From some adverse events, clinical laboratory tests may be integrally tied to delays in treatment and faulty care management events that cause patient harm and deaths
Adverse patient safety events are increasing according to The Joint Commission (TJC), a nonprofit US-based organization that accredits tens of thousands of US healthcare organizations and programs. Its 2023 annual report on “sentinel events”—patient safety breaches that can inflict serious harm or death—found that these events jumped by 78.1% from 2020 to 2021 and by 19.3% from 2021 to 2022. These are significant increases. What effect do they have on healthcare providers?
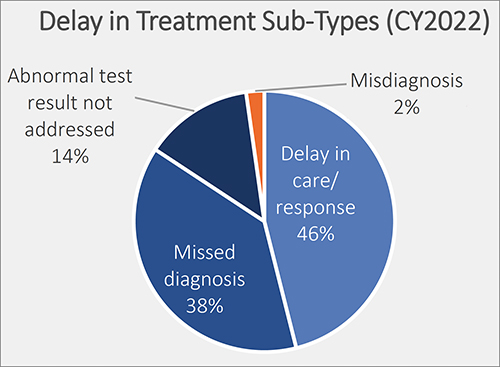
Of particular interest for clinical laboratory managers and pathologists is one finding by TJC involving “delay in treatment” as an adverse event. TJC determined that the cause of 38% of these episodes was due to “missed diagnoses.” It is likely that clinical laboratory test results have some role in this type of adverse event. Thus, this is a potential opportunity for medical lab leaders to add value by helping hospital administrators and physicians reduce the number adverse events tied to missed diagnoses.
Another consequence for hospitals and providers is lost revenue. Medicare will not reimburse care to providers when a medical error, fall, surgery on wrong site, or other “never event” happens, including misdiagnoses due to inaccurate clinical laboratory testing.
Thus, since patient safety is a priority and providers are tasked with reducing medical errors, The Joint Commission’s Office of Quality and Patient Safety has developed the Sentinel Event Database for tracking adverse patient safety events.
The de-identified and aggregate patient data includes “causes and outcomes of sentinel events, is analyzed yearly to help the nation in general—and accredited organizations in specific—gain insight into causes of sentinel events and develop mitigating strategies to prevent harm to individuals under their care,” according to The Joint Commission’s report, “Sentinel Event Data 2022 Annual Review.”
This graphic taken from The Joint Commission’s annual 2023 report on sentinel events shows the percentage of delays in treatment broken out by type. Delays in treatment is the second most common sentinel event, exceeding wrong surgery and medication management, according to The Joint Commission’s report. Only falls exceed delays in treatment, and since 80% of a patient’s health records are clinical laboratory test results, they could play a role in each of these adverse patient safety events. (Graphic copyright: The Joint Commission.)
Most Common Sentinel Events
According to The Joint Commission’s report, “Of reviewed sentinel events in 2022:
“20% resulted in patient death,
“6% in permanent harm or loss of function,
“44% in severe temporary harm, and
“13% in unexpected additional care/extended stay.
“Sentinel events resulting in death were most commonly associated with:
“patient suicide (24%),
“delays in treatment (21%), and
“patient falls (11%).
“Events resulting in severe temporary harm were most commonly associated with patient falls (62%).”
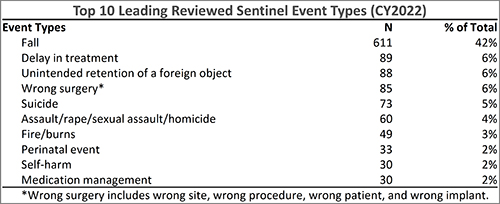
The Joint Commission’s annual 2023 report on sentinel events shows the top 10 sentinel event types in 2022. According to the report, delay in treatment, which could be caused by inaccurate clinical laboratory tests, moved from fourth place in 2018, to third place in 2021, and is now in second place. (Graphic copyright: The Joint Commission.)
