Media reporting on disparities in COVID-19 test billing sparks renewed calls for increased transparency in medical laboratory test charges
Recent media reports of massive disparities in the prices charged for COVID-19 lab tests throughout the United States have citizens and law makers alike again calling for increased transparency in clinical laboratory test charges.
One recent example involves the New York Times (NYT), which after learning that Austin-based Gibson Diagnostic Labs (GDL) of Irving, Tex., billed a patient $2,315 for one COVID-19 test, questioned the disparity in coronavirus testing charges. The article, titled, “Most Coronavirus Tests Cost About $100. Why Did One Cost $2,315?” brought unwanted attention to the Texas clinical laboratory.
On July 16, the NYT reported that GDL, “has run some of the most expensive coronavirus tests in America.” In addition, the paper reported that health insurance companies have paid GDL $2,315 for individual COVID-19 tests, but that in “a couple of cases,” the price rose to $6,946. However, that higher amount resulted “when the lab said it mistakenly charged patients three times the base rate.”
In response to the NYT report, GDL released a statement that said, “In April 2020, a commercial insurer doing business with Gibson Diagnostic Labs inquired about the company’s pricing practices regarding COVID-19 testing. In response to the inquiry, the company conducted an internal review and identified commercial claims that were billed incorrectly by the company’s third-party biller. Because this incident did not meet our standards of quality, service, and compliance, the company terminated its relationship with the third-party biller.”
Gibson Diagnostic Labs (above) in Irving, Texas, recently drew the attention of the New York Times after, according to GDL, its third-party biller accidentally used an incorrect CPT code causing one COVID-19 test customer to receive a bill for $2,315. Further, the NYT reported that “[GDL] billed 117 tests at that price and had 23 of the claims paid in full. Some insurers paid partial reimbursements or sent back no money at all.” In a statement, GDL said it has corrected the mistake and reimbursed all affected parties. (Photo copyright: Dylan Hollingsworth/The New York Times.)
GDL Blames Third-party Biller for Errors
Responding to questions from Dark Daily, GDL provided details that were not previously reported. In an email, GDL said it worked closely with a NYT reporter by providing information about the incident, but that the reporter left out key information.
GDL also said that after the NYT’s inquiry, the lab reviewed its billing systems and learned that the CPT code for 23 COVID-19 commercial claims were transposed as a result of human error, resulting in payments totaling $53,255. The review also showed that the lab’s third-party biller had insufficient systems in place to prevent such errors.
“Upon learning this, we made the decision to terminate our contract with our third-party biller,” GDL said. “Finally, within 24-hours of identifying the billing error—and prior to the story being published—we rebilled all the claims, refunded payments to the respective payers, and followed up with each payer to ensure receipt of the corrected claims.
“Immediately after the claims were rebilled, we contacted all 205 patients who may have received an incorrect EOB [explanation of benefits], explained what happened, and apologized,” GDL stated.
Going forward, GDL said it will require its new biller to conduct regular audits each quarter and to maintain certain levels of automation and staffing to manage higher volume without disruption. GDL also said it regrets the disruption and inconvenience the billing error caused to its clients and patients.
Lessons for Clinical Laboratories
For clinical laboratories, there are at least four lessons that can be learned from GDL’s experience:
First, labs should be aware of how their own charges for all tests compare with what other labs charge, particularly when charging patients for high-profile tests, such as those for the new coronavirus. What Medicare and other payers charge for these tests has been reported widely, so that many patients are likely aware of the reasonable and customary charges for such tests.
Second, clinical labs may want to note that charging high prices for these tests could lead health insurers to increase their scrutiny of lab charges. The NYT article quoted Angela Meoli, a senior vice president at Aetna, saying, “We’ve seen a small number of laboratories that are charging egregious prices for COVID-19 tests.”
Third, coverage in the NYT often leads other publications to cover the same story. In this case, Kaiser Health News (KHN) and other news organizations have reported on what GDL charged and linked that story to their coverage of surprise medical bills.
Fourth, GDL recommends responding appropriately to journalists’ inquiries. However, lab should be aware that, even then, the news media may not report the facts as labs would prefer.
