Family medicine academic departments in Canada are dealing with a shortage of applicants qualified for their residency programs, mirroring the shortage of pathologists
For the past decade, the number of medical residencies in Alberta Canada that went unfilled have increased each year. Now, just like in many parts of America, the province is experiencing severe medical staffing shortages that includes clinical laboratories and pathology groups.
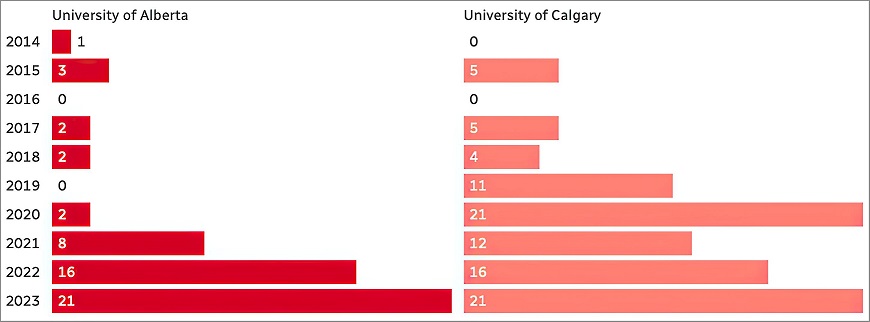
According to data compiled by the Canadian Resident Matching Service (CaRMS), after the first round of matching for post-graduate training spots as many as 12% of all spots went unfilled, especially in family medicine, the Canadian Broadcasting Corporation (CBC) reported.
Though the trend seems to be worse in Alberta, the resident shortage is affecting the entire Canadian healthcare system. According to the Angus Reid Institute, approximately half of all Canadians cannot find a doctor or get a timely appointment with their current doctor.
That is fueling predictions of an increased physician shortage in coming years, particularly in Alberta.
The graphic above taken from the CBC report shows how the number of residencies in family medicine that go unfilled has been increasing for the past 10 years. This trend mirrors similar trends affecting clinical laboratories and pathology groups around the world. (Graphic copyright: Canadian Broadcasting Corporation.)
Internationally Trained versus Home-grown Doctors
Canada’s current doctor shortage appears to be rooted in red tape that determines which MDs qualify for residency matching. According to John Paul Tasker, a senior journalist at the CBC, “there’s no shortage of doctors in Canada. What we have is a shortage of licensed doctors.” In his article, “Canada Is Short of Doctors—and It’s Turning Away Hundreds of Its Own Physicians Each Year,” Tasker notes that there may be as many as 13,000 medical doctors in Canada who are not currently practicing.
What’s standing in the way of Canadian doctors becoming licensed to practice? Some claim the system of residency matching is discriminatory towards Canadian doctors who received their training outside of Canada. Rosemary Pawliuk, President of the Society for Canadians Studying Medicine Abroad, is one of those who believe the system of matching is broken.
“They have cute slogans like, ‘You’re wanted and welcome in Canada,’ but when you look at the barriers, it’s very clear that you should not come home. Their message is essentially, ‘Go away’ and so [doctors] do,” Pawliuk told the CBC.
According the Pawliuk, “the current residency selection system puts internationally trained Canadian doctors at a serious disadvantage,” the CBC reported. “The Canadian public should be entitled to the best qualified Canadian applicant. Whether they’ve graduated from a Canadian school or an international school, whether they’re a Canadian by birth or if they’re an immigrant, they should be competing on individual merit,” she added.
Canada’s Medical School Matching Bias
In Canada’s current matching system, medical schools decide who gets a residency. Critics say the schools are biased towards Canadian-educated doctors and overlook foreign-trained doctors. About 90% of all residencies in Canada are set aside for Canadian-trained doctors and the remaining spots are left for the physicians trained abroad, CBC noted.
It is important to note that these doctors who are trained abroad are either Canadian citizens or permanent residents. Thus, it’s not a question of citizens from other countries competing with Canadian citizens.
So, if a surplus of doctors are being shut out of residency training opportunities, why are there open slots in Alberta? Some believe this indicates individuals are not interested in practicing medicine in Alberta.
