From ‘new-school’ rules of running a clinical laboratory to pharmacy partnerships to leveraging lab data for diagnostics, key industry executives discussed the new era of clinical laboratory and pathology operations
Opening keynotes at the 28th Annual Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management taking place in New Orleans this week covered three main forces that healthcare and medical laboratory administrators should be preparing to address: new consumer preferences, new care models, and new payment models.
“COVID-19 didn’t change a whole lot of things in one sense, but it accelerated a lot of trends that were already happening in healthcare,” said Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and Founder of the Executive War College, during his opening keynote address to a packed ballroom of conference attendees. “Healthcare is transforming, and the transformation is far more pervasive than most consumers appreciate.
“Disintermediation, for example, is taking traditional service providers and disrupting them in substantial ways, and if you think about the end of fee-for-service, be looking forward because your labs can be paid for the value you originate that makes a difference in patient care,” Michel added.
Another opportunity for clinical laboratories, according to Michel, is serving Medicare Advantage plans which have soared in enrollment. “Lab leaders should be studying Medicare Advantage for how to integrate Medicare Advantage incentives into their lab strategies,” he said, highlighting the new influence of risk adjustment models which use diagnostic data to predict health condition expenditures.
Opening sessions at this week’s annual Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, presented by Robert L. Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, discussed demand for delivering healthcare services—including medical laboratory testing—as consumer preferences evolve, new care models are designed, and as payers seek value over volume. While these three forces may be challenging at the outset, they also create opportunities for clinical laboratories and pathology groups—a focal point of the Executive War College each year. (Photo copyright: The Dark Intelligence Group.)
Medical Laboratories Must Adapt to ‘New-School’ Rules
During his keynote address, Stan Schofield, Vice President and Managing Principal at The Compass Group, noted that while the basic “old-school” rules of successfully running a clinical laboratory have not changed—e.g., adding clients, keeping clients, creating revenue opportunities, getting paid, and reducing expenses—the interpretation of each rule has changed. The Compass Group is a trade federation based in South Carolina that serves not-for-profit healthcare integrated delivery networks (IDNs), including 32 health systems and 600 hospitals.
Schofield advised that when it comes to adding new clients under the “new-school” rules of lab management, clinical laboratory directors must be aware of and adapt to hospital integrations of core labs, clinical integrations across health systems, seamless services, direct contracting with employers in insurance relationships, and direct-to-consumer testing. Keeping clients, Schofield said, involves five elements:
Strong customer service.
A tailored metrics program for quality services based on what is important to a lab’s clients.
Balanced scorecards that look at the business opportunity and value proposition with each client.
Monitoring patients’ experiences and continuous improvement.
Participation in all payer agreements.
As to the problem of commoditization of laboratory goods and services, Schofield said, “Right now, we’re facing the monetization of the laboratory. We’re going to swiftly move from commoditization to monetization to commercialization.”
Pharmacies Enter the Clinical Laboratory Market
In another forward looking keynote address, David Pope, PharmD, CDE, Chief Pharmacy Officer at OmniSYS, XiFin Pharmacy Solutions, discussed the “test to treat” trend which could bring clinical laboratories and pharmacies together in new partnerships.
Diagnostics and pharmacy now intersect, according to Pope. “Pharmacists are on the move, and they are true contender as a new provider for you,” he said. “An area of pharmacy that is dependent upon labs is specialty medications.”
Specialty medicines now account for 55% of prescription spending, up from 28% in 2011, driven by growth in auto-immune and oncology, Pope noted. Other examples include companion diagnostics required for targeted treatments pertaining to all major cancers, and new areas like thalassemia (inherited blood disorders), obesity, next-generation sequencing, and pharmacogenomics, in addition to routine testing such as liver function and complete blood count (CBC).
Federal legislation may soon recognize pharmacists as healthcare providers who will be trained to perform specific clinical services, Pope said. Some states already recognize pharmacists as providers, he noted, explaining that pharmacies need lab data for three primary reasons:
Service—Pharmacies can act as a referral source to clinical laboratories. When referring, pharmacies may need to communicate lab test results to patients or providers to coordinate care.
Value-based care—Pharmacies would draw on data to counsel, prescribe, and coordinate care for chronic disease management, among other services.
Diagnostics and pharmacogenetics—Specialty medication workflows require documented test results within a specific timeframe prior to dispensing.
Another point Pope made: Large pharmacies are seeking lab partners. Labs that can provide rapid turnaround time and good pricing on complex tests provide pharmacies with partnership opportunities.
