New EHR installations may require new laboratory information system upgrades and interfaces
Electronic health record (EHR) systems continue to be one of the costliest investments healthcare providers can make. And the company that holds the largest portion of the EHR market is Epic, with anywhere from 36% to 44%, according to various published reports and research briefs.
Healthcare executives remorseful about the cost of their hospital’s EHR may take solace in Becker’s Health IT’s recent list of the “most expensive” Epic EHR installations. It is common for the largest projects to cross the $1 billion mark.
Clinical laboratory leaders tasked with interfacing their hospital’s laboratory information system (LIS) with their healthcare system’s EHR may find the following information useful. The investment in time begins months before the actual EHR implementation.
One example is Lake Charles Memorial Health System (LCMHS) Lake Charles, La. In a blog post, the health system reported that it took 18 months for its physicians, clinicians, and staff to prepare for the installation of their new Epic MyChart EHR.
“There are lots of things we wish our customers would do to make sure their system runs well. Making sure every user is trained, for example. Putting in upgrades quickly. Making sure that the hardware runs fast enough,” wrote Judy Faulkner, Epic founder and CEO, in an Epic blog post.
“The LCMHS staff and physicians have championed this project from the beginning, and I have them to thank for the success of this EMR transition and look forward to seeing the positive impacts as we settle into the operational changes and new experiences Epic brings Lake Charles Memorial Health System and those we serve,” said Devon Hyde (above), President and CEO of Lake Charles Memorial Health System, about the provider’s transition to a new Epic MyChart EHR. (Photo copyright: Lake Charles Memorial Health System.)
Top 10 Most Expensive Epic EHR Installs of 2024
While Becker’s noted that the following compilation is “not an exhaustive list,” here’s its list of the top 10 most expensive Epic EHR projects based on publicly available sources.
KLAS reported that among the healthcare leaders KLAS interviewed:
27% had “an above-average EHR post-implementation” likely due to “providing technological foundation needed” at go-live, while,
40% said implementation of the EHR “had significant misses” and,
22% reported “average satisfaction with room for improvement.”
Providing staff with adequate training may smooth the way for new EHRs, according to the KLAS report. “Often, leaders wish they had invested in more training time and workflow-specific training in the context of patient care,” the authors wrote.
New EHR May Mean New LIS
Pathologists and clinical laboratory leaders may need to transition the laboratory information system (LIS) when the healthcare organization moves to a new EHR. At the very least, new interfaces will be required.
While a new EHR and LIS requires significant investments, they also provide opportunities for needed upgrades, competitive advantage, and security.
Pathologists and clinical laboratories will play a key role in collecting the data needed to create a person’s digital twin
Digital twins is a promising new technology that is making a big impact in healthcare. This development is significant because clinical laboratory test results will be among the most important sets of data to go into the creation of a patient’s “digital twin.”
A digital twin is defined by IBM as “a virtual representation of an object or system designed to reflect a physical object accurately. It spans the object’s lifecycle, is updated from real-time data, and uses simulation, machine learning, and reasoning to help make decisions.”
“We define a digital twin for healthcare as a virtual representation of a person which allows dynamic simulation of potential treatment strategy, monitoring and prediction of health trajectory, and early intervention and prevention, based on multi-scale modeling of multi-modal data such as clinical, genetic, molecular, environmental, and social factors, etc.,” wrote the authors of a review article published in NPJ Digital Medicine titled, “Digital Twins for Health: A Scoping Review.”
“The concept of digital twin for health (DT4H) holds great promise to revolutionize the entire healthcare system, including management and delivery, disease treatment and prevention, and health well-being maintenance, ultimately improving human life,” wrote study lead Eva Katsoulakis, MD (above), clinical informaticist and radiation oncologist at Tampa General Hospital in Florida, et al, in a review article she and her team published in NPJ Digital Medicine. Clinical laboratory test data will be a key element in the creation of a patient’s digital twin. (Photo copyright: Tampa General Hospital.)
Development of Digital Twins
Something akin to digital twins was first used in 1960 at NASA when replicas of spacecrafts currently on a mission in space were duplicated and studied on Earth. In 1991, Michael Grieves introduced the concept to manufacturing while at University of Michigan’s College of Engineering. The technology was later coined “digital twins” by John Vickers, a principal technologist in advanced manufacturing at NASA in 2010, IBM noted.
