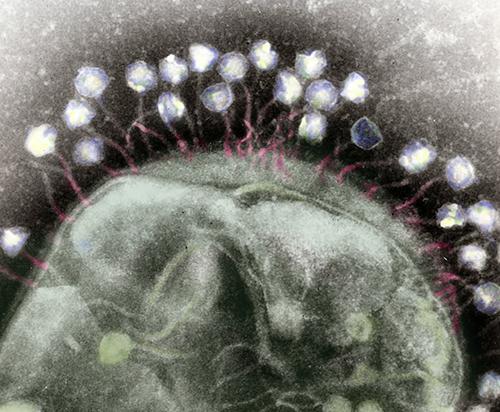
Phages are miniscule, tripod-looking viruses that are genetically programmed to locate, attack, and eradicate a specific kind of pathogen. These microscopic creatures have saved lives and are being touted as a potential solution to superbugs, which are strains of bacteria, viruses, parasites, and fungi that are resistant to most antibiotics and other treatments utilized to counteract infections.
“These multi-drug-resistant superbugs can cause chronic infections in individuals for months to years to sometimes decades,” Dwayne Roach, PhD, Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at SDSU told CNN. “It’s ridiculous just how virulent some of these bacteria get over time.”
Labs across the country are conducting research on phages in eradicating superbugs. Roach’s lab is currently probing the body’s immune response to phages and developing purification techniques to prepare phage samples for intravenous use in patients.
“There are a lot of approaches right now that are happening in parallel,” said Dwayne Roach, PhD (above), Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at San Diego State University (SDSU), in a CNN interview. “Do we engineer phages? Do we make a phage cocktail, and then how big is the cocktail? Is it two phages or 12 phages? Should phages be inhaled, applied topically, or injected intravenously? There’s a lot of work underway on exactly how to best do this.” Clinical laboratories that test for bacterial infections may play a key role in diagnosis and treatment involving bacteriophages. (Photo copyright: San Diego State University.)
Building Libraries of Phages
When certain a bacterial species or its genotypes needs to be annihilated, a collection of phages can be created to attack it via methods that enter and weaken the bacterial cell. The bacteria will attempt to counter the intrusion by employing evasive actions, such as shedding outer skins to eliminate the docking ports utilized by the phages. These maneuvers can cause the bacteria to lose their antibiotic resistance, making them vulnerable to destruction.
Some research labs are developing libraries of phages, accumulating strains found in nature in prime breeding grounds for bacteria to locate the correct phage for a particular infection. Other labs, however, are speeding up the process by producing phages in the lab.
“Rather than just sourcing new phages from the environment, we have a bioreactor that in real time creates billions upon billions of phages,” Anthony Maresso, PhD, Associate Professor at Baylor College of Medicine in Houston told CNN. “Most of those phages won’t be active against the drug-resistant bacteria, but at some point, there will be a rare variant that has been trained, so to speak, to attack the resistant bacteria, and we’ll add that to our arsenal. It’s a next-generation approach on phage libraries.”
For the Baylor study, 12 patients were treated with phages customized to each individual’s unique bacterial profile. The antibiotic-resistant bacteria were exterminated in five of the patients, while several others showed improvement.
Clinical trials are currently being executed to test the effectiveness of phages against a variety of chronic health conditions, including:
Using a phage cocktail could be used to treat a superbug outbreak in real time, while preventing a patient from a future infection of the same superbug.
“The issue is that when patients have infections with these drug-resistant bacteria, they can still carry that organism in or on their bodies even after treatment,” Maroya Walters, PhD, epidemiologist at the federal Centers for Disease Control and Prevention (CDC) told CNN.
“They don’t show any signs or symptoms of illness, but they can get infections again, and they can also transmit the bacteria to other people,” she added.
The colorized transmission electron micrograph above shows numerous phages attached to a bacterial cell wall. Phages are known for their unique structures, which resemble a cross between NASA’s Apollo lunar lander and an arthropod. (Caption and photo copyright: Berkeley Lab.)