National Quality Forum ‘Never Events’
In 2001, Ken Kizer, MD, founding President and CEO of the National Quality Forum (NQF), coined the phrase “never events” to describe often fatal and usually preventable medical errors. Since then, the list of never events, according to PSNet, a national web-based resource of the Agency for Healthcare Research and Quality (AHRQ), has grown to include 29 “serious reportable events” in seven categories:
Surgical or procedural events
Product or device events
Patient protection events
Care management events
Environmental events
Radiologic events
Criminal events
Listed under “Care management events” is “Patient death or serious injury resulting from failure to follow up or communicate laboratory, pathology, or radiology test results.”
In “Hospitals Take Steps to Drive Down Medical Errors in Their Emergency Departments,” Dark Daily wrote how one common source of errors in emergency rooms is lack of information that includes timely access to radiology or clinical laboratory test reports. Moreover, formal process improvement projects to identify and eliminate the sources of errors in emergency rooms can involve the hospital laboratory.
As medical laboratory managers know all too well, the fast-paced environment of a busy emergency room often contributes to errors such as hemolyzed specimens, a delay in transporting the specimen from the ER to the lab, or incomplete patient information on the laboratory test request form as it is received in the hospital laboratory.
‘Stuff of Nightmares‘
In an article he penned for Chicago-based thought leadership and advisory company 4Sight Health, longtime healthcare writer David Burda commented on The Joint Commission’s sentinel events report. He wrote: “Two things scared me from this eight-page report. First, The Joint Commission is publishing statistics and trends in reported sentinel events. How many go unreported? Second, surgeons still are performing the right procedure on the wrong patient or the wrong procedure on the right patient? Isn’t there a checklist to prevent this? The stuff of nightmares.”
Burda went on to note that “88% of the sentinel events in 2022 happened at accredited hospitals, and 90% were self-reported by accredited organizations. Patients, patients’ families, or current/former employees reported 10% of the sentinel events to The Joint Commission.”
The rapid rise of patient adverse safety events should be a concern for all sectors of the healthcare industry. Clinical laboratory managers should be especially concerned since nearly every medical decision precedes or follows a medical laboratory test.
Of 27 BSL-4 labs assessed, Global Biolabs ranked only seven as having ‘good’ biosafety management
In a new report, a research firm assessed the conditions at the handful of laboratories across the world that handle the most dangerous pathogens. In the wake of the SARS-CoV-2 global pandemic, there is heightened awareness of the risks of a lab accident that might release such pathogens into the environment, putting humans at risk.
Medical laboratory scientists working in clinical laboratories worldwide understand the critical nature of biosafety laboratory (BSL) criteria. Nearly all clinical laboratories that test for infectious disease agents are biosafety level-1 and -2 (BSL-1, BSL-2).
Other high-containment laboratories (HCL) that handle deadly, highly transmissible pathogens are typically government-run or university-affiliated. HCL labs have BSL-3 and BSL-4 levels and require rigorous adherence to protocols that ensure worker safety and prevent escape of dangerous pathogens.
Thus, the new report from Global Biolabs, which is critical of biorisk management protocols at existing and planned BSL-4 laboratories—especially given the increasing construction of new HCL labs worldwide—will be of interest to medical technologists, pathologists, and clinical scientists working with highly infectious diseases.
The biosafety experts who make up the Global Biolabs research team conduct risk-assessments and “provide key policy recommendations for strengthening biorisk management in BSL-4 labs,” according to the organization’s website.
“The more labs and people working with dangerous pathogens, the risks go up,” biosecurity expert Filippa Lentzos, PhD (above), Associate Professor, Science and International Security, King’s College London, told Science magazine. Lentzos was part of the team that created the Global Biolabs mapping project two years ago. Clinical laboratory managers may want to review the findings in the Global Biolabs report. (Photo copyright: King’s College London.)
Only Seven Out of 27 Countries Get ‘Good’ Overall Score
“The boom in BSL-4 lab construction appears, so far, not to have been accompanied by strengthened biorisk management oversight,” according to the Global Biolabs 2023 report from the Global Biolabs Initiative. “Additionally, most planned BSL-4 labs will be in countries with relatively low scores for governance and stability,” the report’s authors wrote.