All of these lessons are important during the COVID-19 pandemic, because newspapers and other news organizations have encouraged consumers to submit copies of their lab tests and other bills. Such examples of charges above normal rates often generate unwanted coverage for hospitals, health systems, healthcare providers, and in this case, a clinical diagnostic laboratory.
All of this may be academic for those clinical laboratory managers and pathologists who scrupulously follow appropriate laws and guidelines for coding, billing, and collecting for clinical lab tests of all types—not just the COVID-19 test. But, year after year, there are individuals who operate certain clinical laboratories and who are willing to push their compliance with long-established laws and regulations for short-term profit. When these abusive lab practices surface and attract the attention of both federal prosecutors and national news media, it is the entire clinical laboratory profession that gets characterized in negative ways.
Certainly, many medical laboratory professionals would agree that the system of enforcing federal and state laws and pursuing obvious cases of fraudulent practices involving clinical lab testing leaves much to be desired. However, there are already several examples of federal prosecutors charging lab owners and managers for violating fraud and anti-kickback statutes in their marketing of COVID-19 tests. Hopefully the national news media will be effective in spotting illegal practices involving COVID-19 testing and bring more transparency to the lab testing marketplace.
Two national studies find pathologists bill out-of-network more frequently than other hospital-based specialties, and one study links that behavior to insurer reimbursement rates
Surprise bills for out-of-network services continue to be an important issue for healthcare consumers. Now comes a recently-released report from the Health Care Cost Institute (HCCI) claiming that pathologists are the specialists that most often bill for out-of-network hospital charges.
The HCCI study examined the prevalence and frequency of out-of-network billing among six specialties. The sample used for the report included 13.8 million healthcare visits to over 35 thousand hospital-based healthcare providers that occurred in 2017. The types of visits examined for the report were:
emergency medicine,
pathology,
radiology,
anesthesiology,
behavioral health, and
cardiovascular services.
The researchers calculated the percentage of out-of-network claims for both inpatient and outpatient visits to each type of the six specialties.
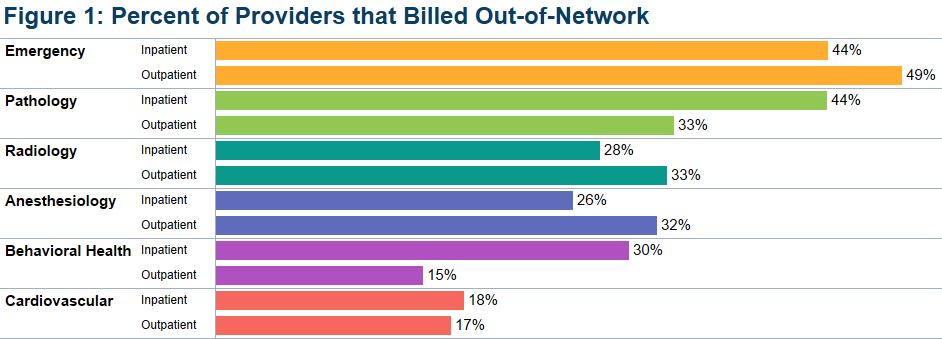
The study found that, overall, less than half of the specialties billed out-of-network for services obtained at in-network facilities. Providers with at least one out-of-network claim associated with an in-network outpatient visit ranged from 15% for behavioral health to 49% for emergency medicine.
Pathologists’ Out-of-Network Billing
Among the pathologists surveyed, HCCI found 33% had at least one out-of-network claim for an in-network outpatient visit. Providers with at least one out-of-network claim associated with an in-network inpatient visit ranged from 18% for cardiovascular services to 44% for both emergency and pathology services.
HCCI researchers also examined how often individual providers in the six specialties billed out-of-network at least one time and found that the majority billed out of network less than 10% of the time. However, this varied among the specialties with 36% of pathologists who billed out-of-network for inpatient visits, and 20% of pathologists who billed out-of-network for outpatient visits, did so more than 90% of the time.
The graphic above, taken from the latest HCCI report, shows “the share of providers who billed out-of-network at least once for inpatient and outpatient visits” and illustrates the percentage of out-of-network billings by pathologists compared to other hospital-based healthcare specialties. (Graphic copyright: Health Care Cost Institute.)