More Studies are Needed
According to CDC data, more than 2.8 million antimicrobial-resistant (AMR) infections occur annually in the United States. More than 35,000 people in the country will die as a result of these infections.
In addition, AMR infections are a huge global threat, associated with nearly five million deaths worldwide in 2019. Resistant infections can be extremely difficult and sometimes impossible to treat.
More research is needed before phages can be used clinically to treat superbugs. But if phages prove to be useful in fighting antibiotic-resistant bacteria, microbiologists and their clinical laboratories may soon have new tools to help protect patients from these deadly pathogens.
CDC advises clinical laboratories and microbiologists encountering C. auris to follow their own protocols before adopting federal agency guidelines
In July, the Centers for Disease Control and Prevention (CDC) warned healthcare facilities and clinical laboratories to be on the alert for Candida auris (C. auris) infections in their patients. An outbreak of the drug resistant and potentially deadly fungus had appeared in two Dallas hospitals and a Washington D.C. nursing home.
Since those outbreaks, researchers have studied with urgency the “superbug’s” emergence in various types of healthcare facilities around the nation, not just hospitals. Their goal was to discover how it was successfully identified and contained.
“Seeing what was happening in New York, New Jersey, and Illinois [was] pretty alarming for a lot of the health officials in California [who] know that LTACHs are high-risk facilities because they take care of [very] sick people. Some of those people are there for a very long time,” the study’s lead author Ellora Karmarkar, MD, MSc, told Medscape. Karmarkar is an infectious disease fellow with the University of Washington and formerly an epidemic intelligence service officer with the CDC.
“One of the challenges was that people were so focused on COVID that they forgot about the MDROs (multi-drug resistant organisms] … Some of the things that we recommend to help control Candida auris are also excellent practices for every other organism including COVID care,” she added.
According to Medscape, “The OCHD researchers screened LTACH and vSNF patients with composite cultures from the axilla-groin or nasal swabs. Screening was undertaken because 5%–10% of colonized patients later develop invasive infections, and 30%–60% die.
Medscape also reported that the first bloodstream infection was detected in May 2019, and that, according to the Annals of Internal Medicine study, as of January 1, 2020, of 182 patients:
22 (12%) died within 30 days of C. auris identification,
“This is really the first time we’ve seen clustering of resistance in which patients seemed to be getting the infections from each other,” Meghan Lyman, MD, Medical Officer in the Mycotic Diseases Branch of the CDC, told Fox News.
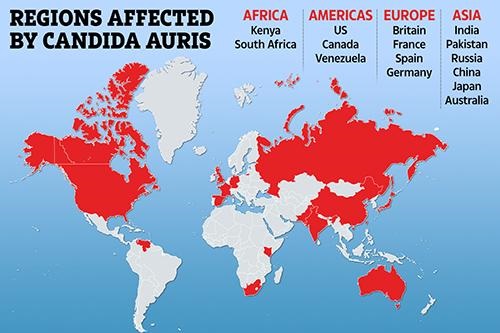
The graphic above illustrates how Candida auris is “spanning the globe,” The New York Times reported. Clinical laboratories that encounter this potentially deadly fungus are advised to contact the CDC immediately for guidance and to take proactive steps to prepare for the “superbug’s” arrival. (Graphic copyright: The Scottish Sun.)
Be More Proactive than Reactive in Identifying C. Auris, CDC Says
C. auris is a type of yeast infection that can enter the bloodstream, spread throughout the body, and cause serious complications. People who appear to have the highest risk of contracting the infection are those:
Who have had a lengthy stay in a healthcare facility,
Individuals connected to a central venous catheter or other medical tubes, such as breathing or feeding tubes, or
Have previously received antibiotics or antifungal medications.
It tends to be resistant to the antifungal drugs that are commonly used to treat Candida infections.