The increased use of digital twins in healthcare has brought some brilliant advancements. Examples, as reported by Computer Weekly, include:
Surgery and treatment: Boston Children’s Hospital uses digital twins to examine the complexities of heart procedures in reference to oxygen, blood flow, and valve pressure. Real-time analysis helps with surgeries and treatments, allowing clear visualization at all angles.
Metabolic analysis to tackle kidney failures: Digital twins are being used in Singapore to “Replicate metabolic fluxes to predict chronic kidney disease in type 2 diabetes mellitus.” Doctors there hope to curb the spike of chronic kidney disease found in type 2 diabetes mellitus. Their country has seen cases double in the last 40 years.
Bacterial predictions, E. coli: Bacteria behavior is being analyzed in computational simulations as part of a Simulating Microbial Systems (SMS) program. Run by the US Defense Advanced Research Projects Agency, the “SMS seeks interdisciplinary, comprehensive, and integrated workflows to generate unknown parameters from new data to inform computational models that can predict E. coli.”
Full body data: Precisely personalized care is the goal of European Virtual Human Twins Initiative, a project from the European Commission. The group creates digital twins and updates them with an individual’s personal conditions and health information that shifts as they age, keeping prevention as a focal point.
Respiratory viral pathogens: The complexities and variety of causes behind respiratory infections makes it an ideal area for digital twins. Its use in hospital ICUs can help doctors consider pneumonia treatment outlooks and develop plans for spread of infection.
Pharmaceuticals: Many pharma companies are opting to use digital twins since drug development is highly expensive and animal testing does not always provide clear data compared to human testing. Examples include Orion Pharma, which paired with AstraZeneca and Bayer to create digital twins that “capture genetic and molecular interactions that causally drive clinical and physiological outcomes.” Immunology company, Sanofi, also is using digital twins as “an essential first step to improve efficacy and safety.”
Future of Digital Twins in Healthcare
While digital twin development within healthcare is still in early stages, it promises to pioneer much change.
“When you have this model, you can personalize with certain features, certain anatomy, then you can try things. In heart surgery, you can’t try 20 different things, you only have one shot,” Ellen Kuhl PhD, professor of engineering and bioengineering at Stanford University, told Computer Weekly.
As technology advances and personalized healthcare continues to trend, it is likely digital twins will have a long-term place in medical practices. Astute clinical laboratory professionals will watch the expansion of this trend, since lab data will play such a key role in its development.
Holmes says life in prison is ‘Hell’ and that Theranos was a failure but ‘not fraud’
For some reason disgraced Theranos founder and ex-CEO Elizabeth Holmes, in a lengthy interview with People magazine, described life in prison while raising her two children even as a three-judge panel of the US 9th Circuit Court of Appeals affirmed her conviction and 11.25-year sentence for fraud.
In June of 2024, Holmes’ defense team appealed to have her conviction overturned due to alleged errors in her trial. According to court documents containing the federal judges’ decisions, her attorneys argued that:
Former Theranos employees who testified as lay witnesses should not have been allowed to offer improper expert testimony.
The court abused its discretion by allowing testimony that Theranos voided all patient sample tests run on a device used in Theranos’s clinical laboratory.
Her rights were violated under the Confrontation Clause of the Sixth Amendment when she was prohibited from cross-examining a former Theranos laboratory director on aspects of his post-Theranos employment.
In February 2025, the judges rejected all points and denied her appeal. Holmes is serving her sentence in a minimum security federal prison camp in Texas and is currently scheduled to be released in 2032.
Elizabeth Holmes (above) taken backstage at TechCrunch Disrupt San Francisco 2014 when Holmes was at the height of her fame and popularity. At this point, Theranos’ Edison blood testing device had not yet been shown to be a fake. But as clinical laboratory scientists and anatomic pathologists studied the technology it was shown to be incapable of producing the results claimed by Holmes and her company president Ramesh Balwani. Today, both are serving lengthy prison sentences for defrauding investors. (Photo copyright: Max Morse/Wikimedia Commons.)