The report included a ranking of countries by total biorisk management score, the Daily Mail noted, adding:
Of 27 countries analyzed, seven ranked as good (above 70%) for biorisk policies,
15 scored medium (above 30%),
five scored below.
Those with the best biorisk management scores (maximum 48):
Canada scored 46 (96%),
US scored 42 (88%),
Australia and the United Kingdom each scored 40 (83%).
Notably, China “scored zero on modifying pathogen rules.” According to the Daily Mail, “China’s overall management score (33) was in the middle of the pack, 69%.”
Associate Professor in Science and International Security, King’s College London, and Gregory Koblentz, PhD, Associate Professor and Director Biodefense Graduate Program, George Mason University, Fairfax, Virginia. The organization tracks maximum containment labs worldwide, noting trends that raise biosafety and biosecurity concerns.
According to the Daily Mail, Lentzos noted “that a particular worrying aspect of the BSL-4 boom was those countries looking to open their first lab were the bottom scorers in terms of good biorisk management.
“Many of the countries building new labs, some for the first time, score poorly on biorisk management. However, there is still time to strengthen national laws and regulations on biosafety, biosecurity, and dual-use research [biological research that could cause harm] to bring them up to international standards,” the Global Biolabs researchers wrote in their report.
Global Mapping of BSL-4 Labs
There are 51 BSL-4 labs operating worldwide, and 18 are planned or under construction, according to Global BioLab’s report. Here’s where they are located:
Europe: 24
North America: 12
Asia: 9
Oceania: 4
Africa: 2
South America: 0
Also, BSL-3+ labs total 55:
Europe: 21
North America: 18
Asia: 10
South America: 3
Africa: 2
Oceania: 1
The report also noted:
Of the 18 BSL-4 labs under construction, 11 are planned to open in Asia.
About half of BSL-4 labs are “less than the size of a tennis court.”
“Eighty percent (of BSL-4 labs) are located in urban areas, which heightens concerns about accidents at these facilities,” Koblentz told the Daily Mail.
According to Science, the number of BSL-4 labs has doubled since 2013. Growth in BLS-4 labs began around the time of the 2001 anthrax attacks and picked up speed in 2003 following the SARS outbreak, University World News reported.
Biosecurity and Biosafety Analyzed
Global Biolabs’ analysis included countries’ biosecurity and biosafety scores. Just 12 out of 27 countries with BSL-4 labs scored high on biosecurity, nine scored medium, and six scored low.
A high score for biosecurity—which US and France received—reflects laws for biosecurity, a national list of dangerous pathogens, and whistleblower protection.
Out of 27 countries, 21 with BSL-4 labs scored high on biosafety. However, two countries scored medium, and four scored low. The two countries that earned the highest scores for biosafety—Canada and Australia—have physical/engineering controls, occupational health, and transportation safety, among other areas reviewed.
Opportunities for Improvement
Global Biolabs made the following recommendations in their report:
Nations with BSL-4 and BSL-3 labs need to have in place biorisk management systems including comprehensive laws, regulations, and institutions that require safety and security risk assessments of proposed research.
Strengthening of biorisk management is called for by the World Health Organization and Biological Weapons Convention.
Labs, of all biosafety levels, are advised to aim toward safety, security, and responsible research.
The effort by Global BioLabs to create a public record of how each BSL-4 and BSL-3 laboratory adheres to strict standards of safety and operations demonstrates that some degree of risk exists in the operation of these labs. Whether government and world health authorities make it a priority to address known deficiencies in those labs is a question yet to be answered.
Federal prosecutors build the new healthcare-related fraud cases on previous nationwide enforcement actions from 2022
Federal charges have once again been brought against a number of physicians and clinical laboratory owners in what the US Department of Justice described as the “largest ever” coordinated nationwide law enforcement effort against COVID-19 pandemic-related healthcare fraud.