It can be difficult to identify via standard laboratory testing and is easily misidentified in labs without specific technology.
It can quickly lead to outbreaks in healthcare settings.
“With all this spread that we’ve been seeing across the country we’re really encouraging health departments and facilities to be more proactive instead of reactive to identifying Candida auris in general,” Lyman told STAT. “Because we’ve found that controlling the situation and containing spread is really easiest when it’s identified early before there’s widespread transmission.”
There continues to be concerns over this highly drug-resistant infection among hospital physicians and medical laboratories. “Acute care hospitals really ought to be moving toward doing species identification of Candida from nonsterile sites if they really want to have a better chance of detecting this early,” Dan Diekema, MD (above), an epidemiologist and clinical microbiologist at the University of Iowa, told Medscape. (Photo copyright: University of Iowa.)
Candia Auris versus Other Candida Infections
C. auris can cause dangerous infections in the bloodstream and spread to the central nervous system, kidneys, liver, spleen, bones, muscles, and joints. It spreads mostly in long-term healthcare facilities among patients with other medical conditions.
The symptoms of having a Candida auris infection include:
Fever
Chills
Pain
Redness and swelling
Fluid drainage (if an incision or wound is present)
General feeling of tiredness and malaise
C. auris infections are typically diagnosed via cultures of blood or other bodily fluids, but they are difficult to distinguish from more common types of Candida infections, and special clinical laboratory tests are needed to definitively diagnose C. auris.
Whole-genome Sequencing of C. Auris and Drug Resistance
The CDC conducted whole-genome sequencing of C. auris specimens gathered in Asia, Africa, and South America and discovered four different strains of the potentially life-threatening Candida species. All four detected strains have been found in the United States.
There are only three classes of antifungal drugs used to treat Candida auris infections:
However, 85% of the infections in the US have proven to be resistant to azoles and 38% are resistant to polyenes. Patients respond well to echinocandins, but more effective therapies are needed especially as some isolates may become resistant while a patient is on drug therapy, STAT reported.
“Even while it might be susceptible upfront, after a week or two of therapy, we may find that the patient has an infection now caused by an isolate of the same Candida auris that has become resistant to the echinocandins and we are really left with nothing else,” Jeffrey Rybak, PhD, PharmD, Instructor, Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, told Infection Control Today.
Although relatively rare, C. auris infections are on the rise. The good news is that there may be further pharmaceutical help available soon. New antifungal agents, such as Ibrexafungerp (Brexafemme) show promise in fighting C. auris infections, but more research is needed to prove their efficacy.
What Should Clinical Laboratories Do?
The CDC stresses that clinical laboratories and microbiologists working with known or suspected cases of Candida auris should first adhere to their own safety procedures. The CDC issued guidelines, but they are not meant to supersede the policies of individual labs.
The CDC also recommends that healthcare facilities and clinical laboratories that suspect they have a patient with a Candida auris infection immediately contact the CDC and state or local public health authorities for guidance.
In a separate study, HHS finds a 40% increase in sepsis cases, as more patients succumb to infections without effective antibiotics and antimicrobial drugs
Given the drastic steps being taken to slow the spread of the Coronavirus in America, it’s easy to forget that significant numbers of patients die each year due to antibiotic-resistant bacteria (ARB), other forms of antimicrobial resistance (AMR), and in thousands of cases the sepsis that follows the infections.
The CDC’s website states that “more than 2.8 million antibiotic-resistant infections occur in the US each year, and more than 35,000 people die as a result.” And a CDC news release states, “on average, someone in the United States gets an antibiotic-resistant infection every 11 seconds and every 15 minutes someone dies.”
Those are huge numbers.
Clinical laboratory leaders and microbiologists have learned to be vigilant as it relates to dangerously infectious antimicrobial-resistant agents that can result in severe patient harm and death. Therefore, new threats identified in the CDC’s Antibiotic Resistance Threats in the United States report will be of interest.
