Clinical laboratories nationwide could follow Yale’s example and enact programs to bring much needed lab services to traditionally underserved communities
Ever since the COVID-19 pandemic drove up demand for telehealth medical services, mobile clinical laboratories have grown in popularity as well, especially among residents of remote and traditionally underserved communities. Now, several divisions of Yale University are getting in on the trend.
“Using a van retrofitted with laboratory-grade diagnostic equipment, the mobile clinic will employ SalivaDirect—a saliva-based COVID-19 PCR test developed at YSPH—to facilitate on-site testing with a turnaround time of two to three hours,” Yale Daily News reported.
Funded by a federal grant, the initial goal was to provide 400 free COVID-19 tests, but the program has exceeded that number. By April 10, the mobile lab had been deployed more than 60 times, appearing at events and pop-up sites throughout various communities in Connecticut, including regular stops at the WHEAT Food Pantry of West Haven.
“[The clinical laboratory-in-a-van] is a brilliant way to reduce the barriers to testing, instead taking the lab to communities who may be less likely—or unable—to access the necessary clinic or labs,” microbiologist Anne Wyllie, PhD, a research scientist who helped develop the PCR test deployed by the mobile lab told Yale Daily News. Wyllie works in the Department of Epidemiology of Microbial Diseases at Yale School of Public Health. “We are actively working with our community partners to identify how we can best serve their communities,” she added. (Photo copyright: Yale School of Medicine.)
Mobile Lab’s Capabilities
Collecting samples, processing, and delivering same-day COVID-19 results was the initial goal but that plan has expanded, Yale School of Medicine noted in a news release.
“Same-day onsite delivery of test results is an added benefit for communities and individuals without access to Wi-Fi or the ability to receive private health information electronically,” Yale added.
The mobile van is staffed with trained clinical laboratory technicians as well as community health navigators who provide both healthcare information and proper follow-up connections as needed for patients who receive positive COVID-19 results. The van runs off power from outdoor electrical outlets at each location and currently serves historically underserved populations in Hartford, Middlesex, Fairfield, New Haven, and New London counties, Yale noted.
“The van allows us to bring our services, as well as healthcare information, directly to communities where they are needed,” said Angelique Levi, MD, Associate Professor, Vice Chair and Director of Pathology Reference Services, and CLIA Laboratory Medical Director in the Department of Pathology at Yale University School of Medicine in a news release.
Launch of a High Complexity Molecular Lab on Wheels
YPL and YSPH collaborated to make the mobile lab a reality. YSPH created the saliva-based COVID-19 test and YPL “provided clinical validation necessary to get the testing method ready for emergency use authorization by the US Food and Drug Administration,” Yale noted.
“YPL recognized the need to be closer to the front lines of patient care and that retrofitting a fully licensed, high complexity molecular laboratory into a consumer-sized van was the right next step,” Chen Liu, MD, PhD, Chair of the Department of Pathology at Yale School of Medicine, noted in a Yale news release. This “gives us options to efficiently deliver accurate diagnostic information when and where it’s needed,” he added.
Throughout the COVID-19 pandemic, the Connecticut Department of Public Health, the City of New Haven, and various community organizations partnered with YPL, YSPH, and the SalivaDirect team to offer free SARS-CoV-2 testing to the public at two different sites in New Haven.
Principal investigators Levi and microbiologist Anne Wyllie, PhD, who helped develop the PCR test deployed by the mobile, lab led the Yale lab-in-a-van research project.
Flambeau Diagnostics, a biomedical company that specializing in mobile lab testing, worked with the Yale team to design and implement the mobile lab van.
“According to Wyllie, the new YSPH and YPL initiative utilizes one of the former Flambeau vans that had been retrofitted for clinical testing,” a Yale news release noted.
Kat Fajardo, Laboratory Manager at Yale University, added custom pieces of equipment to ensure seamless PCR testing. One was a Magnetic Induction Cycler (Mic) measuring only six by six inches. The Mic allowed for measurement of 46 biological specimens, while it’s diminutive size freed up space on the van’s countertop. This allowed lab techs to process specimens concurrently while also providing COVID-19 testing, according to a Yale news release.