But, Nathan Rider, MD, President of the Professional Association of the Resident Physicians of Alberta (PARA), claims he has not heard of residents turning down Alberta. He notes that the factors of where a resident may want to go geographically often depend on factors such as proximity to loved ones, cost of living, and program culture.
But Rinaldi still has concerns, “We may fill them with 42 disinterested people who have no interest in family medicine,” she says.
Anderson admits that “Across the country, over the last five or more years, family medicine has become less popular with medical students graduating from medical schools than it was in the years before.”
Therefore, both Anderson’s and Hemmelgarn’s schools have changed curriculum to put more of an emphasis on family medicine. Perhaps with these changes, and possibly an opening for internationally-trained Canadian doctors to achieve residency positions, Alberta’s—indeed all of Canada’s—residency match days will be better attended.
In the United States, there is little news coverage about serious problems with the health systems in other nations. The experience of residency programs in Canada, as explained above, demonstrates how a different national health system has unique issues that are not identical to issues in the US healthcare system. What is true is that Canada is dealing with a similar shortage of skilled medical technologists (MTs) and clinical laboratory scientists (CLSs), just like here in the United States.
By training a computer to analyze blood samples, and then automating the expert assessment process, the AI processed months’ worth of blood samples in a single day
New technologies and techniques for acquiring and transporting biological samples for clinical laboratory testing receive much attention. But what of the quality of the samples themselves? Blood products are expensive, as hospital medical laboratories that manage blood banks know all too well. Thus, any improvement to how labs store blood products and confidently determine their viability for transfusion is useful.
One such improvement is coming out of Canada. Researchers at the University of Alberta (U of A) in collaboration with scientists and academic institutions in five countries are looking into ways artificial intelligence (AI) and deep learning can be used to efficiently and quickly analyze red blood cells (RBCs). The results of the study may alter the way donated blood is evaluated and selected for transfusion to patients, according to an article in Folio, a U of A publication, titled, “AI Could Lead to Faster, Better Analysis of Donated Blood, Study Shows.”
Improving Blood Diagnostics through Precision Medicine and Deep Learning
“This project is an excellent example of how we are using our world-class expertise in precision health to contribute to the interdisciplinary work required to make fundamental changes in blood diagnostics,” said Jason Acker, PhD, a senior scientist at Canadian Blood Services’ Centre for Innovation, Professor of Laboratory Medicine and Pathology at the University of Alberta, and one of the lead authors of the study, in the Folio article.
The research took more than three years to complete and involved 19 experts from 12 academic institutions and blood collection facilities located in Canada, Germany, Switzerland, the United Kingdom, and the US.
“Our study shows that artificial intelligence gives us better information about the red blood cell morphology, which is the study of how these cells are shaped, much faster than human experts,” said Jason Acker, PhD (above), Senior Research Scientist, Canadian Blood Services, and Professor of Laboratory Medicine and Pathology at the University of Alberta, in an article published on the Canadian Blood Services website. “We anticipate this technology will improve diagnostics for clinicians as well as quality assurance for blood operators such as Canadian Blood Services in the coming years,” he added. Clinical laboratories in the US may also benefit from this new blood viability process. (Photo copyright: University of Alberta.)
To perform the study, the scientists first collected and manually categorized 52,000 red blood cell images. Those images were then used to train an algorithm that mimics the way a human mind works. The computer system was next tasked with analyzing the shape of RBCs for quality purposes.
Removing Human Bias from RBC Classification
“I was happy to collaborate with a group of people with diverse backgrounds and expertise,” said Tracey Turner, a senior research assistant in Acker’s laboratory and one of the authors of the study, in a Canadian Blood Services (CBS) article. “Annotating and reviewing over 52,000 images took a long time, however, it allowed me to see firsthand how much bias there is in manual classification of cell shape by humans and the benefit machine classification could bring.”
According to the CBS article, a red blood cell lasts about 115 days in the human body and the shape of the RBC reveals its age. Newer, healthier RBCs are shaped like discs with smooth edges. As they age, those edges become jagged and the cell eventually transforms into a sphere and loses the ability to perform its duty of transporting oxygen throughout the body.