Drug-resistant Microbes That Pose Severe Risk
The CDC has added the fungus Candida auris (C. auris) and carbapenem-resistant Acinetobacter (a bacteria that can survive for a long time on surfaces) to its list of “urgent threats” to public health, CDC said in the news release. These drug-resistant microbes are among 18 bacteria and fungi posing a greater threat to patients’ health than CDC previously estimated, Live Science reported.
In 2013, the CDC estimated that about two million people each year acquired an antibiotic-resistant (AR) infection that killed as many as 23,000. However, in 2019, the CDC reported that those numbers were low and that the number of deaths due to AR infections in 2013 was about twice that amount. During a news conference following the CDC announcement, Michael Craig (above), a Senior Adviser for the CDC’s Antibiotic Resistance Coordination and Strategy Unit said, “We knew and said [in 2013] that our estimate was conservative … and we were right,” Live Science reported. In 2019, CDC reported 2.8 million antibiotic-resistant infections annually with more than 35,000 related deaths in the US alone. (Photo copyright: Centers for Disease Control and Prevention.)
The CDC considers five threats to be urgent. Including the
latest additions, they are:
Dark Daily has regularly covered the healthcare industry’s ongoing struggle with deadly fungus and bacteria that are responsible for hospital-acquired infections (HAI) and sepsis. This latest CDC report suggests healthcare providers continue to struggle with antimicrobial-resistant agents.
Acinetobacter Threat Increases and C. auris
a New Threat since 2013
Carbapenem-resistant Acinetobacter, a bacterium that
causes pneumonia and bloodstream and urinary tract infections, escalated from
serious to urgent in 2013. About 8,500 infections and 700 deaths were noted by the
CDC in 2017.
C. auris, however, was not addressed in the 2013
report at all. “It’s a pathogen that we didn’t even know about when we wrote
our last report in 2013, and since then it’s circumvented the globe,” said Michael
Craig, Senior Adviser for the CDC’s Antibiotic Resistance Coordination and
Strategy Unit, during a news conference following the CDC announcement, Live
Science reported.
Today, C. auris is better understood. The fungus
resists emerging drugs, can result in severe infections, and can be transmitted
between patients, CDC noted.
By year-end, CDC tracking showed 988 cases in the US.
More Patients Getting Sepsis as Antibiotics Fail: HHS
Study
In a separate study published in Critical Care Medicine, a journal of the Society of Critical Care Medicine (SCCM), the US Department of Health and Human Services (HHS) found that antibiotic-resistant bacteria and fungi are resulting in more people acquiring sepsis, a life-threatening condition, according to an HHS news release.
Sepsis increased by 40% among hospitalized Medicare patients
from 2012 through 2018, HHS reported.
“These (untreatable infections) are happening here and now in the United States in large numbers. This is isn’t some developing world thing. This isn’t a threat for 2050. It’s a threat for here and now,” Cornelius “Neil” Clancy, MD, Associate Chief of Veterans Affairs Pittsburg Health System (VAPHS) and Opportunistic Pathogens, told STAT.
It is troubling to see data about so many patient deaths
related to antibiotic-resistant infections and sepsis cases when the world is
transfixed by the Coronavirus. Nevertheless, it’s important that medical laboratory
leaders and microbiologists keep track of how the US healthcare system is or is
not responding to these new infectious agents. And, to contact infection
control and environmental services colleagues to enhance surveillance, ensure
safe healthcare environments and equipment, and adopt appropriate strategies to
prevent antibiotic-resistant infections.
As infectious bacteria become even more resistant to antibiotics, chronic disease patients with weakened immune systems are in particular danger
Microbiologists
and clinical
laboratory managers in the United States may find it useful to learn that
exceptionally virulent strains of bacteria are causing increasing numbers of cancer
patient deaths in India. Given the speed with which infectious diseases spread
throughout the world, it’s not surprising that deaths due to similar hospital-acquired
infections (HAIs) are increasing in the US as well.
