Some lab experts advise that clinical laboratories and pathology practices should also plan on delayed payments for COVID-19 testing for uninsured patients
Regardless of whether infection rates for SARS-CoV-2 continue to wane or perhaps surge again, business changes are coming for staff at clinical laboratories and anatomic pathology groups. Forward-thinking lab administrators will want to evaluate post-pandemic strategies for labs to stay ahead of potential legal issues and keep their organizations financially healthy.
The public health emergency stemming from COVID-19 is set to expire April 16. That deadline could be extended. However, the U.S. Department of Health and Human Services (HHS) is under pressure from some circles to end the public health emergency, which would affect some health insurance provisions and potentially rein in relaxed rules for telemedicine.
“If you’re a laboratory, now is the time you need to start buttoning up [the above] concerns. You don’t want to be at the mercy of a quick cutoff,” said Jon Harol, president of Lighthouse Lab Services in Charlotte, N.C. The company hosted a webinar last week called “Preparing Your Clinical Lab or Pathology Practice for Post-COVID Success.”
Pathologists and clinical laboratory leaders should consider post-pandemic strategies for labs in the following areas:
COVID-19 testing for uninsured patients;
Preparations for government audits of SARS-CoV-2 tests performed during the pandemic; and,
Repurposing PCR equipment used for COVID-19 testing into other areas of clinical diagnostics.
These strategies will be explored further during the Executive War College Conference on Laboratory and Pathology Management, which takes place April 27-29 in New Orleans. Leaders of innovative clinical laboratories will share how their lab teams are helping to improve patient outcomes while encouraging health insurers to pay them for this value.
COVID-19 Testing for Uninsured Patients
On March 22, the U.S. Health Resources and Services Administration (HRSA) announced that its COVID-19 Uninsured Program stopped accepting claims for testing and treatment due to lack of sufficient funds. This development affects 8.6% of the nation’s population that doesn’t have medical insurance, according to the U.S. Census Bureau.
For clinical laboratories, the announcement could lead to delayed payments for COVID-19 tests performed on uninsured patients, said Mick Raich, President of Revenue Cycle Management Consulting at Lighthouse Lab Services, who also spoke during the webinar. Medical laboratories and pathology groups should anticipate reimbursement gaps and how that might affect revenues collected from payers.
“The patient relationship is going to be the most important thing. That puts labs at the head of the table,” says Jon Harol, president at Lighthouse Lab Services.
“Labs are going to do the testing and are going to bill for it, and there will probably be some retroactive payment,” Raich explained.
With midterm elections happening this year, don’t be surprised to see HRSA funding reinstated for COVID-19 testing for uninsured people, commented Robert Michel, Editor-in-Chief of The Dark Report and Founder of the Executive War College.
“We’ll have to wait and see. After all, it is an election year, so the representatives and senators in Congress would like to be re-elected,” added Michel, who also presented during the webinar.
“It is reasonable to assume that members of Congress don’t want to disappoint the clinical laboratories that stepped up to the table in the earliest days of the pandemic and have done huge volumes of COVID-19 testing.”
Preparations for Government Audits of Pandemic Testing
Another post-pandemic strategy for labs: Prepare for audits of COVID-19 test claims from the HHS Office of Inspector General (OIG).
Ahead of any OIG action, labs should consider performing self-audits to determine whether they complied with HRSA requirements. “The best thing you can do is go back and look at the first two months of your billing. Do an audit to ask: Did we bill anybody with insurance by accident?” Raich suggested. “Take a hundred of those claims and audit them.”
If a medical lab finds problems with uninsured COVID-19 billing, it may be prudent to self-report those discrepancies to the government rather than ignore them. “That looks a lot better to the OIG than tucking the stuff in a desk drawer and waiting for someone to knock on your door,” Raich noted.
Harol predicted the OIG will also review another aspect of how COVID-19 test claims were coded. Auditors will want to see if PCR test claims coded for higher reimbursement if the results were reported within 48 hours actually met that requirement.
“I expect that we’ll see auditing of the coding that was used. Under COVID, you got paid more if you were running tests on a high-throughput platform. It was almost an honor system there. I don’t know that I’ve seen much outside verification of that,” Harol explained. “I’m curious to see if there will be OIG pushback and more documentation required to prove the code was correct.”