Pathologists Top List of Out-of-Network Specialists in Previous HCCI report
Last November, HCCI released a similar report that examined the commonality of out-of-network billing for the same six specialties plus surgical services that took place in 2017. Based on their collected data, they also estimated the amount of surprise bills that patients could expect to receive for those services.
That report found that nationally:
16.5% of visits with emergency room services had an out-of-network claim from an emergency medicine specialist.
12.9% of visits with lab/pathology services had an out-of-network claim from a pathologist.
8.3% of visits with anesthesiology services had an out-of-network claim from an anesthesiologist.
6.7% of visits with behavioral health services had an out-of-network claim from a behavioral health provider.
4.2% of visits with radiology services had an out-of-network claim from a radiologist.
2.1% of visits with surgical services had an out-of-network claim from a surgeon.
2.0% of visits with cardiovascular services had an out-of-network claim from a cardiovascular specialist.
Surgical Services the Most Expensive Out-of-Network Bill
This study also found broad variation in charges between types of services and healthcare settings. The researchers determined that the potential surprise bills for surgical visits due to out-of-network claims were of the greatest magnitude. HCCI estimated that the average potential surprise bill associated with an inpatient surgery was $22,248, while the potential surprise bill associated with an outpatient surgery was $8,493.
Out-of-Network Surprise Billing Varies Widely Depending on Location
The data was further broken down by state. For pathology services, the percentage of visits with out-of-network services in 2017 ranged from 0.3% in Minnesota to 75.3% in Kansas. HCCI researchers estimated the potential surprise bill for out-of-network pathology claims for inpatient services ranged from $14 in Louisiana to $167 in Delaware. The estimated surprise bill for out-of-network outpatient pathology services ranged from $23 in Louisiana to $218 in Wyoming.
Pathologists Also Top Out-of-Network Biller in Yale University Study
A Yale University study into surprise billing released in December and published in the journal Health Affairs found similar results, Modern Healthcare reported. This study examined surprise out-of-network bills incurred by patients who sought care at in-network hospitals for four types of specialists that are not chosen by patients:
pathologists,
anesthesiologists,
radiologists, and
assistant surgeons.
Zack Cooper, PhD (above), is an associate professor of public health at the Yale School of Public Health and one of the study’s authors. He noted in Yale News, “When physicians whom patients do not choose and cannot avoid bill out of network, it exposes people to unexpected and expensive medical bills and undercuts the functioning of US healthcare markets,” adding, “Moreover, the ability to bill out of network allows specialists to negotiate inflated in-network rates, which are passed on to consumers in the form of higher insurance premiums.” (Photo copyright: Yale School of Public Health.)
For the Yale study, the researchers examined employer-sponsored insurance claims from a major commercial insurer for healthcare visits that occurred at in-network hospitals in 2015. They found that 12.3% of cases involving a pathologist were billed out-of-network, which was the highest percentage of the four specialties analyzed. By contrast, 11.8% of anesthesiologists, 11.3% of assistant surgeons, and 5.6% of radiologists billed out-of-network for their services.
The Yale study also found that “the ability of these four specialties to send patients out-of-network bills allowed them to negotiate high in-network payments from insurers, which leads to higher insurance premiums for individuals.”
The Yale study researchers determined that were these specialists unable to bill out-of-network, the particular healthcare plan would save 3.4% of their expenditures or about $40 billion per year, Modern Healthcare reported.
Surprise bills for out-of-network services burden both patients and providers. Insurers want beneficiaries to have access to hospitals and services, but providers in many specialties do not want to contract with those insurers due to low reimbursements.
This disconnect results in providers staying out-of-network and patients receiving surprise bills for out-of-network services even though the hospital was in-network. And pathologists are at the top of the list.
Anatomic pathologists across the country will want to track how government and private payers respond to these findings by amending coverage and reimbursement guidelines in ways that may be unfavorable to the pathology profession.
This is another example of technology companies working to develop medical laboratory testing that consumers can use without requiring a doctor’s order for the test
Here’s new technology that could be a gamechanger in the fight against COVID-19 if further research allows it to be used in patient care. The goal of the researchers involved is to enable individuals to test for the SARS-CoV-2 coronavirus from home with the assistance of a smartphone app enhanced by artificial intelligence (AI).
Such an approach could bypass clinical laboratories by allowing potentially infected people to confirm their exposure to the coronavirus and then consult directly with healthcare providers for diagnosis and treatment.