In total, the DOJ filed criminal charges against 18 defendants in five states plus the territory of Puerto Rico, according to an April 20 press release.
The highest dollar amount of these frauds involved ENT physician Anthony Hao Dinh, DO, who allegedly defrauded the Health Resources and Services Administration (HRSA) COVID-19 Uninsured Program for millions of dollars, and Lourdes Navarro, owner of Matias Clinical Laboratory, for allegedly “submitting over $358 million in false and fraudulent claims to Medicare, HRSA, and a private insurance company for laboratory testing” while performing “COVID-19 screening testing for nursing homes and other facilities with vulnerable elderly populations, as well as primary and secondary schools,” the press release states. Both court cases are being conducted in Southern California courtrooms.
The DOJ’s filing of charges came rather speedily, compared to other cases involving fraudulent clinical laboratory testing schemes pre-pandemic. The amount of money each defendant managed to generate in reimbursement from the fraud represents tens of thousands of patients. If feds were paying $100 per COVID-19 test, then the $153 million represents 153,000 patients, in just 18 to 24 months.
“Today’s announcement marks the largest-ever coordinated law enforcement action in the United States targeting healthcare fraud schemes that exploit the COVID-19 pandemic,” said Assistant Attorney General Kenneth A. Polite, Jr. (above), in an April 20 DOJ press release. “The Criminal Division’s Health Care Fraud Unit and our partners are committed to rooting out pandemic-related fraud and holding accountable anyone seeking to profit from a public health emergency.” Clinical laboratory managers may want to pay close attention to the DOJ’s prosecution of these newest cases of alleged COVID-19 fraud. (Photo copyright: Department of Justice.)
Prosecutors allege that Navarro and her husband, Imran Shams, who operated Matias—also known as Health Care Providers Laboratory—perpetrated a scheme to perform medically unnecessary respiratory pathogen panel (RPP) tests on specimens collected for COVID-19 testing, even though physicians had not ordered the RPP tests and the specimens were collected from asymptomatic individuals.
In some cases, the indictment alleges, Navarro and Shams paid kickbacks and bribes to obtain the samples.
The indictment notes that reimbursement for RPP and other respiratory pathogen tests is generally “several times higher” than reimbursement for COVID-19 testing. Claims for the tests were submitted to Medicare and an unidentified private insurer, as well as the HRSA COVID-19 Uninsured Program, which provided support for COVID-19 testing and treatment for uninsured patients.
Claims to the HRSA falsely represented that “the tested individuals had been diagnosed with COVID-19, when in truth and in fact, the individuals had not been diagnosed with COVID-19 and the tests were for screening purposes only,” the First Superseding Indictment states.
The indictment further states that both Navarro and Shams had previously been barred from participating in Medicare and other federal healthcare programs due to past fraud convictions. Navarro, the indictment alleges, was reinstated in December 2018 after submitting a “false and fraudulent” application to the HHS Office of Inspector General.
It also alleges that Navarro and Shams concealed their ownership role in Matias so the lab could maintain billing privileges.
More Alleged Abuse of HRSA Uninsured Program
In a separate case, Federal prosecutors alleged that Anthony Hao Dinh, DO, an ear, nose, and throat physician in Orange County, California, engaged in a scheme to defraud the HRSA COVID-19 Uninsured Program as well.
Dinh, prosecutors allege, “submitted fraudulent claims for treatment of patients who were insured, billed for services that were not rendered, and billed for services that were not medically necessary.”
The criminal complaint, filed on April 10, alleges that Dinh submitted claims for approximately $230 million, enough to make him the program’s second-highest biller. He was paid more than $153 million, prosecutors allege, and “used fraud proceeds for high-risk options trading, losing over $100 million from November 2020 through February 2022,” states the US Attorney’s Office, Central District of California press release.
Dinh was also charged for allegedly attempting to defraud the federal Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program. He faces a maximum sentence of 50 years in federal prison, the press release states.