Repurposing PCR Equipment Used for COVID-19 Testing
When the pandemic finally winds down, there will be less demand for COVID-19 testing, which could leave PCR equipment collecting dust unless labs make plans now on how to repurpose those systems.
“If you have a PCR instrument that can be revalidated, you want to start thinking about putting in a panel that tests for UTIs, sexually transmitted diseases, respiratory diseases, or women’s health,” Harol explained. “Those types of tests can be done on the equipment that a lot of COVID testing was being performed on, and it can be performed by the same scientists with that same skillset. That’s the low-hanging fruit.”
The next step is more complicated: Moving into the future, clinical laboratories need to determine what menu of tests will meet the needs of patients who previously submitted COVID-19 specimens for testing.
“The patient relationship is going to be the most important thing. That puts labs at the head of the table,” Harol continued. “How can you market your laboratory services directly to patients who might be interested?”
Watch for Developments in Telemedicine
Any post-pandemic strategies for labs will be influenced by how state governments and federal health officials regulate telemedicine in the future.
Pathologists and clinical laboratory directors should keep their eyes on whether telemedicine rules revert to more onerous requirements once the public health emergency lifts. Before the pandemic, rules for physicians licensed in one state generally limited when they could practice over state lines through telemedicine.
“In response to the pandemic, both the federal government and the states relaxed many prohibitions on the practice of medicine across state lines. This is significant for pathologists,” Michel said. “There is speculation that once government officials let this genie out of the bottle regulatory-wise, they won’t be able to put it back in. Thus, there are many predictions that officials at the state and federal level will be under pressure to retain the newer telemedicine rules after the pandemic has ended.”
Telemedicine proved to be a big benefit for Medicare patients during the pandemic. A report from HHS in December indicated telehealth visits in 2020 for Medicare beneficiaries increased 63 times, from approximately 840,000 in 2019 to 52.7 million. That fact should catch the attention of clinical lab managers and pathologists who want to keep their labs at the front edge of clinical services. For Medicare beneficiaries who see their physicians virtually, labs need the capability to access that patient so as to collect the samples needed to perform those tests ordered by the physician during the telehealth consultation.
The Department of Justice steps beyond the law’s original focus on opioid-related lab testing fraud
An interesting aspect with enforcement of the Eliminating Kickbacks in Recovery Act of 2018 (EKRA) is the government’s willingness to go after charges tied to fraudulent COVID-19 testing.
The case U.S. vs. Malena Badon Lepetich provides a good example of this approach. A grand jury indicted Lepetich on various healthcare fraud charges last year, including that she allegedly offered to pay kickbacks for referrals of specimens for COVID-19 testing.
“The government had really only used EKRA in the context of addiction treatment space,” attorney Alexander Porter, a Partner at law firm Davis Wright Tremaine in Los Angeles, said in the latest issue of The Dark Report. “The Lepetich case shows that the government’s going to use EKRA beyond that context and go into other areas where they think that it can be useful—in particular, in the area of COVID-19 testing.”
Clinical laboratories and pathology groups should take note of this development.
Attorney Alexander Porter said EKRA enforcement now goes after fraudulent COVID-19 testing. (Photo: Davis Wright Tremaine)
Defendant Allegedly Filed $10 Million in Fraudulent Lab Claims
Lepetich was the owner of MedLogic, a clinical laboratory in Baton Rouge, La.
In addition to the fraudulent COVID-19 testing charges, she allegedly solicited and received kickbacks in exchange for referrals of urine specimens for medically unnecessary tests, according to the U.S. Department of Justice (DOJ).
EKRA Provisions Rose from the Opioid Crisis in the U.S.
EKRA is a criminal law that falls under the Communities and Patients Act, which lifted restrictions on medications for opioid treatment and sought to limit overprescribing of opioid painkillers. Originally, EKRA targeted fraudulent practices at sober homes and substance abuse treatment centers. However, the final draft of the bill added clinical laboratories to the list of providers under potential scrutiny.
At the time Congress passed EKRA, the law was primarily aimed at fraudulent activity in opioid treatment centers, including related lab testing.
