decrease in commercial payment, coupled with a need to boost caregiver and consumer-facing digital engagement, all during the highest unemployment rate the US has seen since the Great Depression,” he continued. “For organizations in certain locations, it may seem like business as usual. For many others, these issues and greater competition will demand more significant, material change.”
A Guidehouse analysis of a Healthcare Financial Management Association (HFMA) survey, suggests one-in-three provider executives expect to end 2020 with revenues at 15% below pre-pandemic levels, while one-in-five of them anticipate a 30% or greater drop in revenues. Government aid, Guidehouse noted, is likely to cover COVID-19-related costs for only 11% of survey respondents.
“The figures illustrate how the virus has hurled American medicine into unparalleled volatility. No one knows how long patients will continue to avoid getting elective care or how state restrictions and climbing unemployment will affect their decision making once they have the option,” Burik and Fisher wrote. “All of which leaves one thing for certain: Healthcare’s delivery, operations, and competitive dynamics are poised to undergo a fundamental and likely sustained transformation.”
As a result, the two experts predict these pandemic-related changes to emerge:
Payer-Provider Complexity on the Rise; Patients Will Struggle. As the pandemic has shown, elective services are key revenues for hospitals and health systems. But the pandemic also will leave insured patients struggling with high deductibles, while the number of newly uninsured will grow. Furthermore, upholding of the hospital price transparency ruling will add an unwelcomed spotlight on healthcare pricing and provider margins.
Best-in-Class Technology Will Be a Necessity, Not a Luxury. COVID-19 has been a boon for telehealth and digital health usage, creating what is likely to be a permanent expansion of virtual healthcare delivery. But only one-third of executives surveyed say their organizations currently have the infrastructure to support such a shift, which means investments in speech recognition software, patient information pop-up screens, and other infrastructure to smooth workflows will be needed.
“Through all the uncertainty COVID-19 has presented, one thing hospitals and health systems can be certain of is their business models will not return to what they were pre-pandemic,” Guidehouse Partner Chuck Peck, MD (above), a former health system CEO, said in a statement. “A comprehensive consumer-facing digital strategy built around telehealth will be a requirement for providers. Moreover, shifting hardware and physical assets to the cloud, and use of robotic process automation, has proven to be successful in improving back-office operations in other industries. Providers will need to follow suit.” Clinical laboratories and anatomic pathology groups should track these developments and respond appropriately to meet the changing needs of the hospitals and physicians they serve with diagnostic testing services. (Photo copyright: Athens Banner-Herald.)
The Tech Giants Are Coming. Both major retailers and technology stalwarts, such as Amazon, Walmart, and Walgreens, are entering the healthcare space. In January, Dark Daily reported on Amazon’s roll out of Amazon Care, a 24/7 virtual clinic, for its Seattle-based employees. Amazon (NASDAQ:AMZN) is adding to a healthcare portfolio that includes online pharmacy PillPack and joint-venture Haven Healthcare. Meanwhile, Walmart is offering $25 teeth cleaning and $30 checkups at its new Health Centers. Dark Daily covered this in an e-briefing in May, which also covered a new partnership between Walgreens and VillageMD to open up to 700 primary care clinics in 30 US cities in the next five years.
Work Location Changes Mean Construction Cost Reductions. According to Guidehouse’s analysis of the HFMA COVID-19 survey, one-in-five executives expect some jobs to remain virtual post-pandemic, leading to permanent changes in the amount of real estate needed for healthcare delivery. The need for a smaller real estate footprint could reduce capital expenditures and costs for hospitals and healthcare systems in the long term.
Consolidation is Coming. COVID-19-induced financial pressures will quickly reveal winners and losers and force further consolidation in the healthcare industry. “Resilient” healthcare systems are likely to be those with a 6% to 8% operating margins, providing the financial cushion necessary to innovate and reimagine healthcare post-pandemic.
Policy Will Get More Thoughtful and Data-Driven. COVID-19 reopening plans will force policymakers to craft thoughtful, data-driven approaches that will necessitate engagement with health system leaders. Such collaborations will be important not only during this current crisis, but also will provide a blueprint for policy coordination during any future pandemic.
As Burik and Fisher point out, hospitals and healthcare systems emerged from previous economic downturns mostly unscathed. However, the COVID-19 pandemic has proven the exception, leaving providers and health systems facing long-term decreases in commercial payments, while facing increased spending to bolster caregiver- and consumer-facing engagement.
“While situations may differ by market, it’s clear that the pre-pandemic status quo won’t work for most hospitals or health systems,” they wrote.
The message for clinical laboratory managers and surgical pathologists is clear. Patients may be permanently changing their decision-making process when considering elective surgery and selecting a provider, which will alter provider test ordering and lab revenues. Independent clinical laboratories, as well as medical labs operated by hospitals and health systems, must be prepared for the financial stresses that are likely coming.
Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
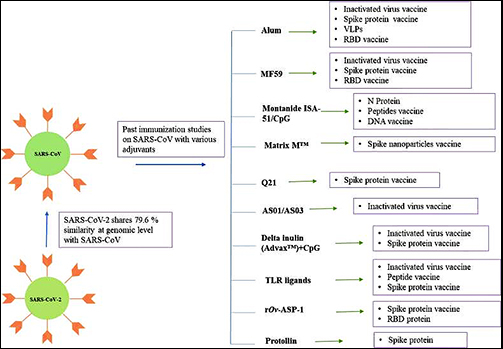
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.