‘Nothing More than a Mirage’
Holmes was convicted in 2022 and sentenced to 135 months for her role in the Theranos fraud case. She was also ordered to pay approximately $452 million in restitution due to her offense, which resulted in significant financial losses to various entities and individuals.
Holmes’ one-time romantic partner and former president of Theranos Ramesh “Sunny” Balwani also was convicted of several fraud charges and sentenced to 155 months in prison.
Theranos claimed to have invented a device called Edison that could run a variety of fast, accurate, and affordable clinical laboratory diagnostic tests from a single finger prick of blood. That’s in contrast to traditional testing methods that require veinous blood drawn with a hypodermic needle. The reality, however, was that the Edison device did not work as described to investors.
“The vision sold by Holmes and Balwani was nothing more than mirage,” wrote 9th Circuit Judge Jacqueline Nguyen, JD, in the panel’s decision, adding that the “grandiose achievements touted by Holmes and Balwani were half-truths and outright lies.”
The judges continued: “Theranos’s blood-testing device failed to deliver faster and more accurate testing results than conventional technology. Pharmaceutical companies never validated the technology, as Holmes and Balwani had told investors. Contrary to the rosy revenue projections shared with investors and business partners, Theranos was running out of money.”
Life Behind Bars
Holmes told People she has adjusted to prison life, waking up every morning just after 5 AM. Her routine includes daily exercise and working as a reentry clerk. Holmes, who was once touted as having an estimated worth of $4.5 billion, now earns just 31 cents an hour teaching fellow inmates how to prepare resumes and apply for jobs and government benefits.
“So many of these women don’t have anyone, and once they’re in there, they’re forgotten,” she told People.
Holmes also teaches French and participates in cognitive and behavioral therapy for post-traumatic stress disorder (PTSD) to address past traumas, including the downfall of Theranos, which was once valued at $9 billion.
“It’s surreal,” she said. “People who have never met me believe so strongly about me. They don’t understand who I am. It forces you to spend a lot of time questioning belief and hoping the truth will prevail. I am walking by faith and, ultimately, the truth. But it’s been hell and torture to be here.”
Raising Children from Prison
Holmes’ trial was delayed three times due to the COVID-19 pandemic and then a fourth time due to a pregnancy. She gave birth to son William a few weeks before her trial began. She later gave birth to daughter Invicta. Both children are being raised by their father Billy Evans, Holmes’ current partner.
Critics allege Holmes only had children to gain sympathy and attempt to avoid prison time. In the People interview, she tried to dispel those claims.
“I know how the optics look, but I always wanted to be a mother,” she said. “I wanted to have children, be a mom. I truly did not think I would ever be convicted or found guilty. I kept talking to my lawyers and they also assured me we would never get this far.
“It wasn’t planned, and I can’t worry about what others think,” she added. “It’s just when the timing happened.”
Holmes’ children will be nine and 10 years-old when she’s slated for release in 2032. She continues to maintain her innocence and considers her trial and conviction a miscarriage of justice. She asserts that while Theranos was a flop, “failure is not fraud.”
“First it was about accepting it happened. Then it was about forgiving myself for my own part. [And] I refused to plead guilty to crimes I did not commit,” Holmes said.
Interestingly, Holmes intends to return to the healthcare industry upon her release. “There is not a day I have not continued to work on my research and inventions,” she told People. “I remain completely committed to my dream of making affordable healthcare solutions available to everyone.”
How she plans to do that given the federal government has banned her for life from operating a clinical laboratory and participating in federal health programs is anyone’s guess.
And thus the life and times saga of Elizabeth Holmes continues.
Innovative in-office test, when integrated with UTI microbiology testing performed by clinical laboratories, could contribute to better patient outcomes
Treatments for certain bacterial infections are becoming less effective due to antimicrobial resistance (AMR). Now, after a 10-year-long worldwide competition, the first multi-million euro prize for an accurate, rapid, and cost effective clinical laboratory test for diagnosing and treating urinary tract infections (UTIs) went to Sysmex Corporation’s subsidiary Astrego. This milestone event could benefit tens of millions of people who suffer from UTIs annually.