Thus, the government’s use of EKRA in the COVID-19 charges against Lepetich case is newsworthy and establishes a precedent, noted Porter. He’ll speak about EKRA at the 2022 Executive War College on Laboratory and Pathology Management. The event takes place April 27-28 in New Orleans.
A contentious part of EKRA for clinical laboratories and pathology groups is that certain conduct protected under the federal Anti-Kickback Statute is treated as a criminal offense under EKRA. Some common lab practices come under that confusing designation, such as paying lab sales reps on a commission-based formula based on testing volumes they generate.
Proof of vaccination, masking, and availability of on-site testing will continue to be measures taken at in-person events for pathologists and medical laboratory professionals
Organizers of in-person clinical laboratory conferences face an interesting dilemma as they plan events in 2022: Where do they draw the line with COVID-19 safety protocols?
On one hand, the surge of cases caused by the SARS-CoV-2 Omicron variant seems to be in its waning stages and large swaths of the population are vaccinated. On the other hand, clinical laboratory and anatomic pathology events want potential registrants to have confidence that it is safe to travel and attend the gatherings.
One lab industry conference producer who happens to be knee-deep in preparing for an in-person meeting this spring is Robert Michel, Editor-in-Chief of The Dark Report and Founder of the 27th Annual Executive War College on Laboratory and Pathology Management. This informative event takes place on April 27-28 in New Orleans and includes COVID-19 protocols to protect attendees.
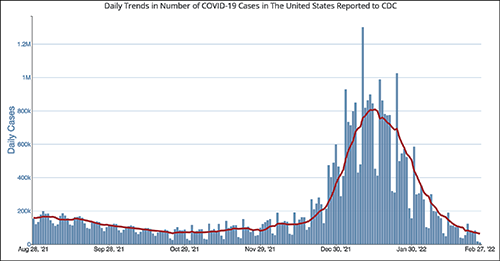
The CDC chart above shows the daily number of new COVID-19 cases in the US for the six-month period ending Feb. 28, 2022. Clinical laboratory managers should note that the number of new cases is at its lowest level since the Omicron variant showed up early this year.
“It’s important for all those planning to attend this year’s Executive War College to know that screening COVID-19 protocols will be in place to ensure the health and safety of all participants,” Michel noted. “We did a large lab conference in the fall of 2021 that included protocols for COVID-19 and the attendees told us they appreciated the protection provided by those protocols.”
After a significant rise in COVID-19 cases in January 2022 due to the Omicron variant, current daily case levels now are lower than they were six months ago before the new variant hit, according to numbers from the federal Centers for Disease Control and Prevention (CDC).
The in-person 2021 Executive War College, which took place in San Antonio on Nov. 2-3, 2021, followed the CDC’s recommendations:
COVID-19 protocols included a daily set of questions and a temperature check for all speakers and attendees before they were allowed to enter the conference area.
CLIA-complex rapid PCR COVID-19 tests were available for individuals whose temperature and answers to the screening questions indicated the need for such testing.
Attendees used an app to answer the daily screening questions and upload proof of vaccination.
“At last fall’s Executive War College, approximately 400 attendees were screened on each of the three days before entering the conference area and not one rapid COVID-19 test was needed,” Michel said. “Not only is that an outstanding outcome, but a number of attendees also told us they appreciated our efforts to keep them safe and protect their health.”
The 2022 Executive War College will follow the CDC’s updated COVID-19 guidelines, along with any state and local directives in effect as of April 27.
Although 300 attendees were expected at the 2021 Executive War College, 400 registered and participated.
Proof of Vaccination Has Been Required at Other Clinical Lab Industry Events
Organizers of other clinical lab conferences also have dealt with COVID-19 safety protocols. For example, the American Clinical Laboratory Association (ACLA) will hold its annual meeting in Washington, D.C., on March 9. COVID-19-related requirements for attendees will include proof of vaccination uploaded to a vaccine verification vendor and proof of a negative PCR test taken within 72 hours prior to the event.
The annual meeting of the American Society of Clinical Pathology (ASCP) occurs later this year in September in Chicago—too early yet to publish protocols. Last year’s ASCP conference in Boston was a hybrid event, offering both in-person and virtual options. Those who attended in person needed to upload proof of vaccination to a third-party vendor and were required to wear masks. On-site COVID-19 testing was available.