Using AI to Create Patients’ ‘Digital Twins’ That Help Identify Disease and Improve Care
High-tech healthcare technology underlies many opportunities in the clinical laboratory and pathology market, as evidenced throughout the Executive War College’s 2023 curriculum. An ongoing challenge for labs, however, is how to produce the valuable datasets that all labs have the potential to generate.
“It feels like we’ve come so far,” explained Brad Bostic, CEO of hc1 during his keynote address. “We’ve got the internet. We’ve got the cloud. All of this is amazing, but in reality, we have this massive proliferation of data everywhere and it’s very difficult to know how to actually put that into use. And nobody’s generating more data than clinical laboratories.
“Every single interaction with a patient that generates data gives you this opportunity to create the idea of a ‘digital twin.’ That means that labs are creating a mathematical description of what a person’s state is and using that information to look at how providers can optimally diagnose and treat that person. Ultimately, it is bigger than just one person. It’s hundreds of millions of people that are generating all this data, and many of these people fall into similar cohorts.”
This digital twin opportunity is heavily fueled by medical laboratory testing, Bostic said, adding that labs need to be able to leverage artificial intelligence (AI) to:
“I recommend lab leaders sit down with their teams and any outside partners they trust and identify what are their lab’s goals,” Bostic stated. “Think about how this technology can advance a lab’s mission. Look at strategy holistically—everything from internal operations to how patient care is affected.”
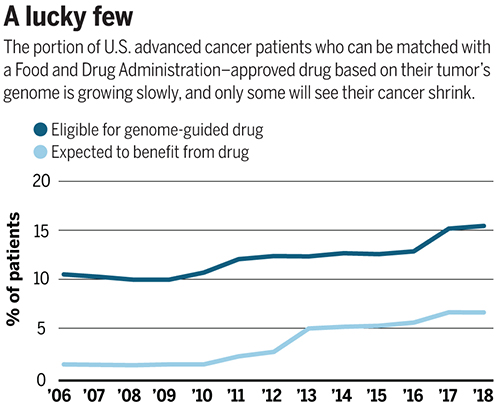
Number of patients eligible for genome-driven oncology therapy is increasing, but the percentage who reportedly benefit from the therapy remains at less than 5%
Advances in precision medicine in oncology (precision oncology) are fueling the need for clinical laboratory companion diagnostic tests that help physicians choose the best treatment protocols. In fact, this is a fast-growing area of clinical diagnostics for the nation’s anatomic pathologists. However, some experts in the field of genome-based cancer treatments disagree over whether such treatments offer more hype than hope.
Prasad and his colleagues evaluated 31 US Food and Drug
Administration (FDA) approved drugs, which were “genome-targeted” or
“genome-informed” for 38 indications between 2006 and 2018. The researchers
sought to answer the question, “How many US patients with cancer are eligible
for and benefit annually from genome-targeted therapies approved by the US Food
and Drug Administration?”
They found that in 2018 only 8.33% of 609,640 patients with
metastatic cancer were eligible for genome-targeted therapy—though this was an
increase from 5.09% in 2006.
Even more telling from Prasad’s view, his research team concluded
that only 4.9% had benefited from such treatments. Prasad’s study found the
percentage of patients estimated to have benefited from genome-informed therapy
rose from 1.3% in 2006 to 6.62% in 2018.
“Although the number of patients eligible for genome-driven treatment has increased over time, these drugs have helped a minority of patients with advanced cancer,” the researchers concluded. “To accelerate progress in precision oncology, novel trial designs of genomic therapies should be developed, and broad portfolios of drug development, including immunotherapeutic and cytotoxic approaches, should be pursued.”
The graph above is based on data from a study published in Science titled, “Estimation of the Percentage of US Patients With Cancer Who Benefit from Genome-Driven Oncology,” co-authored by Vinay Prasad, MD, MPH, et al. (Image copyright: Science.)
A Value versus Volume Argument?
Hyman, who leads a team of oncologists that conduct dozens
of clinical trials and molecularly selected “basket studies” each year,
countered Prasad’s assertions by noting the increase in the number of patients
who qualify for precision oncology treatments.
As reported in Science, Hyman said during his AACR
presentation that Sloan Kettering matched 15% of the 25,000 patients’ tumors it
tested with FDA-approved drugs and 10% with drugs in clinical trials.
“I think this is certainly not hype,” he said during the
conference.