The at-home test is being developed through a partnership between French pharmaceutical company Sanofi and San Jose, Calif.-based Luminostics, creator of a smartphone-based diagnostic platform that “can detect or measure bacteria, viruses, proteins, and hormones from swabs, saliva, urine, and blood,” according to the company’s website.
Users who wish to self-test collect a specimen from their nose via a swab and then insert that swab into a device attached to a smartphone. The device uses chemicals and nanoparticles to examine the collected sample. If the individual has the virus, the nanoparticles in the specimen glow in a way visible to smartphone cameras. The device generates data and AI in the smartphone app processes a report. The app informs the user of the results of this COVID-19 test, and it also enables the user to connect to a doctor directly through telehealth video conferencing to discuss a diagnosis.
“This partnering project could lead to another important milestone in Sanofi’s fight against COVID-19,” said Alan Main, Sanofi’s Executive Vice President, Consumer Healthcare, and Chair of the Global Self-Care Federation, in a press release. “The development of a self-testing solution with Luminostics could help provide clarity to individuals—in minutes—on whether or not they are infected.” (Photo copyright: Global Self-Care Federation.)
According to the press release, the diagnostic platform is composed of:
an iOS/Android app to instruct a user on how to run the test, capture and process data to display test results, and then to connect users with a telehealth service based on the results;
a reusable adapter compatible with most types of smartphones; and
consumables for specimen collection, preparation, and processing.
The COVID-19 test results are available within 30 minutes or less after collecting the sample, notes the Sanofi press release. Advantages cited for having a fast, over-the-counter (OTC) solution for COVID-19 testing include:
easy access and availability;
reduced contact with others, which lowers infection risk; and
timely decision-making for any necessary treatments.
The two companies plan to have their COVID-19 home-testing application available for the public before the end of the year, subject to government regulatory clearances. They intend to make their OTC solution available through consumer and retail outlets as well as ecommerce sites.
Can Sound Be Used to Diagnose COVID-19?
Another smartphone app under development records the sound of coughs to determine if an individual has contracted COVID-19. Researchers at the Swiss Federal Institute of Technology Lausanne (École Polytechnique Fédérale de Lausanne or EPFL) in Switzerland created the Cough-based COVID-19 Fast Screening Project (Coughvid), which utilizes a mobile application and AI to analyze the sound of a person’s cough to determine if it resembles that of a person infected with the SARS-CoV-2 coronavirus.
The inspiration for this project came from doctors who reported that their COVID-19 patients have a cough with a very distinctive sound that differs from other illnesses. The cough associated with COVID-19, according the EPFL website, is a dry cough that has a chirping intake of breath at the end.
“The World Health Organization (WHO) has reported that 67.7% of COVID-19 patients exhibit a ‘dry cough,’ meaning that no mucus is produced, unlike the typical ‘wet cough’ that occurs during a cold or allergies. Dry coughs can be distinguished from wet coughs by the sound they produce, which raises the question of whether the analysis of the cough sounds can give some insights about COVID-19. Such cough sounds analysis has proven successful in diagnosing respiratory conditions like pertussis [Whooping Cough], asthma, and pneumonia,” states the EPFL website.
“We have a lot of contact with medical doctors and some of them told us that they usually were able to distinguish, quite well, from the sound of the cough, if patients were probably infected,” Tomas Teijeiro Campo, PhD, Postdoc Researcher with EPFL and one of the Coughvid researchers, told Business Insider.
The Coughvid app is in its early developmental stages and the researchers behind the study are still collecting data to train their AI. To date, the scientists have gathered more than 15,000 cough samples of which 1,000 came from people who had been diagnosed with COVID-19. The app is intended to be used as a tool to help people decide whether to seek out a COVID-19 clinical laboratory test or medical treatment.
“For now, we have this nice hypothesis. There are other work groups working on more or less the same approach, so we think it has a point,” said Teijeiro Campo. “Soon we will be able to say more clearly if it’s something that’s right for the moment.”
With additional research, innovative technologies such as these could change how clinical laboratories interact with diagnosticians and patients during pandemics. And, if proven accurate and efficient, smartphone apps in the diagnosis process could become a standard, potentially altering the path of biological specimens flowing to medical laboratories.