Revived Corporate Travel Could Boost Clinical Laboratory Conferences
The path back to live events across all industries has not been easy given various COVID-19 surges, political divisiveness over masking, frozen corporate travel budgets, and corporate policies banning or limiting employee travel.
Conference organizers throughout the United States universally hope those barriers will lower as 2022 progresses.
“With the fast-spreading Omicron triggering another round of setbacks to start 2022, event planners now are betting on spring to finally mark a turning point for the hard-hit industry,” MarketWatch reported on Feb. 4. “Their hopes hinge on American corporations taking a note from the recovery already under way for domestic air travel for leisure purposes, with the linchpin being a robust revival of trade show attendance and other in-person business gatherings.”
For Michel, offering actionable advice through well-thought-out sessions has been a cornerstone of the content offered each year at the Executive War College. He believes that approach will continue to be the strongest drawing point for clinical laboratory and pathology executives now considering attending the event.
“Our reading of the tea leaves is that across the profession of laboratory medicine, a great many managers, administrators, executives, and pathologists want to return to in-person conferences,” Michel noted. “Registrations for our April event are running ahead of 2019, and people tell us that they recognize the changes in healthcare and the lab marketplace because of the pandemic. They want to understand what’s driving current trends, like greater consumer involvement in lab testing and how to get private payers to reimburse claims for COVID-19 and genetic tests, as well as how a growing number of clinical laboratories are incorporating artificial intelligence solutions in both clinical care settings and lab operations.”
Self-insured and campus health markets are contract opportunities for small and midsize clinical laboratories through investment in data infrastructure and management
Bordenave spoke this week at the Executive War College in San Antonio. During two intriguing presentations, she shared that the self-insured employer and campus health markets are areas of opportunity for small and midsize clinical laboratories. This is because employer groups and college campuses are busy communities of covered individuals, and these population health groups are well-suited for proactive care models.
In fact, she said, some clinical laboratories may already be well-positioned to serve these customers.
Self-Insured Employer Groups and Campus Health Markets as New Clinical Laboratory Customers
According to CMS national health expenditure data, in 2020, a whopping $4 trillion was spent on healthcare in the US. In the middle of all that are people living, going to school, and working who have high blood pressure, rising lipid levels, lower-back pain, migraines, and other health conditions waiting to be diagnosed and flagged for follow-up.
And as pathologists and clinical laboratory managers know, 80% of those healthcare encounters result in lab test data.
Clinical laboratories, therefore, can gain customers among self-insured employer groups and similarly functioning campus health markets that serve students.
During her presentations at the 2021 Executive War College in San Antonio, Kristine Bordenave, MD, FACP (above), a strategic consultant in precision medicine, population health, Medicare compliance, and cost management, noted that “just about all paths forward post-COVID will require the data infrastructure of clinical laboratories to achieve an advanced level of functionality.” (Photo copyright: The Dark Intelligence Group.)
In one example she gave during her presentation, Bordenave noted that self-insured employer groups “were more than willing to contract directly, and they were contracting for care that directly relates to lab. Anything that would help reduce presenteeism and absenteeism with their employees.”
Presenteeism and Absenteeism
For years, presenteeism and absenteeism have plagued employee productivity in organizations large and small. Both have been attributed to numerous individual health and wellness factors among individuals. At some point, these issues culminate into various forms of reactive healthcare services and safety issues, she added.
The cost of presenteeism is estimated at between $150 billion and $225 billion. Meanwhile, at least 60% of employees are now covered in fully-funded or partially-funded self-insured plans, Healthcare Finance reported.
The way a campus health system operates is similar to a self-insured model but more of an integrated delivery system, Bordenave said. Among the priorities are controlling the spread of infectious diseases, such as COVID-19 and measles.
Clinical Laboratory Data Valuable in Treating-to-Goal and Closing Care Gaps
During two featured Executive War College general session discussions, Bordenave explained the focus of her work: aligning primary care with the clinical laboratory to treat-to-goal and close care gaps.
“There was a lot of focus on us taking laboratory information and treating people to goal, and that was with respect to diabetes, cholesterol, and hypertension, because those are three common diseases that exist within their [employee] populations. [Primary care doctors] know [that] if they [can] maximize the care in those patients—so that the patient is maximally treated—that patient performs. There’s a lot of literature around this.”