Additionally, the van has a Myra portable robotic liquid handler which is “designed to automate the process of moving clinical specimens between vials,” the news release notes.
“What we wanted to do is run high complexity testing in the van, with a reduced timeframe, and then be able to get the results out to the patients as soon as we possibly could,” Fajardo stated.
Exploring the Mobile Laboratory’s Potential
According to a news release, YPL and YSPH consult with community partners to select locations for the mobile lab to visit. These partners include:
APT Foundation (New Haven County, in addition to others.
Although the van was initially used to provide SalivaDirect COVID-19 testing to vulnerable populations, YPL is working with its partners in those communities to identify other testing needs beyond COVID.
The Yale team is considering additional offerings and support such as the addition of a social worker as well as expanding lung health awareness beyond COVID-19 to other respiratory diseases. Also under consideration:
Vaccinations including for COVID-19 and Hepatitis B, and
Health education and materials for harm reduction and STI prevention, a Yale news release noted.
Yale’s Laboratory-in-a-Van program is a consumer-facing effort that is bringing much needed clinical lab services to traditionally underserved communities in Connecticut. Clinical laboratories throughout the nation could do the same with remote or homebound patients who cannot reach critical care.
Clinical laboratories and pathologists should expect to receive increase referrals from oncologists with younger patients
More people are getting serious cases of cancer at younger and younger ages. So much so that some anatomic pathologists and epidemiologists are using the term “Turbo Cancers” to describe “the recent emergence of aggressive cancers that grow very quickly,” Vigilant News reported.
Cancer continues to be the second leading cause of death in the United States and current trends of the disease appearing in younger populations are causing alarm among medical professionals and scientists.
“Because these cancers have been occurring in people who are too young to get them, basically, compared to the normal way it works, they’ve been designated as turbo cancers,” Harvey Risch, MD, PhD, Professor Emeritus of Epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine, in an interview with Epoch TV’sAmerican Thought Leaders.
It’s anatomic pathologists who receive the biopsies and analyze them to diagnose the cancer. Thus, they are on the front lines of seeing an increased number of biopsies for younger patients showing up with the types of cancers that normally take many years to grow large enough to be discovered by imaging and lumps leading to biopsy and diagnosis. It’s a medical mystery that may have long term effects on younger populations.
“What clinicians have been seeing is very strange things,” said Harvey Risch, MD, PhD (above), Professor Emeritus of Epidemiology at the Yale School of Public Health and Yale School of Medicine, in an Epoch TV interview. “For example, 25-year-olds with colon cancer, who don’t have family histories of the disease—that’s basically impossible along the known paradigm for how colon cancer works—and other long-latency cancers that they’re seeing in very young people.” Epidemiologists and anatomic pathologists are describing these conditions as “turbo cancers.” (Photo copyright: Yale University.)
Early-Onset Cancer Rates Jump Sharply
According to the federal Centers for Disease Control and Prevention (CDC), about 3.3 million Americans died in 2022, and 607,800 of those deaths were attributed to cancer. This statistic translates to approximately 18.4% of US deaths being due to cancer last year.
An article published in the Journal of the American Medical Association titled, “Patterns in Cancer Incidence among People Younger than 50 Years in the US, 2010 to 2019,” states that the rates of cancer in people under the age of 50 has risen sharply in recent years. The study found that “the incidence rates of early-onset cancer increased from 2010 to 2019. Although breast cancer had the highest number of incident cases, gastrointestinal cancers had the fastest-growing incidence rates among all early-onset cancers.”
The largest increase in cancer diagnoses occurred in people in the 30 to 39-year-old age group. This number represents a jump of almost 20% for the years analyzed for individuals in that demographic. The researchers also found that cancer rates decreased in individuals over the age of 50.
Breast cancer, which increased by about 8% in younger people, accounted for the most diagnoses in this age group. However, the biggest increase was 15% for gastrointestinal cancers, including colon, appendix, bile duct, and pancreatic cancer.
Because cancer can recur or progress, researchers have concerns about what happens to young cancer patients as they grow older and what effect cancer may have on their lives.