Astrego, of Uppsala, Sweden, won the €8 million (US$8.19 million) Longitude Prize on AMR for its PA-100 AST System. The new diagnostic technology will “transform treatment of urinary tract infections and brings the power of clinical laboratory testing into a doctor’s office,” according to a news release from Challenges Works, the United Kingdom-based organization that organized and awarded the prize.
The Astrego system is, according to Challenge Works’ website, a “game-changing solution” in “a novel point-of-care diagnostic test that rapidly and accurately identifies the presence of a bacterial infection and the right antibiotic to prescribe.”
“We launched the Longitude Prize on AMR (in 2014) to create the urgent ‘pull’ needed to get innovators working on one of the biggest life-and-death challenges facing humanity. Hundreds of teams [that] competed with multiple solutions [are] now close to market thanks to the prize,” said Tris Dyson, Managing Director, Challenge Works, in a news release.
The new diagnostic technology “could herald a ‘sea change’ in antibiotic use” according to the judges of the competition, The Guardian reported.
“The PA-100 AST System (above) creates a future where patients can quickly and accurately get a diagnosis and the correct treatment when they visit the doctor,” said Sherry Taylor, MD, UK National Health Service, Temple Fortune Medical Group, London, in the Challenge Works news release. “Accurate, rapid diagnosis of bacterial infections that help doctors and health workers to manage and target antibiotics, will slow the development and spread of antibiotic resistant infections, improve healthcare and save potentially millions of lives,” she added. In-office point-of-care systems like the PA-100 may reduce the number of doctor orders for UTI tests to clinical laboratories while contributing to better patient outcomes. (Photo copyright: Sysmex.)
How the Test Works
In the UK, people are treated for UTIs more than any other infection. It takes about three days for doctors to receive the results from traditional microbiology testing. They then prescribe an antibiotic to treat the infection. But about half of “infection-causing bacteria are resistant to at least one antibiotic,” according to a news release from the Geneva, Switzerland-based NESTA Foundation which funded the Longitude Prize on AMR.
“It’s impossible to overstate how critical it is to address AMR [antimicrobial resistance]. By 2050, it is predicted to cause 10 million deaths a year—matching those caused by cancer—and cost $1 trillion in additional health costs,” the news release states.
UTI are more common in women and the reason for eight million healthcare appointments annually in the US, according to Medscape.
The PA-100 AST system makes it possible for patients to provide a small urine sample during their appointments with doctors, find out if they have a bacterial infection in 15 minutes, and receive the “right antibiotic to treat it within 45 minutes,” NESTA said. Sysmex describes the PA-100 AST as an “automated phenotypic analyzer, based on EUCAST standards,” that combines “phase-contrast microscopy and nanofluidics to make available antibiograms at point of care.” It enables healthcare providers to perform antimicrobial susceptibility testing (AST) in-office rather than sending out urine samples to microbiology laboratories.
The systems works as follows, according to the Sysmex website:
As a urine sample passes through the chip, “single bacterial cells are trapped in individual channels.”
Meanwhile, “larger cellular components” are filtered and kept out of the nanofluidic chip.
Contrast-phase microscopy enables real-time monitoring of cell growth. “Resistant bacteria keep a higher growth rate during incubation, while susceptible ones grow slowly or lyse.”
Expert computer software identifies that bacterial strain, delivers an “easy to interpret antibiogram after assay completion” and provides an “informed prescription decision” on which antibiotic is expected to fight the infection.
“The PA-100 AST System challenges bacteria present in a patient’s urine with microscopic quantities of antibiotics in tiny channels embedded in a cartridge the size of a smartphone,” said Mikael Olsson, CEO and co-founder of Sysmex Astrego, in The Microbiologist.
“We rapidly pinpoint whether a bacterial infection is present and identify which antibiotic will actually kill the bugs, guiding doctors only to prescribe antibiotics that will be effective,” he added.
Sysmex is conducting more studies in the UK and working with regulators in Europe for clearances, according to Olsson.
Older Antibiotics May Make Comeback
It’s possible that use of the PA-100 system to identify the best antibiotic to treat infections could lead to a resurgence in the use of previously retired antibiotics.