In the state of New Mexico where Bordenave’s project evolved, a culture of innovation prevails, where like-minded people have an opportunity to “do the unique,” she explained. The state’s population is spread out, there is a shortage of healthcare providers, and people generally lack access to health services and other social determinants of health. The liberty to think outside the box—to ensure care in creative ways—was essential to the success of Bordenave’s project.
“Blue Cross Blue Shield paid handsomely for improving healthcare outcomes in diabetes,” she said, adding, “and we never did a standard visit with any of those patients, ever. Then we got paid by a big employer group to do the same thing for them.”
Future of Clinical Laboratory Functionality
Bordenave noted that just about all paths forward post-COVID will require the data infrastructure of clinical laboratories to achieve an advanced level of functionality. Dark Daily will cover more opportunities for labs to capitalize on their structured data in future ebriefings.
Executive War College is scheduled to reconvene April 27-28, 2022, in New Orleans. In the meantime, recordings of this year’s presentations will be available for download, including:
A Roundtable Discussion on Current Activity Involving Clinical Laboratory and Pathology Mergers and Acquisitions.
Taking a Deeper Dive into How Artificial Intelligence Analyzes a Digital Pathology Image: What Current Technology Can and Cannot Do, Steps to Implement, and Understanding How the FDA Views AI in Digital Pathology.
Open Conversation About the Healthcare Data Aggregation Hub Model.
And more.
To learn about Executive War College’s complete program package, send an email request to info@darkreport.com.
Speakers at this week’s Executive War College in San Antonio explained that the way records are collected and stored plays a large part in the long-term usefulness of clinical laboratory data
Data structure as a term may not flow off the lips of clinical laboratory and pathology laboratory managers, but it should be top-of-mind. Well-structured data improves reimbursements and, in aggregated form, can be an enticing avenue to partnerships with outside parties.
Data structure refers to the makeup of digital records—in other words, how data is collected, stored, and accessed. Structured information offers consistency and is easier to analyze and share.
“You have to make sense of all that messy data, and that’s a heavy lift,” she said. “Results are not standardized.”
Appeals Payments Increase with More Clinical Data
Data quality can improve claim reimbursement appeals, Goede noted. When a more complete clinical record is provided to payors, they are more likely to reimburse for services.
According to information Goede covered along with Julie Ramage, Director of Precision Medicine Quality Initiatives and Partnerships at biopharmaceutical company AstraZeneca, when appealing a denied claim for a colon cancer molecular test, for example, the average appeal payment was $318 without cross-specialist clinical records.
Meanwhile, payment for a similar claim appeal which included that added data jumped to $612!
This information is often available, but may not be structured in a way that makes it easy to share with a payer. “You really have to be thinking about what elements you need,” Goede said.
Market for Structured, Anonymized Lab Data
Clinical laboratories that want to provide or sell anonymized, aggregated data to outside parties—such as research firms or pharmaceutical companies—also need to pursue efficient data structure. The re-use of existing, high-quality lab data can create a new business revenue stream.
“But it has to be more than that vanilla, male/female, date-of-birth stuff,” Ramage noted.
For example, she said, genetic testing builds up data registries, and that’s what pharma is looking for to find patients early on.
“If you don’t have a way to structure your data, you’re not going to be able to play in the sandbox,” she added.
Co-presenters Julie Ramage (left), Director of Precision Medicine Quality Initiatives and Partnerships at AstraZeneca Pharmaceuticals, and Patricia Goede, PhD (right), Vice President of Clinical Informatics at XIFIN, Inc., answer attendee questions about data structure during their presentation at this week’s Executive War College Conference on Laboratory and Pathology Management in San Antonio. To register for EWC 2022 and receive a special early-bird rate, click here by November 6.
How Clinical Laboratories Can Improve Clinical Data Structure
Here are some tips for clinical laboratory executives to consider as they tackle data structure:
Standardize how to enter patient information and test results. A common problem with data input is that the same information is entered differently over time. For example, various patient records might refer to dates in different ways: November 1, 2021, can also be entered as 11/1/21, 11/1/2021, or 11-01-21. Structured data uses a single way to list dates in records. This lesson applies to all similar clinical data.