Hyman added that another 10% to 15% of patient tumors have a
DNA change that matches a potential drug tested in animals. He expects “basket”
trials to further increase the patient pool by identifying drugs that can work
for multiple tumor types.
The US National Institute of Health (NIH) describes “basket studies” as “a new sort of clinical studies to identify patients with the same kind of mutations and treat them with the same drug, irrespective of their specific cancer type. In basket studies, depending on the mutation types, patients are classified into ‘baskets.’ Targeted therapies that block that mutation are then identified and assigned to baskets where patients are treated accordingly.”
Are Expectations of Precision Medicine Exaggerated?
A profile in MIT Technology Review, titled, “The Skeptic: What Precision Medicine Revolution?,” describes Prasad’s reputation as a “professional scold” noting the 36-year-old professor’s “sharp critiques of contemporary biomedical research, including personalized medicine.” Nevertheless, Prasad is not alone in arguing that precision oncology’s promise is often exaggerated.
“Like most ‘moonshot’ medical research initiatives,
precision medicine is likely to fall short of expectations,” Joyner wrote.
“Medical problems and their underlying biology are not linear engineering
exercises and solving them is more than a matter of vision, money, and will.”
“Although some niche applications have been found for
precision medicine—and gene therapy is now becoming a reality for a few rare
diseases—the effects on public health are miniscule while the costs are astronomical,”
they wrote.
Hope for Precision Medicine Remains High
However, optimism over precision oncology among some industry leaders has not waned. Cindy Perettie, CEO of molecular information company Foundation Medicine of Cambridge, Mass., argues genome-directed treatments have reached an “inflection point.”
“Personalized cancer treatment is a possibility for more patients than ever thanks to the advent of targeted therapies,” she told Genetic Engineering and Biotechnology News. “With a growing number of new treatments—including two pan-tumor approvals—the need for broad molecular diagnostic tools to match patients with these therapies has never been greater. We continue to advance our understanding of cancer as a disease of the genome—one in which treatment decisions can be informed by insight into the genomic changes that contribute to each patient’s unique cancer.”
Prasad acknowledges genome-driven therapies are beneficial for some cancers. However, he told MIT Technology Review the data doesn’t support the “rhetoric that we’re reaching exponential growth, or that is taking off, or there’s an inflection point” signaling rapid new advancements.
“Right now, we are investing heavily in immunotherapy and heavily in genomic therapy, but in other categories of drugs, such as cytotoxic drugs, we have stopped investigating in them,” he told Medscape Medical News. “But it’s foolish to do this—we need to have the vision to look beyond the fads we live by in cancer medicine and do things in a broader way,” he added.
“So, I support broader funding because you have to sustain
efforts even when things are not in vogue if you want to make progress,” Prasad
concluded.
Is precision oncology a fad? Dark Daily has covered the advancements in precision medicine extensively over the past decade, and with the launch of our new Precision Medicine Institute website, we plan to continue reporting on further advancements in personalized medicine.
Time will tell if precision oncology can fulfill its
promise. If it does, anatomic pathologists will play an important role in
pinpointing patients most likely to benefit from genome-driven treatments.
One thing that the debate between proponents of precision
medicine in oncology and their critics makes clear is that more and better
clinical studies are needed to document the true effectiveness of target
therapies for oncology patients. Such evidence will only reinforce the
essential role that anatomic pathologists play in diagnosis, guiding
therapeutic decisions, and monitoring the progress of cancer patients.
With $191 million in startup capital, the genomics startup will draw on existing genetic databases to create personalized medicine therapies for chronic diseases
Why do some people get sick while others do not? That’s what genetic researchers at Maze Therapeutics want to find out. They have developed a new approach to using tools such as CRISPR gene editing to identify and manipulate proteins in genetic code that may be the key to providing personalized protection against specific diseases.
If viable, the results of Maze’s research could mean the development of specific drugs designed to mimic genetic code in a way that is uniquely therapeutic to specific patients. This also would create the need for clinical laboratories to sequence and analyze patients’ DNA to determine whether a patient would be a candidate for any new therapies that come from this line of research.
Based in San Francisco, Maze Therapeutics (Maze) is studying modifier genes—genes that affect the phenotype or physical properties of other genes—and attempting to create drugs that replicate them, reported MIT Technology Review. Maze believes that genetic modifiers could afford a “natural form of protection” against disease.
“If you have a disease-causing gene, and I have the disease-causing gene, why is it that you may be healthy and I may be sick? Are there other genes that come into play that provide a protective effect? Is there a drugging strategy to recover normal phenotype and recover from the illness?” Maze Chief Executive Officer Jason Coloma, PhD, asked in an interview with FierceBiotech.