“Roughly 25-30% of patients have infections resistant to older first-line antibiotics which have been retired as a result; this means the remaining 70-75% of patients could still benefit from those older drugs,” Pathology in Practice reported, adding, “Since the PA-100 AST System identifies which specific antibiotic can treat an infection, it will likely allow retired antibiotics to be brought back into service because the test is able to demonstrate when an infection is susceptible to their effects.”
Many people could benefit from the older antibiotics, Challenge Works noted.
Revolutionizing Healthcare
The Sysmex Astrego’s PA-100 AST System is a significant development.
“Currently, I send the urine sample off for analysis, and it usually takes around three days to come back with results,” said Sherry Taylor, MD, UK National Health Service, Temple Fortune Medical Group, London, in the Challenge Works news release. “Having a bedside test that would enable rapid diagnosis through antibiotic susceptibility testing would revolutionize general practice and patient care. It’s all about using antibiotics only when necessary and appropriate.”
Each individual test costs about €25 (US$25.72), The Guardian reported, adding that ramped up production may lower the price.
The PA-100 AST System is the latest example of a diagnostic/therapeutic solution developed in Europe rather than the US, which is often slower to award regulatory clearance.
It also is another test that will be performed outside of traditional clinical laboratory settings, demonstrating the trend to move medical laboratory tests closer to patients.
New guidelines come on the heels of recommendations covering post-market modifications to AI products, including those incorporated into systems used by clinical laboratories
Artificial intelligence (AI) is booming in healthcare, and as the technology finds its way into more medical devices and clinical laboratory diagnostic test technologies the US Food and Drug Administration (FDA) has stepped up its efforts to provide regulatory guidance for developers of these products. This guidance will have an impact on the development of new lab test technology that uses AI going forward.
In December, the FDA issued finalized recommendations for submitting information about planned modifications to AI-enabled healthcare products. Then, in January, the federal agency issued draft guidance that covers product management and marketing submission more broadly. It is seeking public comments on the latter document through April 7.
“The FDA has authorized more than 1,000 AI-enabled devices through established premarket pathways,” said Troy Tazbaz, director of the Digital Health Center of Excellence at the FDA’s Center for Devices and Radiological Health, in a press release announcing the draft guidance.
This guidance “would be the first to provide total product life cycle recommendations for AI-enabled devices, tying together all design, development, maintenance and documentation recommendations, if and when finalized,” Healthcare IT News reported.
“Today’s draft guidance brings together relevant information for developers, shares learnings from authorized AI-enabled devices, and provides a first point-of-reference for specific recommendations that apply to these devices, from the earliest stages of development through the device’s entire life cycle,” said Troy Tazbaz (above), director of the Digital Health Center of Excellence at the FDA Center for Devices and Radiological Health, in a press release. The new guidance will likely affect the development of new clinical laboratory diagnostic technologies that use AI. (Photo copyright: LinkedIn.)
Engaging with FDA
One key takeaway from the guidance is that manufacturers “should engage with the FDA early to ensure that the testing to support the marketing submission for an AI-enabled device reflects the agency’s total product lifecycle, risk-based approach,” states an analysis from consulting firm Orrick, Herrington and Sutcliffe LLP.
Another key point is transparency, Orrick noted. For example, manufacturers should be prepared to offer details about the inputs and outputs of their AI models and demonstrate “how AI helps achieve a device’s intended use.”
Manufacturers should also take steps to avoid bias in data collection for these models. For example, they should gather evidence to determine “whether a device benefits all relevant demographic groups similarly to help ensure that such devices are safe and effective for their intended use,” Orrick said.
New Framework for AI in Drug Development
On the same day that FDA announced the device guidelines, the agency also proposed a framework for regulating use of AI models in developing drugs and biologics.
“AI can be used in various ways to produce data or information regarding the safety, effectiveness, or quality of a drug or biological product,” the federal agency stated in a press release. “For example, AI approaches can be used to predict patient outcomes, improve understanding of predictors of disease progression and process, and analyze large datasets.”
The press release noted that this is the first time the agency has proposed guidance on use of AI in drug development.