Use dropdown menu choices instead of free-typing, open fields. An online box to enter a test result can create a variety of entries that affect data structure. While not perfect, drop-down options create a consistent set of entries, Goede said.
Ask patient advocacy groups about common nomenclature. Clinical laboratory data should reflect how patients speak, Ramage said. For example, do patients refer to genomic and genetic testing as the same thing? Establishing more consistency improves data structure as records are updated.
Enlist your organization’s IT or research team for help. Tech workers and principal investigators can easily look at clinical laboratory data and tell what information is missing or inconsistent, said Cheryl Schleicher, Director of IT Strategy at Northwell Health Labs in Lake Success, NY. Schleicher attended this week’s Executive War College.
Look Further into Clinical Laboratory Data Structure
Data structure can help clinical laboratories and pathology laboratories grab more reimbursement dollars and potentially sell anonymized data to external partners.
It is an area many lab executives are not familiar with and need to investigate more, particularly following the accelerated move to digital lab services during the COVID-19 pandemic. Your organization’s IT department or Chief Information Officer can be a useful ally.
If you could not make it to this week’s Executive War College, then join us for our next Executive War College on April 27-28, 2022, in New Orleans. Click here to take advantage of special early-bird pricing for this critical event.
Intriguing technology may find immediate value in assisting the detection and tracking of COVID-19 worldwide
Pathologists and clinical laboratory personnel old enough to have watched Star Trek on television will recall the tricorder, a multi-functional handheld device that could non-invasively detect any disease or medical condition that the science fiction series needed to be revealed. Fiction, yes, but so was the Star Trekcommunicator before the advent of smartphones.
Now, Florida-based Advanced Medical Solutions International (AMSI) anticipates bringing to market in early 2022 a similar tricorder-like handheld device that detects SARS-CoV-2 in humans and on contaminated objects and surfaces.
AMSI’s COVID Hunter™ device would be the world’s first noninvasive touchless viral detector for COVID-19, which has reportedly killed 4.55 million people worldwide. The inventors make the point that the device is simply to detect the presence of the coronavirus. It is not a diagnostic test.
For clinical laboratory scientists, this is yet another example of new technology being applied to a clinical problem that could ultimately lead to new diagnostic tools, not only for COVID-19, but ultimately for other viruses as well.
Pictured above is the actual COVID Hunter™ device that was extensively used in testing around the world. According to AMSI, this breakthrough technology can immediately detect COVID-19 in a person’s throat, lungs, sinuses, and breath, or on skin or clothes. High-touch areas such as door handles, mobile phones, and desktops also could be routinely checked for the virus and sanitized, breaking the transmission chain. (Photo copyright: Advanced Medical Solutions International.)
According to the COVID Hunter™ website, the device’s proprietary detection method utilizes a US-patent-pending detection technology that was initially invented by Engineer Nassar Said, a partner and inventor at AMSI. The method for detecting SARS-CoV-2 (the coronavirus that causes COVID-19) utilizes the above patent-pending detection technology and was invented and developed by Nassar Said and Adeeb Al-Zoubi, PhD, immunologist, and AMSI co-founder and Chief Scientific Officer.
According to the inventors, the detection technology employed by the COVID Hunter™ utilizes a combination of radio frequency (RF) and infrared (IR) electromagnetic waves to detect the RNA and spike protein found in the SARS-CoV-2 coronavirus with greater than 99% specificity and 99% sensitivity from as far as six feet away.
Al-Zoubi described the groundbreaking technology in a January 2021 news conference introducing the device. “This patent-pending technology uses a unique combination of light waves and sound waves combined to hone in on specific physical, chemical, and biological characteristics of SARS-CoV-2,” he said.
“We are basically surrounding the virus and characterizing the virus on all its characteristics all at once,” he continued. “Through focused research and tireless work, we at AMSI and Stem Cells Arabia [a Jordanian scientific research company] analyzed and specified these physical, chemical, and biological characteristics of SARS-CoV-2 and used these characteristics as one single value to target the detection by the COVID Hunter™.
“The sum of these specific SARS-CoV-2 characteristics is not found in any other virus or any other targets and constitutes a unique thumbprint of the virus,” he added.