In 2019, Maze received $191 million in financing from Third Rock Ventures, ARCH Venture Partners, and others, to find ways to translate their findings into personalized medicines, according to a news release. And with the availability of international public genetic databases and CRISPR gene editing, now may be good timing.
“This was the perfect time to get into this space with the tools that were being developed and the amount of data that has been accumulated on the human genetic side,” Charles Homcy, MD, Third Rock Ventures Partner and Maze Scientific Founder, told Forbes, which noted that Maze is tapping existing population-wide genetic databases and large-scale studies, including the United Kingdom’s Biobank and Finland’s Finngen.
To help find genetic modifier drug targets, Maze is accessing CRISPR gene editing capabilities. Jonathan Weissman, PhD, Maze Scientific Founder and Professor of Cellular Molecular Pharmacology at University of California, San Francisco (UCSF), told MIT Technology Review: “You take a cell with a disease-causing gene and then see if you can turn it back to normal. We can do 100,000 experiments at once because each cell is its own experiment.”
“At Maze, we are focused on expanding our understanding of the natural disease protection provided by genetic modifiers through an integrated approach that combines studying natural human genetic variation across the globe and conducting large-scale experiments of gene perturbations,” Charles Homcy, MD (above), Founder and interim CEO of Maze and a partner at Third Rock Ventures, said in a news release. “Through our integrated approach, we believe we will create novel medicines based around those modifiers to treat a number of diseases.” (Photo copyright: Forbes.)
Using CRISPR to Identify the Cause of Disease
One drug research program reportedly progressing at Maze involves developing gene therapy for the neurogenerative disease amyotrophic lateral sclerosis (ALS). The program borrows from previous research conducted by Aaron Gitler, PhD, Professor of Genetics at Stanford University and Maze co-founder, which used CRISPR to find genetic modifiers of ALS. The scientists found that when they removed the protein coding gene TMX2 (Thioredoxin Related Transmembrane Protein 2), the toxicity of proteins building the disease was reduced, reported Chemical and Engineering News.
“We used the CRISPR-Cas9 system to perform genome-wide gene-knockout screens for suppressors and enhancers of C9ORF72 DPR toxicity in human cells,” Gitler and colleagues wrote in Nature Genetics. “Together, our results demonstrate the promise of using CRISPR-Cas9 screens in defining the mechanisms of neurodegenerative diseases.”
“We have the flexibility to think differently. We like to
think of ourselves as part of this new breed of biotech companies,” Coloma told
FierceBiotech.
It’s an exciting time. Clinical laboratories can look
forward to new precision medicine diagnostic tests to detect disease and
monitor the effects of patient therapies. And the research initiatives by Maze
and other genetic companies represent a new approach in the use of genetic code
to create specific drug therapies targeted at specific diseases that work best
for specific patients.
The companion diagnostics that may come from this research would
be a boon to anatomic pathology.
Clinical labs and pathology groups know how advances in targeted therapies and genomics far outpace providers’ and patients’ ability to know how best to use and pay for them.
One fascinating development on the road to precision medicine is that many new cancer drugs now in clinical trials will require a companion genetic test to identify patients with tumors that will respond to a specific therapeutic drug.
This implies more genetic testing of tumors, a prospect that challenges both the Medicare program and private health insurers because they already struggle to cope with the flood of new genetic tests and molecular diagnostic assays. However, even as this genetic testing wave swamps payers, some pharmaceutical companies have cancer drugs for rare types of cancers and these companies would like to see more genetic testing of tumors.
Pathologists and clinical laboratory managers will find this to be precisely the dilemma facing specialty pharma company Loxo Oncology (NASDAQ:LOXO), a biopharmaceutical company located in San Francisco and Stamford, Conn.
Loxo is developing larotrectinib (LOXO-101), a “selective TRK inhibitor.” According to a Loxo press release, Larotrectinib is “a potent, oral, and selective investigational new drug in clinical development for the treatment of patients with cancers that harbor abnormalities involving the tropomyosin receptor kinases (TRK receptors).” In short, the drug is designed to “directly target TRK, and nothing else, turning off the signaling pathway that allows TRK fusion cancers to grow.”