Dinh’s sister, Hang Trinh Dinh, 64, of Lake Forest, California, and Matthew Hoang Ho, 65, of Melbourne, Florida, are also charged in the complaint, the Los Angeles Times reported.
Both of these cases are notable because of the size of the fraud each defendant pulled off involving COVID-19 lab testing. Clinical laboratory managers may want to review the original court indictments. The documents show the brazenness of these fraudsters and detail how they may have induced other doctors to refer them testing specimens.
More than 10,000 doctors walked out for the second time in two months, further burdening an already overwhelmed NHS
On April 11, tens of thousands of junior doctors (similar to medical residents in the US) left their posts in British hospitals commencing a four-day walkout. The strike resulted in the cancellation of thousands of operations and appointments, as well as cancelling or delaying thousands of clinical laboratory tests and anatomic pathology readings associated with those healthcare visits and surgical procedures.
The walkout was spurred by pay concerns and working conditions and comes on the heels of a three-day strike last month. That strike had already weakened the UK’s frail National Health System (NHS), which has become inundated with appointment backlogs that predate the COVID-19 pandemic, and which has led to longer wait times to see a doctor, ABC News reported.
This latest strike was more perilous since the senior doctors who covered for their juniors during last month’s strike were previously on leave for a holiday weekend, United Press International (UPI) reported.
“These strikes are going to have a catastrophic impact on the capacity of the NHS to recover,” Matthew Taylor (above), Chief Executive of the NHS Confederation, told Sky News. “The health service has to meet high levels of demand at the same time as making inroads into that huge backlog … That’s a tough thing to do at the best of times—it’s impossible to do when strikes are continuing.” (Photo copyright: Wikimedia Commons.)
Junior Docs Cite Injustice
Junior doctors who walked out are calling for a 35% pay raise to right the wrongs of 15 years of below-inflation raises, but the government continues to argue it cannot afford to increase pay, UPI noted.
“There is nothing ‘junior’ about the work I have done as a doctor. For an hour of work that I might save a life, I can be paid 19£ [$23.65],” said Jennifer Barclay, MD, a surgical junior doctor in the UK’s North West electoral zone, in a British Medical Association (BMA) press release.
“My dad, an electrician, tells me to quit and retrain in his footsteps. I’d be earning more, have less stress, less responsibility, better hours, and a better work-life balance after three years,” she added. “Surely, this life, this training, responsibility, debt, and crushing workload is worth more than 19£ per hour? I’ll be on the picket line this week because doctors believe that it is.”
According to the BMA, newly qualified junior doctors earn just over 14£ ($17.43) per hour, ABC News reported, which added, “The doctors’ union has asked for a 35% pay rise to bring junior doctor pay back to 2008 levels.”
However, their pay demands come in the midst of a cost-of-living crisis in the UK. Inflation has risen above 10%. Paired with increases in heating costs and food prices mean that decreased wages leave many struggling to pay bills, ABC news reports.
A hard-hitting BMA advertising campaign designed to shine light on these disparities depicts three junior doctors (with one-, seven-, and 10-years’ experience) removing an appendix. The video shows that the total the three would be paid for the hour-long operation would be 66.55£ ($82.84):
Doctor with one year experience: 14.09£ ($17.54).
Doctor with two years’ experience: 24.46£ ($30.45).
Doctor with three years’ experience: 28£ ($34.85).
And this for performing a potentially life-saving procedure, the BMA stated.
In the press release, BMA Junior Doctors Committee co-chairs Robert Laurenson and Vivek Trivedi said, “It is appalling that this government feels that paying three junior doctors as little as 66.55£ between them for work of this value is justified. This is highly skilled work requiring years of study and intensive training in a high-pressure environment where the job can be a matter of life or death.”
Patient Care is Affected
Lower salaries also affect patient care levels and have led to recruitment issues, with many doctors leaving the profession, the BBC reported. “This is not a situation where we are fixed in our position. We’re looking for negotiations and Steve Barclay (UK’s Secretary of State for Health and Social Care) isn’t even willing to talk to us. He hasn’t put any offer at all on the table … there has to be two sides in the discussion,” Emma Runswick, MD, a junior doctor and deputy chairwoman of the BMA, told the BBC.