Recent news reporting indicates that an ever-growing number
of cancer patients in the world’s second most populous nation are struggling to
survive these infections while undergoing chemotherapy and other treatments for
their cancers.
In some ways, this situation is the result of more powerful antibiotics. Today’s modern antibiotics help physicians, pathologists, and clinical laboratories protect patients from infectious disease. However, it’s a tragic fact that those same powerful drugs are making patients with chronic diseases, such as cancer, more susceptible to death from HAIs caused by bacteria that are becoming increasingly resistant to those same antibiotics.
India is a prime example of that devastating dichotomy. Bloomberg
reported that a study conducted by Abdul
Ghafur, MD, an infectious disease physician with Apollo Hospitals in Chennai, India,
et al, concluded that “Almost two-thirds of cancer patients with a
carbapenem-resistant infection are dead within four weeks, vs. a 28-day
mortality rate of 38% in patients whose infections are curable.”
This news should serve as an alert to pathologists, microbiologists,
and clinical laboratory leaders in the US as these same superbugs—which resist
not only antibiotics but other drugs as well—may become more prevalent in this
country.
‘We Don’t Know
What to Do’
The dire challenge facing India’s cancer patients is due to escalating
bloodstream infections associated with carbapenem-resistant
enterobacteriaceae (CRE), a particularly deadly bacteria that has become
resistant to even the most potent carbapenem antibiotics, generally
considered drugs of last resort for dealing with life-threatening infections.
Lately, the problem has only escalated. “We are facing a
difficult scenario—to give chemotherapy and cure the cancer and get a
drug-resistant infection and the patient dying of infections.” Ghafur told Bloomberg.
“We don’t know what to do. The world doesn’t know what to do in this scenario.”
Ghafur added, “However wonderful the developments in the
field of oncology, they are not going to be useful, because we know cancer
patients die of infections.”
Abdul Ghafur, MD (above), an infectious disease physician with Apollo Hospitals in Chennai, India, told The Better India that, “Indians, are obsessed with antibiotics and believe that they can cure almost all infections, including viral infections! Moreover, at least half of the prescriptions by Indian doctors include an antibiotic. Sadly, the public believes that whenever we get cold and cough, we need to swallow antibiotics for three days along with paracetamol [acetaminophen]! This is a myth that urgently needs to disappear!” (Photo copyright: Longitude Prize.)
The problem in India, Bloomberg reports, is
exacerbated by contaminated food and water. “Germs acquired through ingesting
contaminated food and water become part of the normal gut microbiome, but they can
turn deadly if they escape the bowel and infect the urinary tract, blood, and
other tissues.” And chemotherapy patients, who likely have weakened digestive
tracts, suffer most when the deadly germs reach the urinary tract, blood, and surrounding
tissues.
“Ten years ago, carbapenem-resistant superbug infections
were rare. Now, infections such as carbapenem-resistant klebsiella bloodstream
infection, urinary infection, pneumonia, and surgical site infections are a
day-to-day problem in our (Indian) hospitals. Even healthy adults in the
community may carry these bacteria in their gut in Indian metropolitan cities;
up to 5% of people carry these superbugs in their intestines,” Ghafur told The
Better India.
“These patients receive chemotherapy during treatment, which
lead to severe mucositis
of gastrointestinal tract and myelosuppression.
It was hypothesized that the gut colonizer translocate into blood circulation
causing [bloodstream infection],” the AIIMS paper states.
US Cases of C. auris Also Linked to CRE
Deaths in the US involving the fungus Candida auris (C. auris)
have been linked to CRE as well. And, people who were hospitalized outside the
US may be at particular risk.
The CDC reported on
a Maryland resident who was hospitalized in Kenya with a
carbapenemase-producing infection, which was later diagnosed as C. auris. The CDC
describes C. auris as “an emerging drug-resistant yeast of high public concern
… C auris frequently co-occurs with carbapenemase-producing organisms like
CRE.”