How to Find Patients for This Cancer Drug
While a powerful, new, targeted cancer drug will be a boon to cancer therapy, it is only intended for a relatively small number of patients. Loxo estimates that between 1,500 and 5,000 cases of cancer are caused by TRK mutations in the United States each year. Conversely, according to the National Cancer Institute, the total number of new cancer diagnoses in the US in 2016 was 1,685,210.
An article in MIT Technology Review on larotrectinib notes, “To find patients, Loxo will need to convince more doctors to order comprehensive tests that screen multiple genes at once, including TRK.” And that is where things get complicated.
“These advanced genetic tests, which can cost $5,000 or more, are offered by companies like Foundation Medicine, Caris Life Sciences, and Cancer Genetics. The problem is, insurers still consider the tests ‘experimental’ and don’t routinely cover them, meaning patients are often stuck picking up the bill,” notes MIT Technology Review.
Data for the graph above comes from theNational Human Genome Research Institute. The graph illustrates the steep decline in cost for whole genome sequencing over the past 17 years. As the cost of genetic testing drops, development of targeted-drug cancer therapies increases. Clinical laboratories and anatomic pathology groups can expect to be performing more such tests in the future. (Graphic copyright: National Human Genome Research Institute/Simple English Wiki.)
To further confuse the market, the National Cancer Institute states that “Insurance coverage of tumor DNA sequencing depends on your insurance provider and the type of cancer you have. Insurance providers typically cover a DNA sequencing test if there is sufficient evidence to support that the test is necessary to guide patient treatment. Tests without sufficient evidence to support their utility may be considered experimental and are likely not covered by insurance.”
Many reliable sources agree. For example, the US National Library of Medicine Genetics Home Reference states, “In many cases, health insurance plans will cover the costs of genetic testing when it is recommended by a person’s doctor.”
That, however, leads to a different conundrum for drug makers such as Loxo: the majority of doctors are not keeping up with the rapid-fire pace of discovery in the realm of genetics and targeted therapies. Some genes like BRCA1 and BRCA2 are familiar enough to doctors that they know how and why they are important. However, most other genes are less known, and critically, less understood by doctors who must also focus on all the other myriad aspects of patient care.
In an article on the Color Genomics $249 Hereditary Cancer Test, which tests for mutations in 30 genes, Timothy Hamill, MD, Professor Emeritus, University of California San Francisco (UCSF) Department of Laboratory Medicine, and former overall director of UCSF’s clinical laboratories, told Wired, “If you talk to docs, they say ‘BRCA, that’s the only thing I’m interested in because I don’t know what to do with the other information.’ Doctors don’t know what to do with it. Patients don’t know what to do with it.”
More Testing Equals More Knowledge
Further complicating the issue, there is an enormous lack of information on how multipanel screenings will affect individuals, public health, and the cost of healthcare in general. Several studies are underway, but they are so new it could be years before any real results become available.
Five years ago, it cost about $20,000 to sequence the whole human genome. Now the average price is $1,500, though there are more and less expensive types of genetic tests. As the cost continues to decline, however, more people will undergo the testing and scientists will learn more about how to identify the best therapy to treat cancers caused by genetic mutations.
FDA is streamlining how new diagnostic tests are approved; encourages IVD companies to focus on ‘qualifying biomarkers’ in development of new cancer drugs
It is good news for the anatomic pathology profession that new insights into the human immune system are triggering not only a wave of new therapeutic drugs, but also the need for companion diagnostic tests that help physicians decide when it is appropriate to prescribe immunotherapy drugs.
Rapid advances in precision medicine, and the discovery that a patient’s own immune system can be used to suppress chronic disease, have motivated pharmaceutical companies to pursue new research into creating targeted therapies for cancer patients. These therapies are based on a patient’s physiological condition at the time of diagnosis. This is the very definition of precision medicine and it is changing how oncologists, anatomic pathologists, and medical laboratories diagnose and treat cancer and other chronic diseases.
Since immunotherapy drugs require companion diagnostic tests, in vitro diagnostic (IVD) developers and clinical laboratory and pathology group leaders understand the stake they have in pharma companies devoting more research to developing these types of drugs.
New cancer drugs combined with targeted therapies would directly impact the future of anatomic pathology and medical laboratory testing.
Targeted Therapies Cost Less, Work Better
Targeted therapies focus on the mechanisms driving the cancer, rather than on destroying the cancer itself. They are designed to treat cancers that have specific genetic signatures.
One such example of a targeted therapy is pembrolizumab (brand name: Keytruda), a humanized antibody that targets the programmed cell death 1 (PD-1) receptor. The injection drug was primarily designed to treat melanoma. However, the FDA recently expanded its approval of Keytruda to include treatment of tumors with certain genetic qualities, regardless of the tumor’s location in the body. It was the first time the FDA has expanded an existing approval.