These include “bias and reliability problems due to variability in the quality, size, and representativeness of training datasets; the black-box nature of AI models in their development and decision-making; the difficulty of ascertaining the accuracy of a model’s output; and the dangers of data drift and a model’s performance changing over time or across environments. Any of these factors, in FDA’s thinking, could negatively impact the reliability and relevancy of the data sponsors provide FDA.”
The FDA also plans to participate in direct testing of AI-enabled healthcare tools. In October, the FDA and the Department of Veterans Affairs (VA) announced that they will launch “a joint health AI lab to evaluate promising emerging technologies,” according to Nextgov/FCW.
Elnahal said the facility will allow federal agencies and private entities “to test applications of AI in a virtual lab environment.” The goal is to ensure that the tools are safe and effective while adhering to “trustworthy AI principles,” he said.
“It’s essentially a place where you get rapid but effective evaluation—from FDA’s standpoint and from VA’s standpoint—on a potential new application of generative AI to, number one, make sure it works,” he told Nextgov/FCW.
He added that the lab will be set up with safeguards to ensure that the technologies can be tested safely.
“As long as they go through the right security protocols, we’d essentially be inviting parties to test their technology with a fenced off set of VA data that doesn’t have any risk of contagion into our actual live systems, but it’s still informative and simulated,” he told Nextgov/FCW.
There has been an explosion in the use of AI, machine learning, deep learning, and natural language processing in clinical laboratory diagnostic technologies. This is equally true of anatomic pathology, where AI-powered image analysis solutions are coming to market. That two federal agencies are motivated to establish guidelines on working relationships for evaluating the development and use of AI in healthcare settings tells you where the industry is headed.
Small handheld device uses sound waves to detect certain clinical laboratory biomarkers in blood samples
University of Colorado Boulder researchers have developed a novel technology that uses sound waves to test for biomarkers in blood samples. In addition to being very easy to use, the handheld device is portable, highly sensitive, and delivers results in minutes. Though not ready for clinical use, this is yet another example of how researchers are developing faster diagnostic tests that can be performed in near-patient settings, and which do not have to be done in core laboratories, shortening time to answer.
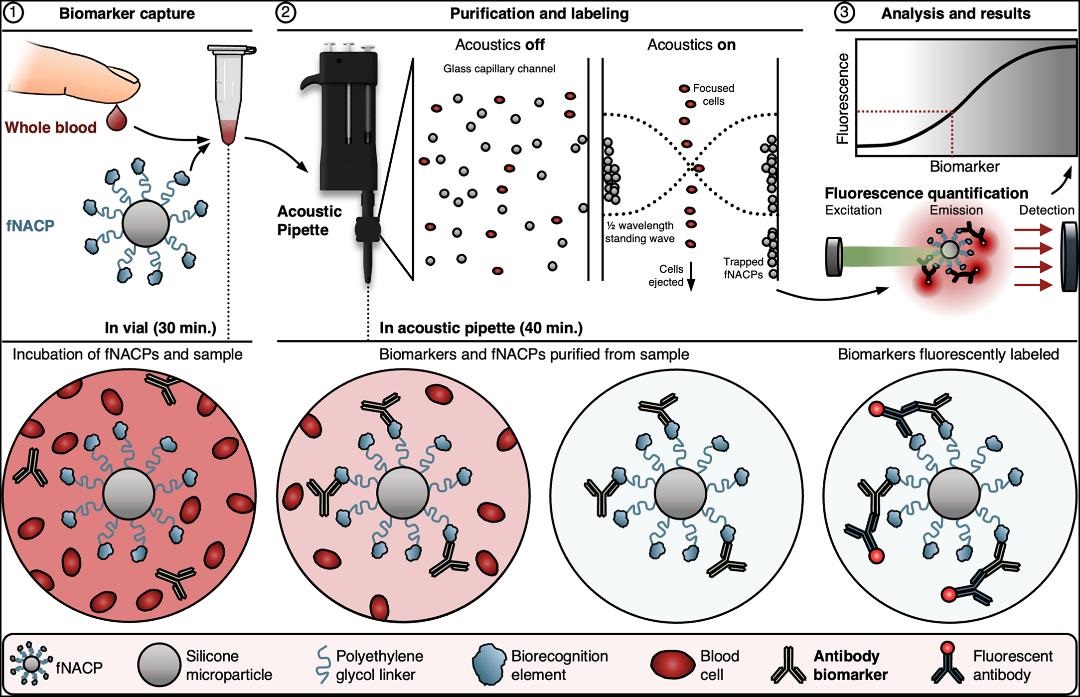
The small instrument—referred to as an “acoustic pipette”—delivers sound waves to tiny particles within the device called “functional negative acoustic contrast particles” (fNACPs). These particles are cell-sized balls that can be customized with different coatings to identify specific biomarkers—such as viruses or proteins—in tiny blood samples, according to a news release.