Blood donations are processed, packed, and stored for later use. Once outside the body, the RBCs begin to change their shape and deteriorate. RBCs can only be stored for a maximum of 42 days before they lose the ability to function properly when transfused into a patient.
Scientists routinely examine the shape of RBCs to assess the quality of the cell units for transfusion to patients and, in some cases, diagnose and assess individuals with certain disorders and diseases. Typically, microscope examinations of red blood cells are performed by experts in medical laboratories to determine the quality of the stored blood. The RBCs are classified by shape and then assigned a morphology index score. This can be a complex, time-consuming, and laborious process.
“One of the amazing things about machine learning is that it allows us to see relationships we wouldn’t otherwise be able to see,” Acker said. “We categorize the cells into the buckets we’ve identified, but when we categorize, we take away information.”
Human analysis, apparently, is subjective and different professionals can arrive at different results after examining the same blood samples.
“Machines are naive of bias, and AI reveals some characteristics we wouldn’t have identified and is able to place red blood cells on a more nuanced spectrum of change in shape,” Acker explained.
The researchers discovered that the AI could accurately analyze and categorize the quality of the red blood cells. This ability to perform RBC morphology assessment could have critical implications for transfusion medicine.
“The computer actually did a better job than we could, and it was able to pick up subtle differences in a way that we can’t as humans,” Acker said.
“It’s not surprising that the red cells don’t just go from one shape to another. This computer showed that there’s actually a gradual progression of shape in samples from blood products, and it’s able to better classify these changes,” he added. “It radically changes the speed at which we can make these assessments of blood product quality.”
More Precision Matching Blood Donors to Recipients
According to the World Health Organization (WHO), approximately 118.5 million blood donations are collected globally each year. There is a considerable contrast in the level of access to blood products between high- and low-income nations, which makes accurate assessment of stored blood even more critical. About 40% of all blood donations are collected in high-income countries that home to only about 16% of the world’s population.
More studies and clinical trials will be necessary to determine if U of A’s approach to using AI to assess the quality of RBCs can safely transfer to clinical use. But these early results promise much in future precision medicine treatments.
“What this research is leading us to is the fact that we have the ability to be much more precise in how we match blood donors and recipients based on specific characteristics of blood cells,” Acker stated. “Through this study we have developed machine learning tools that are going to help inform how this change in clinical practice evolves.”
The AI tools being developed at the U of A could ultimately benefit patients as well as blood collection centers, and at hospitals where clinical laboratories typically manage the blood banking services, by making the process of matching transfusion recipients to donors more precise and ultimately safer.
University of Alberta researchers developed CIDER-Seq tool and protocols for the study, which they have made freely available to all scientists
Here’s another promising new technology which, given more research into effectiveness and safety, may soon lead to improved clinical laboratory cancer diagnostics. Oncology research scientists have focused much attention on understanding the role of extrachromosomal circular DNA (eccDNA) in human cancer. Now, a new gene sequencing method may help expand their knowledge about that and other circular DNA found in the genomes of bacteria, viruses, and other cells.
University of Alberta (UA) researchers have invented a new way for sequencing circular DNA, according to a recent study published in the journal Nature Protocols. As with any new technological method, this new tool—called CIDER-Seq—will need to be time-tested, but it does hold promise for providing valuable insights into the role these “mysterious loops” play not only in human disease, but in agricultural viruses as well.
A New Tool for Understanding DNA
DNA is considered “circular” when it has a closed loop with no ends. It differs from “linear” DNA chromosomes found in human cell nuclei. Circular DNA include:
Devang Mehta, PhD (above), Postdoctoral Fellow in the University of Alberta’s Department of Biological Sciences, and lead author of the UA study, describes the breakthrough in his team’s on-going work researching the role of eccDNA molecules. “We devised a new molecular biology method and a new bioinformatics algorithm to finally obtain full-length sequences of eccDNA,” he said in a news release. “Our method finally allows us to sequence these molecules completely and gives us and other researchers a tool to better understand what they actually do in the cell.” (Photo copyright: ecrLife.)
According to the UA study, circular DNA enrichment sequencing (CIDER-Seq) “is a technique to enrich and accurately sequence circular DNA without the need for polymerase chain reaction amplification, cloning, and computational sequence assembly.”