Two major clinical laboratory conferences reschedule, as the SARS-CoV-2 pandemic continues to disrupt long-planned events; Many labs are losing money as fewer patients visit physicians
This week, the ongoing Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic was responsible for two important developments in the clinical laboratory industry. Both involved the rescheduling of major annual conferences. In both cases, conference organizers are placing different bets on when they think the COVID-19 outbreak, the illness caused by the SARS-CoV-2 coronavirus, will have passed and when they believe some semblance of normalcy will return to both social interaction and business activities.
On Monday, the American Association of Clinical Chemistry (AACC) announced that it would reschedule its 2020 AACC annual meeting and exhibition—originally scheduled for July 26-30, 2020, at McCormick Place in Chicago—to Dec. 13-17, 2020, also at McCormick Place.
On the same day, Dark Daily’s sister publication, The Dark Report, announced it had rescheduled the 25th annual Executive War College on Laboratory and Pathology Management to new dates and to a new hotel. This conference will now take place on July 14-15, 2020, at the Hyatt Regency Hotel in New Orleans. This is a change from the originally scheduled date of April 28-29, 2020, and from the original location, the Sheraton New Orleans Hotel.
On its website, AACC stated: “Based on input from all stakeholder groups, and in close collaboration with host city officials, the organization is pleased to announce that AACC will be able to preserve the complete Annual Scientific Meeting and Clinical Lab Expo experience to which its members, exhibitors, and the entire laboratory medicine community have been looking forward. The 2020 AACC Annual Scientific Meeting and Clinical Lab Expo will now be held December 13-17, 2020, at McCormick Place in Chicago, IL, USA.”
Each conference claims to be “the largest” in some
dimension. Each year, AACC’s annual conference attracts more than 20,000
attendees, as measured by clinical chemists and other visitors to its Expo,
which features more than 750 lab companies.
While the Executive War College claims to be the largest conference serving the business, management, operations, and financial health needs of clinical laboratories and pathology groups. Each year, it hosts almost 900 attendees—generally senior administrators, lab executives, pathologist-business leaders, consultants, and in vitro diagnostics (IVD) manufacturers. The conference is supported by more than 50 corporate benefactors and sponsors.
AACC’s rescheduling of its conference from July to December
will delay two important activities:
Many lab scientists planning to attend were hoping to participate in the first assessments of the novel coronavirus pandemic, assuming that the pandemic had passed by mid-summer.
During AACC is when the nation’s major IVD manufacturers and companies that sell lab automation, instruments, test kits, reagents, and other products introduce their latest-generation solutions. Now, many of those product launches will be pushed back to December.
Meanwhile, organizers of the Executive War College are betting that the novel coronavirus pandemic will taper down, possibly synchronized with the end of the annual influenza season in North America, which is typically sometime in April or early May.
If this proves true, then conducting the conference on July 14-15, 2020, will give lab leaders the opportunity to gather and share lessons learned during this COVID-19 outbreak in time to prepare for a possible second outbreak of COVID-19 when the next influenza season arrives in the fall. It will also be an important opportunity for lab managers and pathologists to learn ways to restore revenue lost during the pandemic.
Clinical Laboratories, Pathology Groups, Hospitals, at
Brink of Financial Ruin
“What has gone unrecognized by the national news media is how the novel coronavirus pandemic is causing financial devastation to the finances of the nation’s clinical laboratories and anatomic pathology groups,” stated Robert L. Michel, Editor-in-Chief of The Dark Report and Founder of the Executive War College. “In absolute terms, the pandemic is a growing financial disaster to the medical lab industry, and it will take years for many labs to rebuild the staff that they have laid off or terminated in recent months in order to stay operational.
“Why are all labs losing money at this time?” asked Michel.
“The answer is simple—beginning early in March, patients stopped visiting their
doctors. Hospitals ceased to admit patients for elective procedures. Fewer
patients per day means fewer lab test referrals per day and loss of the revenue
generated by those claims that pays the salaries and expenses of the labs
performing those tests. Laying off or furloughing staff is one way labs lower
costs in response to lower income.
“Many clinical labs, pathology groups, and the hospitals
they serve are steadily approaching financial ruin,” he continued. “Every week
the pandemic continues, and North American citizens are advised to shelter in
place, forces labs to draw down their dwindling financial reserves to keep
their doors open.”