“The handheld COVID Hunter™ will revolutionize the way SARS-CoV-2 (including mutated strains) is detected, slowing the spread of the deadly virus, saving lives, and returning life to ‘normal’ in the near future,” said AMSI co-founder and CEO Donald Redman (above center), with technology inventor/AMSI partner Nassar Said (left) and AMSI co-founder/Chief Scientific Officer and COVID Hunter™ co-inventor Adeeb Al-Zoubi, PhD (right), in a news release.
The COVID Hunter™ introductory press conference noted:
The COVID Hunter™ showed 100% accuracy and 100% specificity to detect only SARS-CoV-2 positive samples, distinguishing COVID-19 from viruses such as SARS-CoV-1, MERS, Influenza, and HIV,
The COVID Hunter™ detected all PCR positive COVID-19 test samples among more than 4,000 nasal swabs.
When more than 1,000 human subjects were tested with both PCR testing and the COVID Hunter™, the device confirmed as positive all confirmed COVID-19 cases.
4.8% of PCR false negatives in human subjects were accurately detected by the COVID Hunter™ as COVID-19 positive, indicating superior sensitivity to PCR testing.
76 out 94 confirmed COVID-19 positive individuals were shown to be infective, meaning they could transmit the disease.
The COVID Hunter™ was able to track the mode of transmission of COVID-19 as the virus moved from hand to mouth to other people and objects. Developers found that a healthy individual who shook hands with an infected person could transmit the virus to a third party without becoming infected themselves.
Researchers detected COVID-19 on the feet of domestic pets, indicating pets could transmit the virus to multiple persons within a household.
Al-Zoubi said nine months of research and development resulted in several COVID Hunter™ prototypes that demonstrated accuracy, specificity, and sensitivity in experiments using both nasal swab samples and confirmed COVID-19 patients residing in quarantine areas and hospitals in different countries.
“I am excited to see the COVID Hunter™ go from the prototype phase to a fully refined manufactured device that can be used to save lives around the world,” Al-Zoubi said in his concluding remarks.
Mass Production of COVID-Hunter
In an exclusive interview with Dark Daily, Redman and Al-Zoubi said they are seeking additional investor backing so they can shift from product refinement to high-volume manufacturing. If funding is secured this fall, their goal is to begin production in January 2022 of up to 30,000 units per month, which are projected to sell for $3,000 per device. Initially, the COVID Hunter™ would be marketed only as a COVID-19 detection tool under Federal Trade Commission (FTC) regulations.
Once manufacturing begins, AMSI will be able to submit the required number of COVID Hunter™ devices to the federal Food and Drug Administration (FDA) for review, the final step in its application for Emergency Use Authorization (EUA) of the COVID Hunter™ as a COVID-19 diagnostic device. The company expects its expedited EUA review to be completed by early spring.
AMSI notes that COVID Hunter™ can perform up to 300 scans per hour and does not use consumables other than batteries. This, according to Al-Zoubi, makes it a game-changing device for the travel industry, schools, businesses, restaurants, professional sports franchises, and concert venues seeking a return to “normal” operations.
The COVID Hunter™ also will be capable of being updated online to precisely detect new virus mutations, making it a critical weapon to defeat the pandemic as new COVID-19 mutations are found.
“This device is highly tested and it’s much more accurate than PCR [testing] because it detects the virus based on the physical presence of the virus, not based on chemical reactions or antibodies,” Al-Zoubi told Dark Daily. “We have gone beyond proof-of-concept testing.”
Clinical pathologists will want to follow development of the COVID Hunter™ and see if it eventually receives FDA approval. It may fulfill its promise as a game-changing new technology, not just for detection, but also for diagnosis.
The inventors and developers of the COVID Hunter™ will present their technology and its potential uses in detection and diagnosis at the upcoming Executive War College on Laboratory and Pathology Management, which takes place at the San Antonio Hyatt Riverwalk Hotel on Nov. 2-3, 2021.
Adeeb Al-Zoubi, PhD, and Nassar Said will conduct the session titled “New Technology Preview: Meet the COVID Hunter™, a Non-Invasive, Touchless, Immediate, and Portable Detection Device That Identifies the SARS-Cov-2 Virus.”
Medical laboratory professionals interested in attending this informative presentation can register by clicking here or by copying https://www.executivewarcollege.com your browser.