The graphic above, developed by the NYT from CDC data, shows that Candida auris is found globally and not restricted to poor or resource-strapped nations. “The fungus seems to have emerged in several locations at once, not from a single source,” the NYT reports. This means clinical laboratories can expect to be processing more tests to identify the deadly fungus. (Graphic copyright: New York Times/CDC.)
Drug-resistant germs are a public health threat that has
grown beyond overuse of antibiotics to an “explosion of resistant fungi,”
reported the New
York Times (NYT).
“It’s an enormous problem. We depend on being able to treat
those patients with antifungals,” Matthew Fisher, PhD,
Professor of Fungal Disease Epidemiology at Imperial College London, told the NYT.
The NYT article states that “Nearly half of patients
who contract C. auris die within 90 days, according to the CDC. Yet the world’s
experts have not nailed down where it came from in the first place.”
Cases of C. auris in the US are showing up in New York, New
Jersey, and Illinois and is arriving on travelers from many countries,
including India, Pakistan, South Africa, Spain, United Kingdom, and
Venezuela.
“It is a creature from the black lagoon,” Tom Chiller, MD,
Chief of the Mycotic
Diseases Branch at the CDC told the NYT. “It bubbled up and now it
is everywhere.”
Since antibiotics are used heavily in agriculture and
farming worldwide, the numbers of antibiotic-resistant infections will likely
increase. Things may get worse, before they get better.
Pathologists, microbiologists, oncologists, and clinical
laboratories involved in caring for patients with antibiotic-resistant
infections will want to fully understand the dangers involved, not just to
patients, but to healthcare workers as well.
Clinical laboratories and microbiologists will want to be on the alert for this deadly infectious agent that has killed patients through blood infections
Healthcare continues to struggle with the issue of how much to disclose to the public when new and deadly infectious agents are identified in a limited number of patients. Timely disclosure of new pathogens is a matter of great concern to clinical laboratory scientists, microbiologists, and clinical pathologists because their laboratories get specimens from infected patients and they must correctly identify rare or emerging pathogens to help minimize the spread of disease.
This is why many medical laboratory professionals were surprised to see national news headlines recently about a particularly deadly new form of a pathogen. The Centers for Disease Control and Prevention (CDC) has been dealing with one particularly nasty example of Candida auris, or C. auris. This “superbug” fungus has been appearing in hospitals and healthcare clinics across the globe and it has killed people.
The news coverage of C. auris focused on two
elements:
First, how the pathogen was recognized by such
healthcare agencies as the CDC.
Second, why CDC and others did not issue a
public alert to hospitals, physicians, and other caregivers once it was known
that C. auris was responsible for the death of several patients.
Once C. auris takes hold, it can enter a patient’s bloodstream or wounds and cause life- threatening complications like sepsis. When hospitals rooms are not properly decontaminated, life-threatening hospital-acquired infections (HAIs), also known as nosocomial infections, can occur.
Incidences of HAIs have been on the rise in the past few
years. Dark Dailyhas reported
on this disturbing trend many times.
The New York Times (NYT) reported on one such HAI that had tragic consequences. A patient admitted to Mount Sinai Hospital in New York for abdominal surgery was later discovered to have contracted C. auris. He was immediately isolated and spent 90 days in the hospital before passing away. Tests showed that Candida auris was everywhere in his room.
“Everything was positive—the walls, the bed, the doors, the curtains, the phones, the sink, the whiteboard, the poles, the pump,” Scott Lorin, MD, President and Chief Operating Officer at Mount Sinai Brooklyn Hospital, told the NYT. “The mattress, the bed rails, the canister holes, the window shades, the ceiling, everything in the room was positive,” he said.
The hospital had to use special cleaning equipment to
sterilize the room and even found it necessary to tear out some ceiling and
floor tiles to annihilate the fungus, the NYT reported.