Robert Michel (above), Editor-in-Chief of The Dark Report and Dark Daily and Founder of The Dark Intelligence Group, will host the 25th anniversary Executive War College on Lab and Pathology Management on July 14-15, 2020, in New Orleans. Attendees from clinical laboratories and pathology groups will gain critical insights from such learning opportunities as: “Preparing Your Lab for a Second Outbreak of COVID-19,” and “Rapidly Building Cash Flow and Restoring Your Lab’s Financial Stability Post-Pandemic.” (Photo copyright: The Dark Report.)
This crisis has created three big questions that labs need
to answer:
How much longer will the COVID-19 pandemic last
before some degree of normalcy is restored (meaning patient office visits resume
and physicians begin ordering lab tests every day)?
If there is a second outbreak of SARS-CoV-2 this
fall, what does every lab need to know to be ready?
As American society and business return to
normal, how can labs quickly build up cash flow, collect more revenue, and
restore financial stability?
“Given the unknown aspects of the SARS-CoV-2 coronavirus,
the answer to the first question is a crap-shoot. But to reschedule the
Executive War College to dates that are 14 weeks away seems a reasonable bet,”
noted Michel. “The pay-off to that bet is the ability to provide the owners and
leaders of the nation’s labs answers to the second and third questions.
“The 14 weeks between now and mid-July give us the
opportunity to organize sessions and invite speakers who can provide answers
and information to help labs with their two most pressing needs: to be prepared
for another COVID-19 outbreak later this year, and to restore cash flow and
financial health as soon as possible,” said Michel. “This will be the very
first opportunity for lab managers and pathologists to assemble, learn the
COVID-19 lessons from successful labs, gain financial insights, and network
with their peers.”
The Executive War College team is inviting suggestions for
speakers and session topics for the July 14-15 conference. The original agenda
that was taking shape for the planned dates of April 28-29 will be revised so
as to include presentations now directly relevant to the state of the clinical
lab and pathology professions for mid-year 2020. Send your suggestions for
topics and speakers to info@darkreport.com.
Information on registering for the 25th annual Executive War College, and on placing reservations at the Hyatt Regency Hotel in New Orleans, is available on the EWC website (or copy and paste this URL in your browser: https://www.executivewarcollege.com.)
People already registered for Executive War College 2020
will have their registrations automatically applied to the new July 14-15
dates.
At The Dark Report’s annual Lab Quality Confab for clinical laboratory administrators, managers, and quality team members, experts outline how disruption in healthcare requires labs to improve processes and cut costs
This is an opportunity for clinical laboratory directors,
pathologists, and other lab professionals, to comment on the proposed revisions
to CLIA before or during the upcoming CLIAC meeting on Nov. 6.
The agenda for the meeting is posted on the CDC’s website.
Public to be Heard on CLIA Regulations
“For the first time in its 26-year history, the council has
called for three workgroups to address how to revise CLIA,” Salerno said. The
workgroups will address these topics:
“It’s a dramatic step for the government to ask the
laboratory community how to revise the CLIA regulations,” Salerno commented.
Chartered in 1992, the advisory council meets twice a year, once in April and
once in November.
In the coming weeks, Dark Daily will publish more
information on how clinical laboratory professionals can comment on the
important issue of CLIA revisions.
Digital slides from Salerno’s keynote address are posted on LQC’s presentations website.
Clinical Laboratory Testing is Increasing in Value,
Keynote Speaker Says
As a service to clinical laboratories, Salerno outlined many
of the services the CDC’s Division of Laboratory Systems provides for free to
clinical labs, including information on such topics as:
During his remarks at the 13th Annual Lab Quality Confab in Atlanta, Salerno had good news for the clinical laboratory professionals in attendance. He said that lab testing was becoming a more valued commodity in healthcare because physicians and other providers were growing increasingly confident in lab test results. [Photo copyright: The Dark Report.]
Healthcare System Disruption Impacts Providers, Including
Clinical Laboratories
Other keynote speakers addressed how disruption in the US
healthcare systems affects provider organizations in significant ways. For
clinical laboratories, such disruption has resulted in reduced payment and
demands for quality improvement and shorter turnaround times.