But while the junior doctors battle for wages, the government’s initial focus has been on patient wellbeing. “There will be risks to patient safety, risks to patient dignity, as we are not able to provide the kind of care we want to,” NHS Confederation Chief Executive Matthew Taylor told UPI prior to the walkout.
The timing of the walkout also caused consternation with the NHS. “Not only will walkouts risk patient safety, but they have been timed to maximize disruption after the Easter break,” Health Secretary Barclay told UPI as the walkout was announced.
Barclay also claimed the amount sought by doctors was “unreasonable” and would cause raises above $25,000 per year, UPI reported. “If the BMA is willing to move significantly from this position and cancel strikes, we can resume confidential talks and find a way forward as we have done with other unions,” he stated.
It is important to note that doctors would be pulled from picket lines if immediate danger were present due to trade union laws that say life-and-limb coverage must be provided, the BMA told the BBC.
Founder of now defunct clinical laboratory testing company was supposed to report to prison April 27, but a last-minute legal challenge has delayed that judge’s order
Anatomic pathologists and clinical laboratory leaders who are following the continuing saga of Theranos and Elizabeth Holmes may be interested to learn that the former CEO’s attorneys are making last-minute legal moves to delay her prison sentence while she appeals her guilty verdict. At the same time, Holmes appears to be on a mission to revamp her public image.
Apparently, the twists and turns in Holmes’ never-ending story are not yet over when it comes to Theranos, its maligned clinical laboratory technology, and the company’s convicted founder.
On May 7, The New York Times (NYT) profiled Holmes in a massive, 5,000-word story that attempted to portray her as a flawed businessperson who now prefers a simpler life with her partner and two young children.
“I made so many mistakes and there was so much I didn’t know and understand, and I feel like when you do it wrong, it’s like you really internalize it in a deep way,” disgraced Theranos founder Elizabeth Holmes recently told The New York Times. Anatomic pathologists and clinical laboratory directors impacted by the revelation that Theranos hide the fact that its blood testing technology was faulty may not sympathize with Holmes’ position. (Photo copyright: Stuart Isett/Fortune Global Forum.)
Legal Team Secures Last-Minute Delay in Holmes’ Surrender
Holmes admitted to the news outlet that the deep voice she used in public, along with her black turtleneck sweaters, were part of a character she created.
“I believed it would be how I would be good at business and taken seriously and not taken as a little girl or a girl who didn’t have good technical ideas,” Holmes told the NYT. “Maybe people picked up on that not being authentic, since it wasn’t.”
However, on April 26, the 9th Circuit Court of Appeals stayed her surrender date until that court rules on Holmes’ latest bid to stay free while she appeals her conviction, The Washington Post reported.
Just days earlier on April 10, a district court judge ruled that Holmes would not stay free while her appeal progresses. The 9th Circuit announcement curtailed the district court ruling. It is not known when the 9th Circuit will issue a decision in the matter.
New York Times Reports on Holmes’ Change in Personality
The somewhat odd New York Times profile of Holmes varied between reflections on her past crimes and on her current personal life, where she is known as “Liz.”
“In case you’re wondering, Holmes speaks in a soft, slightly low, but totally unremarkable voice—no hint of the throaty contralto she used while running her blood-testing startup Theranos, now defunct,” the NYT reported.
Holmes still lives in California with her partner, Billy Evans (whose parents own a luxury hotel chain), and their two children: a son who is almost two years old and a daughter born in February. She works at home for a rape-crisis hotline.
Balwani’s Role in Theranos Again Publicly Debated
In the NYT interview, Holmes talked about being raped while a student at Stanford University and about alleged abuse from her Theranos business partner and former lover, Ramesh “Sunny” Balwani.
Balwani, Theranos’ former President and Chief Operating Officer, began his 12-year, 11-month prison sentence on April 20 in a Southern California facility for his role in defrauding Theranos investors, KTVU TV reported. Balwani has also appealed his conviction on the 12 fraud charges.