To operate the device, the custom fNACPs are mixed with a drop of blood and then placed inside the acoustic pipette. The mixture is then blasted with sound waves, which forces particles carrying certain biomarkers to one side of the chamber where they are trapped while the rest of the blood is expelled. The captured biomarkers are then labeled with fluorescent tags and examined with lasers to determine how much of a specific biomarker is present.
“We’re basically using sound waves to manipulate particles to rapidly isolate them from a really small volume of fluid,” said Cooper Thome (above), PhD candidate in Chemical and Biological Engineering at UC Boulder and first author of the study in a news release. “It’s a whole new way of measuring blood biomarkers,” he added. Should further studies validate this approach, clinical laboratories may be able to use this technology to perform diagnostic tests with smaller volumes of patient samples. (Photo copyright: University of Colorado Boulder.)
Blood Testing Quickly and in Multiple Settings
To test their invention, the UC Boulder researchers examined antibodies against a protein called ovalbumin, which is found in egg whites and often used in the development of various vaccines. The scientists discovered that their device could detect the antibodies even in low amounts.
Current rapid tests known as lateral-flow assays can detect specific biomarkers in blood or urine samples but cannot determine how much of the biomarker is present. Enzyme-linked immunotherapy assays (ELISA), the leading clinical laboratory blood test, requires expensive equipment and can take hours to days for results to be received.
With UC Boulder’s new handheld device, tiny blood samples collected from a single finger prick could ensure accurate test results are available quickly at the point of care as well as outside of traditional healthcare settings. This would greatly benefit people in developing nations and underserved communities and may help ease test anxiety for individuals who are apprehensive about traditional blood tests.
“We’ve developed a technology that is very user friendly, can be deployed in various settings, and provides valuable diagnostic information in a short time frame,” said Wyatt Shields IV, PhD, Assistant Professor, Department of Chemical and Biological Engineering, UC Boulder, and senior author of the research in the news release.
“In our paper, we demonstrate that this pipette and particle system can offer the same sensitivity and specificity as a gold-standard clinical test can but within an instrument which radically simplifies workflows,” he added. “It gives us the potential to perform blood diagnostics right at the patient’s bedside.”
The graphic above, taken from UC Boulder’s published paper, illustrates how “fNACPs capture target biomarkers from whole blood samples. fNACPs are purified from blood components by acoustic trapping and captured biomarkers are labeled with a fluorescent antibody within the acoustic pipette. fNACP fluorescence is then measured to determine biomarker presence and concentration.” (Graphic/caption copyright: University of Colorado Boulder.)
Not Like Theranos
The authors of the UC Boulder study are cognizant of some skepticism surrounding the field of biosensing, especially after the downfall of Theranos. The scientists insist their technology is different and based on systematic experiments and peer-reviewed research.
“While what they (Theranos) claimed to do isn’t possible right now, a lot of researchers are hoping something similar will be possible one day,” said Thome in the news release. “This work could be a step toward that goal—but one that is backed by science that anybody can access.”
The device is still in its initial proof-of-concept stage, but the UC Boulder scientists have applied for patents for the apparatus and are searching for ways to scale its use and expand its capabilities.
“We think this has a lot of potential to address some of the longstanding challenges that have come from having to take a blood sample from a patient, haul it off to a lab, and wait to get results back,” Shields noted.
More research, studies, and regulatory reviews will be needed before this technology becomes available for regular, widespread use. But UC Boulder’s new blood testing device is another example of a research team using novel technology to test for known biomarkers in ways that could improve standard clinical laboratory testing.