For all these reasons, quality
management systems may be every clinical laboratory’s best strategy to
survive and thrive, the keynote speakers said.
The first keynoter was Robert L. Michel, Editor-in-Chief and Publisher of The Dark Report. Michel’s remarks focused on how price cuts from Medicare, Medicaid, private payers, and the drive for value-based payment, are requiring labs to do more with less. For this reason, quality management systems are necessary for all labs seeking to improve results, eliminate errors, and cut costs, he said.
“The people closest to the work know how to fix these
problems,” he added. “That’s why labs know they must train their staff to
identify problems and then report them up the chain so they can be fixed,”
Michel commented. “Labs that are best at listening to their employees are
getting very good at identifying problems by measuring results and monitoring
and reporting on their own performance.”
Michel identified three principle factors that are
disrupting healthcare:
The shift from reactive care in which the health system cares for sick patients to proactive care in which the health system aims to keep patients healthy and out of the hospital and other costly sites of care.
The transition away from fee-for-service payment that encourages providers to do more for patients, whether more care is needed or not, to value-based payment that aims to reward providers for keeping patients healthy.
The consolidation among hospitals, health systems, physicians, and other providers. A trend that requires clinical laboratories to find new partners and new ways to improve lab services and reduce costs.
Informatics Performance Data Help Clinical Laboratories
Respond to Change
“The attributes of new and successful labs are that they will have faster workflow and shorter cycle times for clinical lab tests and anatomic pathology specimen results,” Michel explained. “That means that labs will attack non-value-added processes by implementing continuous improvement strategies [such as Lean and Six Sigma] and by the sophisticated use of informatics.”
Making use of performance data enables clinical laboratory
directors to make changes in response to disruptions that affect healthcare.
“If you have good informatics, then seven or eight of every 10 decisions you
make will be good decisions, and with the other two and three decisions, you’ll
have time to pull back and adjust,” Michel commented.
The second keynote speaker, Jeremy Schubert, MBA, MPH, Division Vice President of Abbott, reiterated what Michel said about how the health system is moving away from fee-for-service payment. Instead of focusing on caring for sick patients exclusively, he said, health insurers are paying all healthcare providers to keep patients healthy.
“Healthcare today is about the whole life course of the
individual,” Schubert explained. “Patients no longer want healthcare only when
they’re sick. Instead, they want to be healthy. And health creation is not just
about a person’s physical health. It’s about their mental health, their
emotional health, and their social wellbeing.
“In fact,” he continued, “you can learn more about a
person’s health from their Zip code than from their genetic code.”
That is essentially what TriCore Reference Laboratories (TriCore) has been doing in New Mexico, Schubert added. During his presentation, Michel mentioned TriCore as being one of four clinical laboratories participating in Project Santa Fe, a non-profit organization that promotes the movement from Clinical Lab 1.0 to Clinical Lab 2.0. (See “TriCore Forges Ahead to Help Payers Manage Population Health,” The Dark Report, May 20, 2019.)
“If you want to be a quality engine in healthcare you have
to be operating at Lab 2.0. Who is best qualified to interpret information?
It’s the lab,” Schubert said. Then he challenged labs to begin pursuing the
goal of achieving Lab 3.0, saying “Lab 3.0 is being able to interface with the
patient to address each patient’s problems.”
The 13th Annual Lab Quality Confab (LQC) in Atlanta continues through the 17th with post-event workshops in Six Sigma and mastering quality management systems. In attendance are 300 clinical laboratory administrators, managers, and quality team members who are learning a complete array of professional training methods.
To register to attend, click here or enter https://www.labqualityconfab.com/register into your browser, or call 707-829-9485, or e-mail lqcreg@amcnetwork.com.
How medical laboratories can show value through process improvement methods and analytics will be among many key topics presented at the upcoming Lab Quality Confab conference
Quality management is the clinical laboratory’s best strategy for surviving and thriving in this era of shrinking lab budgets, PAMA price cuts, and value-based payment. In fact, the actions laboratories take in the next few months will set the course for their path to clinical success and financial sustainability in 2020 and beyond.
But how do medical laboratory managers and pathologists address these challenges while demonstrating their lab’s value? One way is through process improvement methods and another is through the use of analytics.