“They are at a transitional stage in life,” Chun Chao, PhD, Research Scientist, Division of Epidemiologic Research at Kaiser Permanente, told The Hill. “If you think about it, this is the age when people are trying to establish their independence. Some people are finishing up their education. People are trying to get their first job, just start to establish their career. And people are starting new families and starting to have kids. So, at this particular age, having a cancer diagnosis can be a huge disruption to these goals.”
Sadly, young cancer survivors have a heightened risk of developing a second cancer and a variety of other health conditions, such as cardiovascular diseases and metabolic disorders.
Lifestyle a Factor in Increased Risk for Cancer
“The increase in early-onset cancers is likely associated with the increasing incidence of obesity as well as changes in environmental exposures, such as smoke and gasoline, sleep patterns, physical activity, microbiota, and transient exposure to carcinogenic compounds,” according to the JAMA study.
“Suspected risk factors may involve increasing obesity among children and young adults; also the drastic change in our diet, like increasing consumption of sugar, sweetened beverages, and high fat,” Hyuna Sung, PhD, Cancer Surveillance Researcher at the American Cancer Society, told US News and World Report. “The increase in cancers among young adults has significant implications. It is something we need to consider as a bellwether for future trends.”
“Increased efforts are required to combat the risk factors for early-onset cancer, such as obesity, heavy alcohol consumption, and smoking,” said Daniel Huang, MD, Assistant Professor of Medicine at the National University of Singapore, one of the authors of the study, in the US News and World Report interview.
Other studies also have shown a rise in so-called turbo cancers.
“Cancer as a disease takes a long time to manifest itself from when it starts. From the first cells that go haywire until they grow to be large enough to be diagnosed, or to be symptomatic, can take anywhere from two or three years for the blood cancers—like leukemias and lymphomas—to five years for lung cancer, to 20 years for bladder cancer, or 30 to 35 years for colon cancer, and so on,” Risch told the Epoch Times.
Not the Occurrence Oncologists Expect
“Some of these cancers are so aggressive that between the time that they’re first seen and when they come back for treatment after a few weeks, they’ve grown dramatically compared to what oncologists would have expected,” Risch continued. “This is just not the normal occurrence of how cancer works.”
Risch believes that damage to the immune system is the most likely cause of the rise in turbo cancers. He said the immune system usually recognizes, manages, and disables cancer cells so they cannot progress. However, when the immune system is impaired, cancer cells can multiply to the point where the immune system cannot cope with the number of bad cells.
It is a statistical fact that more people are being diagnosed with serious cases of cancer at younger and younger ages. If this trend continues, clinical laboratories and pathologists can expect to see more oncology case referrals and perform more cancer diagnostic tests for younger patients.
Though not a replacement for clinical laboratory testing, the CDC says the surveillance system will help slow spread of COVID-19 in vulnerable communities
Clinical laboratory testing for COVID-19 is receiving an ally. In mid-August, the Centers for Disease Control and Prevention (CDC) and the US Department of Health and Human Services (HHS) announced they were initiating a National Wastewater Surveillance System (NWSS) in response to the COVID-19 pandemic.
In collaboration with other federal agencies, the NWSS will work with state, local, territorial, and tribal health departments to collect data on wastewater (aka, sewage) samples throughout the United States.
The goal of the NWSS is to detect SARS-CoV-2, the coronavirus that causes COVID-19, before it spreads by detecting traces of it in local sewer systems. The level of the virus detected in wastewater can be a leading indicator of a worsening outbreak in a community, according to a CDC statement.
“Quantitative SARS-CoV-2 measurements in untreated sewage can provide information on changes in total COVID-19 infection in the community contributing to that wastewater treatment plant,” noted the CDC.
People infected with the coronavirus discard traces of it—whether they are symptomatic or asymptomatic—and levels of the virus in untreated sewage can provide scientists with information about the degree of outbreak in specific areas.
The NWSS will not include or monitor homes that use septic tanks or entities with decentralized systems that treat their own waste, such as hospitals, universities, and prisons.