Holmes reiterated to the NYT past statements she made in court that Balwani allegedly exerted social and sexual control over her when they both worked at Theranos and were in a romantic relationship.
“She lived by entrepreneurial tenets that she said Balwani told her she needed to follow in order to succeed,” the NYT reported. “These included not sleeping for more than five hours, going vegan, getting to the office daily by 5 a.m., no alcohol.”
“[I] deferred to [Balwani] in the areas he oversaw because I believed he knew better than I did,” including on clinical lab activities at Theranos, Holmes said.
Balwani’s attorneys dismissed Holmes’ allegations, as they have in the past.
Clinical laboratory professionals can reasonably make two broad observations from the continuing saga of Theranos and Elizabeth Holmes:
Justice for healthcare crimes is often deferred for those who have influence and money.
Holmes’ image overhaul may be a last-ditch effort to sway public opinion about her, in the event that she receives a new jury trial as a result of her appeal.
Dark Daily will continue to keep you updated on further developments in this case.
Prior to that, however, the FDA had already announced its intention to issue a proposed rule giving the agency regulatory oversight of LDTs.
“The FDA has continually supported the passage of the VALID Act by Congress,” attorney Charles Dunham IV, a Shareholder at Greenberg Traurig LLP in Houston, told Dark Daily. “In fact, there is speculation that the VALID Act will be attached to the Pandemic and All Hazards Preparedness Act as it moves through Congress.”
“The FDA may not actually proceed with promulgating rules to regulate LDTs if it is concerned it will not be successful in court if the rules are challenged, which would happen,” said attorney Charles Dunham IV (above), a Shareholder at Greenberg Traurig, LLP. Clinical laboratory leaders can learn more from Dunham during a panel discussion at next week’s 2023 Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management in New Orleans. (Photo copyright: Greenberg Traurig LLP.)
Arguments For and Against FDA LDT Regulation of LDTs
Supporters of the VALID Act contend that putting LDTs under FDA regulation will lead to improved patient safety and less review for low-risk tests. Their argument is that LDTs should undergo the same FDA review and approval process as other medical devices.
Hospital laboratory managers and pathologists—particularly in academic medical center laboratories—have largely opposed FDA regulation of LDTs. They prefer to keep the current setup under which lab-developed tests are validated under the Clinical Laboratory Improvement Amendments of 1988 (CLIA). They argue that FDA intervention will slow down development of new tests.
In response, an FDA official indicated during the American Clinical Laboratory Association’s (ACLA) annual meeting on March 1 that the federal agency plans to issue a proposed rule to regulate LDTs, BioWorld reported. That rulemaking has not yet emerged. It’s possible the FDA will wait and see what happens in Congress with the VALID Act.
“Some legal experts have suggested that one significant new legal challenge FDA may face is the Supreme Court’s West Virginia v. EPA decision last summer that limited the ability of the EPA to cap power plant emissions by regulation due to the EPA’s lack of explicit congressional authority to do so,” said Gee, who also will appear on the Executive War College legal panel next week.
“The West Virginia v. EPA ruling provides support for those in the clinical lab industry who point to the FDA’s lack of clear statutory authority to regulate LDTs and therefore fundamentally disagree with FDA’s longstanding position that LDTs are medical devices subject to FDA’s authority to regulate,” he added.
Actions Clinical Laboratory Managers Can Take
Clinical laboratory managers who want to share their thoughts about the future of LDT regulation may want to take one or both of the following actions:
Contact their representatives in Congress.
Find out whether any trade associations they belong to have taken a position on the VALID Act.
Clinical laboratory professionals should monitor the VALID Act’s progress while also paying attention to industry groups and manufacturers that support or oppose the bill.
Doing so will provide a clearer indication of who has the most to gain or lose should the legislation be passed. Pathologists and medical laboratory managers should also remain alert for further efforts by the FDA to issue proposed rulemaking to regulate LDTs.