Clinical pathologists, hospital lab leaders, and independent lab executives have told Dark Daily that the trends demanding their focus include:
Ensuring needed resources and appropriate tests,
while the lab is scrutinized by insurance companies and internally by hospital
administration;
“Our impact on patient care, in many cases, is very
indirect. So, it is difficult to point to outcomes that occur. We know things
we do matter and change patient care, but objectively showing that is a real
struggle. And we are being asked to do more than we ever had before, and those
are the two big things that keep me up at night these days,” he added.
This is where process improvement methods and analytics are
helping clinical laboratories understand critical issues and find opportunities
for positive change.
“You need to have a strategy that you can adapt to a changing landscape in healthcare. You have to use analytics to guide your progress and measure your success,” Patricia Nortmann, System Director of Laboratory Services at St. Elizabeth Healthcare, Erlanger, Ky., told Dark Daily.
Clinical Laboratories Can Collaborate Instead of Compete
Prior to a joint venture with TriHealth in Cincinnati, St. Elizabeth lab leaders used data to inform their decision-making. Over about 12 years preceding the consolidation of labs they:
Implemented front-end automation outside the core area and in the microbiology lab.
“We are now considered a regional reference lab in the state
of Kentucky for two healthcare organizations—St. Elizabeth and TriHealth,”
Nortmann said.
Thanks to these changes, the lab more than doubled its
workload, growing from 2.1 million to 4.3 million outreach tests in the core
laboratory, she added.
Christopher Doern, PhD (left), Director of Microbiology and Associate Professor of Pathology at Virginia Commonwealth University Health System; Patricia Nortmann (center), System Director of Laboratory Services at St. Elizabeth Healthcare; and Joseph Cugini (right), Manager Client Solutions at Health Network Laboratories, will present practical solutions and case studies in quality improvement and analytics for clinical laboratory professionals at the 13th Annual Lab Quality Confab, October 15-16, 2019, at the Hyatt Regency in Atlanta, Ga. (Photo copyright: The Dark Report.)
Using Analytics to Test the Tests
Clinical laboratories also are using analytics and information technology (IT) to improve test utilization.
At VCH Health, Doern said an analytics solution interfaces
with their LIS, providing insights into test orders and informing decisions
about workflow. “I use this analytics system in different ways to answer
different questions, such as:
How are clinicians using our tests?
When do things come to the lab?
When should we be working on them?
“This is important for microbiology, which is a very delayed
discipline because of the incubation and growth required for the tests we do,”
he said.
Using analytics, the lab solved an issue with Clostridium
difficile (C diff) testing turnaround-time (TAT) after associating it with
specimen transportation.
Inappropriate or duplicate testing also
can be revealed through analytics. A physician may reconsider a test after discovering
another doctor recently ordered the same test. And the technology can guide
doctors in choosing tests in areas where the related diseases are obscure, such
as serology.
Avoiding Duplicate Records While
Improving Payment
Another example of process
improvement is Health Network Laboratories (HNL) in Allentown, Pa. A team there established an enterprise master patient index (EMPI) and implemented digital tools to find and eliminate
duplicate patient information and improve lab financial indicators.
“The system uses trusted sources of data to make sure data is clean and the lab has what it needs to send out a proper bill. That is necessary on the reimbursement side—from private insurance companies especially—to prevent denials,” Joseph Cugini, HNL’s Manager Client Solutions, told Dark Daily.
HNL reduced duplicate records in its database from 23% to
under one percent. “When you are talking about several million records, that is
quite a significant improvement,” he said.
Processes have improved not only on the billing side, but in
HNL’s patient service centers as well, he added. Staff there easily find
patients’ electronic test orders, and the flow of consumers through their
visits is enhanced.
Learn More at Lab Quality Confab Conference
Cugini, Doern, and Nortmann will speak on these topics and more during the 13th Annual Lab Quality Confab (LQC), October 15-16, 2019, at the Hyatt Regency in Atlanta, Ga. They will offer insights, practical knowledge, and case studies involving Lean, Six Sigma, and other process improvement methods during this important 2-day conference, a Dark Dailynews release notes.
Register for LQC, which is produced by Dark Daily’s sister publication The Dark Report, online at https://www.labqualityconfab.com/register, or by calling 512-264-7103.