Not a Replacement for Clinical Laboratory Testing
The CDC stressed that sewage testing is not meant to replace clinical laboratory testing, but it can be a valuable tool in communities where COVID-19 tests are underutilized or unavailable. Wastewater testing, CDC noted in its statement, could have an enormous reach as 80% of households in the US are connected to a municipal sewage system.
The CDC is not actively taking samples from wastewater, but relying on local partners to take samples, test them, and enter data into the NWSS portal for the purpose of summarizing and interpreting for public health action.
The agency predicts that participation in a national database will ensure data comparability across separate jurisdictions.
Could Testing Raw Sewage Be More Effective than Contact Tracing for Tracking COVID-19 Outbreaks?
A Yale University study published in Nature Biotechnology, titled, “Measurement of SARS-CoV-2 RNA in Wastewater Tracks Community Infection Dynamics,” detected SARS-CoV-2 concentrations in sewage sludge in New Haven, Conn., over a 10-week period earlier this year. The results of the study “show the utility of viral RNA monitoring in municipal wastewater for SARS-CoV-2 infection surveillance at a population-wide level,” the study authors noted.
The published study states that “SARS-CoV-2 RNA was detected throughout the more than 10-week study and, when adjusted for time lags, tracked the rise and fall of cases seen in SARS-CoV-2 clinical test results and local COVID-19 hospital admissions. Relative to these indicators, SARS-CoV-2 RNA concentrations in sludge were 0–2 [days] ahead of SARS-CoV-2 positive test results by date of specimen collection, 0–2 [days] ahead of the percentage of positive tests by date of specimen collection, 1–4 [days] ahead of local hospital admissions and 6–8 [days] ahead of SARS-CoV-2 positive test results by reporting date.”
The Yale researchers concluded, “Our results demonstrate that measurement of SARS-CoV-2 RNA concentrations in primary sludge provides an approach to estimate changes in COVID-19 prevalence on a population level. Sludge results were not a leading indicator compared to positive test results or percentage of positive tests by date of specimen collection. However, they led hospitalizations by 1–4 [days] and test results by report date by ~1 week. Thus, in communities where test reporting is delayed, sludge results, if analyzed and reported on the same day as sampling, can provide substantial advance notice of infection dynamics.”
Jordan Peccia, Jr., PhD (above), Professor of Chemical and Environmental Engineering at the Yale School of Engineering and Applied Science, and study author, told NBC News, “There’s still a lot more to do. We’re one of the earlier groups to have developed a robust relationship between wastewater and coronavirus cases, but this is just a first step.” He added, “It doesn’t replace contact tracing. [But] if we know a little bit ahead of time, we can raise the alarm.” (Photo copyright: Yale University.)
Sewage Testing for COVID-19 Around the World
Sewage testing can provide data to complement other collected information about COVID-19 and steer public health decision-making. However, the CDC notes that “it is not possible to reliably and accurately predict the number of infected individuals in a community based on sewage testing” and that “more data on fecal shedding by infected individuals over the course of disease are needed to better understand the limits of detection.”
Nevertheless, some experts have leaned heavily on sewage sample testing for their conclusions about the origination of the coronavirus. In August, Dark Daily reported on a theory based on finding remnants of SARS-CoV-2 in sewage systems that suggested the virus may not have originated in Wuhan, China. Analysis of sewage samples in Italy, Spain, and Brazil indicated the virus was present in those countries before the disease was known to exist outside of China. The controversy over these findings has motivated virologists to expand wastewater testing.
The creation of the NWSS by the CDC validates growing interest in new methods of testing for infectious disease. Lower cost, faster response time, more automation of genetic sequencing, and improved analytical software has enabled this type of testing to become a useful tool. It would be wise for clinical laboratory managers to monitor the expanded use of new testing technologies for infectious diseases.
Two national studies find pathologists bill out-of-network more frequently than other hospital-based specialties, and one study links that behavior to insurer reimbursement rates
Surprise bills for out-of-network services continue to be an important issue for healthcare consumers. Now comes a recently-released report from the Health Care Cost Institute (HCCI) claiming that pathologists are the specialists that most often bill for out-of-network hospital charges.