Media News Coverage of ‘Culture of Secrecy’
When this deadly fungus first emerged in America, it was not
disclosed to the public for a lengthy period of time. Then, when details of
deaths in hospitals due to the superbug went public, the national news media
reacted but then went silent. Why?
In that article, the NYT states that “under its
agreement with states, the CDC is barred from publicly identifying hospitals
that are battling to contain the spread of dangerous pathogens.” So, the CDC is
prevented from revealing to the public the names and locations of facilities
that are dealing with C. auris. And state governments typically do not
share that information either.
The NYT article also states, “The CDC declined to
comment, but in the past officials have said their approach to confidentiality
is necessary to encourage the cooperation of hospitals and nursing homes, which
might otherwise seek to conceal infectious outbreaks.”
And that, “Those pushing for increased transparency say they
are up against powerful medical institutions eager to protect their
reputations, as well as state health officials who also shield hospitals from
public scrutiny.”
“Who’s speaking up for the baby that got the flu from the hospital worker or for the patient who got MRSA from a bedrail? The idea isn’t to embarrass or humiliate anyone, but if we don’t draw more attention to infectious disease outbreaks, nothing is going to change,” Arthur Caplan, PhD (above), told the NYT. Caplan is Drs. William F and Virginia Connolly Mitty Professor and founding head of the Division of Medical Ethics at NYU School of Medicine in New York City. (Photo copyright: NYU Langone Health.)
Common Yeast Infection or Killer Superbug? Both!
C. auris grows as a common yeast infection. However,
it can be life threatening if it enters the bloodstream.
“The average person calls Candida infections yeast infections,” William Schaffner, MD, Professor and Chair, Department of Preventative Medicine at Vanderbilt University Medical Center, told Prevention. “However, Candida auris infections are much more serious than your standard yeast infection. They’re a variety of so-called superbugs [that] can complicate the therapy of very sick people.”
The CDC reports that, as of May 31, 2019, there have been a total of 685 cases of C. auris reported in the US. The majority of those cases occurred in Illinois (180), New Jersey (124), and New York (336). Twenty more cases were reported in Florida, and eight other states—California, Connecticut, Indiana, Maryland, Massachusetts, Oklahoma, Texas, and Virginia—each had less than 10 confirmed cases of C. auris.
The CDC states the infection seems to be most prominent among populations that have had extended stays in hospitals or nursing facilities. Patients who have had lines or tubes such as breathing tubes, feeding tubes, or central venous catheters entering their body, and those who have recently been given antibiotics or antifungal medications, seem to be the most vulnerable to contracting C. auris.
The fungus typically attacks people who are already sick or have weakened immune systems, which can make it challenging to diagnose, the CDC notes. C. auris infections are typically diagnosed with special clinical laboratory testing of blood specimens or other body fluids. Infections have been found in patients of all ages, from infants to the elderly.
Data from the CDC indicates that C. auris can cause
bloodstream infections, wound infections, and ear infections. Common symptoms
that indicate a person has Candida auris include fever, chills,
weakness, low blood pressure, and general malaise that do not improve with
antibiotics.
“A patient’s temperature may go up, their blood pressure can
go down, and they have complications of a pre-existing illness because of Candida
auris,” Schaffner told Prevention.
The CDC reports that more than one in three patients with
invasive C. auris dies. Even though the mortality rates for Candida
auris are high, it is unclear whether patients are dying from the infection
or from their underlying illnesses. “Whatever the cause, having Candida
auris doesn’t help a patient in any way,” Schaffner noted.
The CDC states that it and its public health partners are
working hard to discover more about this fungus, and to devise ways to protect
people from contracting it. Average healthy people probably don’t need to worry
about becoming infected with Candida auris. However, individuals who are
at high risk, and healthcare professionals, microbiologists, and pathologists,
should be on the alert for this new superbug strain of fungus.