In a Forbes article, David Shaywitz, MD, PhD, noted that pembrolizumab had “an unprecedented type of FDA approval … authorizing its use in a wide range of cancers.” Shaywitz is Chief Medical Officer of DNAnexus in Mountain View, Calif.; Visiting Scientist, Department of Biomedical Informatics at Harvard Medical School; and Adjunct Scholar, American Enterprise Institute.
Cancers with high mutational burdens respond to the therapy because they are more likely to have what Shaywitz calls “recognizable novel antigens called mutation-associated neoantigens, or MANAs.” Such cancers include melanomas, non-small cell lung cancer, some rare forms of colorectal cancers, and others.
Such therapies require genetic sequencing, and because sequencing is becoming faster and less expensive—as is the analysis of the sequencing—the information necessary to develop targeted therapies is becoming more accessible, which is part of what’s motivating pharma research.
Biomarkers and Traditional versus Modern Drug Testing and Development
At the same time pharma is developing new immunotherapies, the FDA is recognizing the benefit of faster approvals. In an FDA Voice blog post, Janet Woodcock, MD, Director of the Center for Drug Evaluation and Research (CDER) at the FDA, wrote, “In the past three years alone, [we have] approved more than 25 new drugs that benefit patients with specific genetic characteristics … and we have approved many more new uses—also based on specific genetic characteristics—for drugs already on the market.”
In his Forbes article, Shaywitz notes that pembrolizumab’s development foreshadows a “More general trend in the industry,” where the traditional phases of drug testing and development in oncology are becoming less clear and distinct.
Along with the changes to drug development and approval that precision medicine is bringing about, there are also likely to be changes in how cancer patients are tested. For one thing, biomarkers are critical for precision medicine.
However, pharmaceutical companies have not always favored using biomarkers. According to Shaywitz, “In general, commercial teams tend not to favor biomarkers and seek to avoid them wherever possible.” And that, “All things being equal, a doctor would prefer to prescribe a drug immediately, without waiting for a test to be ordered and the results received and interpreted.”
In July, just weeks after expanding its approval for Keytruda, the FDA approved a Thermo Fisher Scientific test called the Oncomine Dx Target Test. A Wired article describes it as “the first next-generation-sequencing-based test” and notes that it “takes a tiny amount of tumor tissue and reports on alterations to 23 different genes.”
Thermo Fisher’s Oncomine DX Target Test (above) is the first multi-drug next-generation sequencing test approved by the FDA. The test is a companion diagnostic for lung-cancer drugs made by Novartis and Pfizer. (Caption and photo copyright: Thermo Fisher Scientific.)
Unlike pembrolizumab, however, the Oncomine Dx Target Test did not enjoy fast-track approval. As Wired reported, “Getting the FDA’s approval took nearly two years and 220,000 pages of data,” in large part because it was the first test to include multiple genes and multiple drugs. Thus, according to Joydeep Goswami, PhD, President of Clinical Next Generation Sequencing at Thermo Fisher, “That put the technology under extraordinary scrutiny.”
FDA Encouraging Use of Biomarkers in Precision Medicine Therapies
The FDA, however, is taking steps to make that process easier. Woodcock noted in her FDA Voice blog post that the agency is actively encouraging drug developers to “use strategies based on biomarkers.” She added that the FDA currently “works with stakeholders and scientific consortia in qualifying biomarkers that can be used in the development of many drugs.”
Additionally, in a column he penned for Wired, Robert M. Califf, MD, former Commissioner of the FDA, states that the organization has “begun to lay out a flexible roadmap for regulatory approval.” He notes, “Given the complexity of NGS [next-generation-sequencing] technology, test developers need assurance as well, and we’ve tried to reduce uncertainty in the process.”
Regulations that assist IVD developers create viable diagnostics, while ensuring the tests are accurate and valid, will be nearly as important in the age of precision medicine as the therapies themselves.
All of these developmental and regulatory changes will impact the work done by pathologists and medical laboratories. And since precision medicine means finding the right drug for the individual patient, then monitoring its progress, all of the necessary tests will be conducted by clinical laboratories.
Faster approvals for these new drugs and tests will likely mean steep learning curves for pathologists. But if the streamlined regulation process being considered by the FDA works, new immunoassay tests and targeted therapies could mean improved outcomes for cancer patients.