The HCCI study examined the prevalence and frequency of out-of-network billing among six specialties. The sample used for the report included 13.8 million healthcare visits to over 35 thousand hospital-based healthcare providers that occurred in 2017. The types of visits examined for the report were:
emergency medicine,
pathology,
radiology,
anesthesiology,
behavioral health, and
cardiovascular services.
The researchers calculated the percentage of out-of-network claims for both inpatient and outpatient visits to each type of the six specialties.
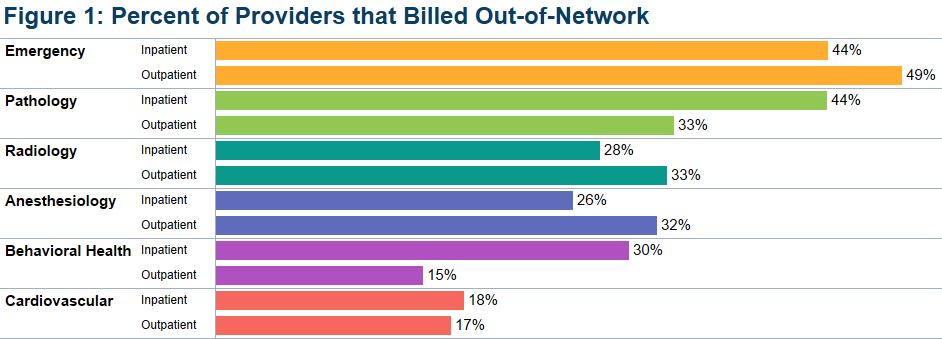
The study found that, overall, less than half of the specialties billed out-of-network for services obtained at in-network facilities. Providers with at least one out-of-network claim associated with an in-network outpatient visit ranged from 15% for behavioral health to 49% for emergency medicine.
Pathologists’ Out-of-Network Billing
Among the pathologists surveyed, HCCI found 33% had at least one out-of-network claim for an in-network outpatient visit. Providers with at least one out-of-network claim associated with an in-network inpatient visit ranged from 18% for cardiovascular services to 44% for both emergency and pathology services.
HCCI researchers also examined how often individual providers in the six specialties billed out-of-network at least one time and found that the majority billed out of network less than 10% of the time. However, this varied among the specialties with 36% of pathologists who billed out-of-network for inpatient visits, and 20% of pathologists who billed out-of-network for outpatient visits, did so more than 90% of the time.
The graphic above, taken from the latest HCCI report, shows “the share of providers who billed out-of-network at least once for inpatient and outpatient visits” and illustrates the percentage of out-of-network billings by pathologists compared to other hospital-based healthcare specialties. (Graphic copyright: Health Care Cost Institute.)
Pathologists Top List of Out-of-Network Specialists in Previous HCCI report
Last November, HCCI released a similar report that examined the commonality of out-of-network billing for the same six specialties plus surgical services that took place in 2017. Based on their collected data, they also estimated the amount of surprise bills that patients could expect to receive for those services.
That report found that nationally:
16.5% of visits with emergency room services had an out-of-network claim from an emergency medicine specialist.
12.9% of visits with lab/pathology services had an out-of-network claim from a pathologist.
8.3% of visits with anesthesiology services had an out-of-network claim from an anesthesiologist.
6.7% of visits with behavioral health services had an out-of-network claim from a behavioral health provider.
4.2% of visits with radiology services had an out-of-network claim from a radiologist.
2.1% of visits with surgical services had an out-of-network claim from a surgeon.
2.0% of visits with cardiovascular services had an out-of-network claim from a cardiovascular specialist.
Surgical Services the Most Expensive Out-of-Network Bill
This study also found broad variation in charges between types of services and healthcare settings. The researchers determined that the potential surprise bills for surgical visits due to out-of-network claims were of the greatest magnitude. HCCI estimated that the average potential surprise bill associated with an inpatient surgery was $22,248, while the potential surprise bill associated with an outpatient surgery was $8,493.
Out-of-Network Surprise Billing Varies Widely Depending on Location
The data was further broken down by state. For pathology services, the percentage of visits with out-of-network services in 2017 ranged from 0.3% in Minnesota to 75.3% in Kansas. HCCI researchers estimated the potential surprise bill for out-of-network pathology claims for inpatient services ranged from $14 in Louisiana to $167 in Delaware. The estimated surprise bill for out-of-network outpatient pathology services ranged from $23 in Louisiana to $218 in Wyoming.
Pathologists Also Top Out-of-Network Biller in Yale University Study
A Yale University study into surprise billing released in December and published in the journal Health Affairs found similar results, Modern Healthcare reported. This study examined surprise out-of-network bills incurred by patients who sought care at in-network hospitals for four types of specialists that are not chosen by patients:
pathologists,
anesthesiologists,
radiologists, and
assistant surgeons.
Zack Cooper, PhD (above), is an associate professor of public health at the Yale School of Public Health and one of the study’s authors. He noted in Yale News, “When physicians whom patients do not choose and cannot avoid bill out of network, it exposes people to unexpected and expensive medical bills and undercuts the functioning of US healthcare markets,” adding, “Moreover, the ability to bill out of network allows specialists to negotiate inflated in-network rates, which are passed on to consumers in the form of higher insurance premiums.” (Photo copyright: Yale School of Public Health.)
For the Yale study, the researchers examined employer-sponsored insurance claims from a major commercial insurer for healthcare visits that occurred at in-network hospitals in 2015. They found that 12.3% of cases involving a pathologist were billed out-of-network, which was the highest percentage of the four specialties analyzed. By contrast, 11.8% of anesthesiologists, 11.3% of assistant surgeons, and 5.6% of radiologists billed out-of-network for their services.
The Yale study also found that “the ability of these four specialties to send patients out-of-network bills allowed them to negotiate high in-network payments from insurers, which leads to higher insurance premiums for individuals.”
The Yale study researchers determined that were these specialists unable to bill out-of-network, the particular healthcare plan would save 3.4% of their expenditures or about $40 billion per year, Modern Healthcare reported.
Surprise bills for out-of-network services burden both patients and providers. Insurers want beneficiaries to have access to hospitals and services, but providers in many specialties do not want to contract with those insurers due to low reimbursements.
This disconnect results in providers staying out-of-network and patients receiving surprise bills for out-of-network services even though the hospital was in-network. And pathologists are at the top of the list.
Anatomic pathologists across the country will want to track how government and private payers respond to these findings by amending coverage and reimbursement guidelines in ways that may be unfavorable to the pathology profession.
US hospitals typically spend $2,424/day to provide inpatient care, according to the KFF report
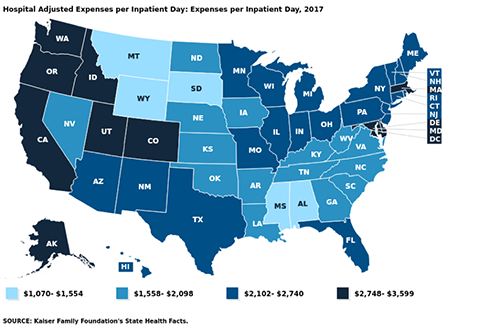
How much does the average hospital spend/day to provide inpatient care? The numbers vary widely, but the latest statistics from Kaiser Family Foundation (KFF) State Health Facts show West Coast states incur the highest daily operating and non-operating inpatient costs.
This disparity in spending is unlikely to surprise medical laboratory executives working in hospital settings. They know firsthand that operating costs can vary from state-to-state and by hospital ownership type.
Oregon, California, and Washington are the most expensive
three states overall for inpatient hospital care. However, the leaderboard
changes when looking specifically at inpatient care at for-profit hospitals.
In the for-profit hospital category:
North Dakota, South Dakota, and Alaska rack up
the highest expenses/day.
Idaho, California, and Oregon top the non-profit
hospital segment.
Overall in the US, the average hospital incurs expenses of
$2,424/inpatient day, the KFF reports.
While the average US hospital spends $2,424/day to deliver inpatient care, West Coast states have the highest hospital adjusted operating and non-operating expenses/inpatient day, according to a recent report from the Kaiser Family Foundation. Oregon hospitals top the spending list at $3,599/day. (Graphic copyright: Kaiser Family Foundation.)
AMA Annual Survey
Rankings
Rankings are based on information from the 1999-2017 American Hospital
Association Annual Survey, which includes all operating and non-operating
expenses for registered US community hospitals. The figures are an estimate of
the expenses incurred by a hospital to provide a day of inpatient care. They
have been adjusted higher to reflect an estimate of the volume of outpatient
services, according to the KFF. The numbers do not reflect actual charges or
reimbursement for the care provided.
Most expensive average expenses/inpatient day:
Oregon, $3,599
California, $3,441
Washington, $3,429
Idaho, $3,119
District of Columbia, $3,053
Least expensive average expenses/inpatient day:
Montana, $1,070
Mississippi, $1,349
South Dakota, $1,505
Wyoming, $1,520
Alabama, $1,554
Most expensive non-profit hospitals/inpatient day:
Idaho, $4,208
California, $3,800
Oregon, $3,546
Washington, $3,500
Colorado, $3,319
Least expensive non-profit hospitals/inpatient day:
Mississippi, $1,365
South Dakota, $1,519
Iowa, $1,564
Montana, $1,627
Alabama, $1,723
Most expensive for-profit hospitals/inpatient day:
North Dakota, $4,701
South Dakota, $3,956
Alaska, $3,280
Nebraska, $3,031
Wisconsin, $2,830
Least expensive for-profit hospitals/inpatient day:
Maine, $1,055
Maryland, $1,207
West Virginia, $1,362
Iowa, $1,558
Arkansas, $1,619
Most expensive state/local government hospitals/inpatient
day:
Oregon, $4,062
Connecticut, $3,979
Washington, $3,312
California, $3,217
Utah, $3,038
Least expensive state/local government hospitals/inpatient
day:
Montana, $52
South Dakota, $442
Pennsylvania, $787
Nebraska, $906
Georgia, $917
Some Regions Pay Much
More for Healthcare
The KFF report did not look at whether patients in states
where hospitals incur the highest daily operating and non-operating expenses
also pay the most for hospital services. Hospital charges vary widely, with
many treatments costing far more in some regions than others.
In addition, health bills can vary at different hospitals in
the same city or region. According to Healthcare.gov,
the average total cost of a three-day hospital stay is about $30,000.
Adding to the confusion is the fact that hospital costs,
billed charges, and the amounts paid by patients for services can be distinctly
different amounts. Health insurance companies, for example, negotiate lower
rates with hospitals and health systems for their plan enrollees. While patients
without insurance are billed full price for services based on the hospital’s chargemaster.
Zack Cooper, PhD, Associate Professor of Health Policy and Economics at Yale University, told National Public Radio (NPR) that hospital consolidation is partly to blame for the wide variation in the price of hospital services within states and across the country. He says consolidation has eliminated competition in many markets. “Where one large hospital dominates the markets, that hospital is able to get higher prices,” Cooper maintains. “Hospitals have gotten increasingly powerful over time.” (Photo copyright: Yale University.)
CMS Final Rule
Requires Pricing Transparency
As of Jan. 1, 2019, a new Centers for Medicare and Medicaid Services (CMS) rule went into effect aimed at making hospital pricing more transparent. The CMS is now requiring hospitals to publish chargemaster price lists online, rather than release those numbers to patients upon request.
However, healthcare advocates have questioned the rule’s
impact on transparency. Posted hospital pricing information is often hard to
access and difficult to comprehend. In addition, chargemaster prices typically
do not represent the actual costs passed on to consumers.
“[The chargemaster] is the list price. When you go to buy a car, you have a manufacturer’s suggested retail price. This is basically what [the chargemaster] is,” Medical Contributor Natalie Azar, MD, told NBC News.
“Prevention comes first,” Nechrebecki suggests. “Utilize the
ambulatory care clinics. Go see your doctors and do what they recommend to keep
yourself healthy. Eat well and exercise often. You will prevent many surgeries
and hospitalizations.”
Sound advice. Nevertheless, clinical laboratories and anatomic pathology groups should take note of the federal government’s ongoing push for price transparency and prepare accordingly.