CIDER-Seq uses DNA sequencing technology from Pacific Biosciences, Inc. (PacBio) of Menlo Park, Calif. PacBio (NASDAQ:PACB) is an American biotechnology company founded in 2004 that develops and manufactures gene sequencing systems.
Understanding Circular DNA in Any Human or Plant Cell, Including Cancer
Because many viruses that infect crops have circular DNA, Mehta believes the new tool may be particularly helpful to agricultural scientists. His team of researchers, he noted in the UA news release, used an earlier version of CIDER-Seq to study crop plants in Kenya which were genetically engineered to resist circular DNA viruses.
“Our key advance is that, through our method, scientists can finally gain an unbiased, high-resolution understanding of circular DNA in any type of cell. With our invention of CIDER-Seq, we can start to begin to understand the function of these mysterious circular DNAs in human and plant cells,” Mehta said.
However, this technological advance may be equally welcomed by researchers investigating the role of eccDNA in human cancer. Though both healthy and diseased cells may contain circular DNA, the New York Times noted that the “mysterious loops” are “surprisingly common in cancer cells and play a bigger role in many types of cancers than was previously recognized.” The article goes on to state that until now there have not been effective methods for sequencing circular DNA.
In Clinical Chemistry, a panel of eccDNA experts discussed the critical role circular DNA plays in cancer, referred to as extrachromosomal DNA (ecDNA). “Importantly, in cancer cells, ecDNAs seem to be more transcriptionally active than their chromosomal counterparts and have been suspected to confer growth and survival advantage to cancer cells,” the article states.
According to the New York Times, scientists first discovered the existence of circular DNA in the 1960s when “little clumps of DNA” were detected alongside chromosomes. Today, researchers believe circular DNA is more common in the human genome than first realized and could be linked to a variety of conditions and diseases, not solely to cancer.
CIDER-Seq Research May Lead to New Clinical Laboratory Biomarkers
Birgitte Regenberg, PhD, Associate Professor in Ecology and Evolution at the University of Copenhagen, pioneered methods for detecting circular DNA. She told the New York Times, “I think we’re just opening our eyes up.”
Though she says the research has been “cancer-centered,” Regenberg maintains the role circular DNA plays in human biology may prove to be much broader.
“It’s like when a horse has blinders: The blinders focus the science, but they also prevent some things from being understood,” she said.
Clinical laboratory leaders should keep an eye on the use of CIDER-Seq technology. It may lead to the development of new biomarkers for cancer and other diseases.
As standard masks are used they collect exhaled airborne pathogens that remain living in the masks’ fibers, rendering them infectious when handled
Surgical-style facial masks harbor a secret—viruses that could be infectious to the people wearing them. However, masks can become effective virus killers as well. At least that’s what researchers at the University of Alberta (UAlberta) in Edmonton, Canada, have concluded.
If true, such a re-engineered mask could protect clinical laboratory workers from exposure to infectious diseases, such as, SARS (Severe Acute Respiratory Syndrome), MERS (Middle East Respiratory Syndrome), and Swine Influenza.
“Surgical masks were originally designed to protect the wearer from infectious droplets in clinical settings, but it doesn’t help much to prevent the spread of respiratory diseases such as SARS or MERS or influenza,” Hyo-Jick Choi, PhD, Assistant Professor in UAlberta’s Department of Chemical and Materials Engineering, noted in a press release.
So, Choi developed a mask that effectively traps and kills airborne viruses.
Clinical Laboratory Technicians at Risk from Deadly Infectious Diseases
The global outbreak of SARS in 2003 is a jarring reminder of how infectious diseases impact clinical laboratories, healthcare workers, and patients. To prevent spreading the disease, Canadian-based physicians visited with patients in hotel rooms to keep the virus from reaching their medical offices, medical laboratory couriers were turned away from many doctors’ offices, and hospitals in Toronto ceased elective surgery and non-urgent services, reported The Dark Report—Dark Daily’s sister publication. (See The Dark Report, “SARS Challenges Met with New Technology,” April 14, 2003.)
UAlberta materials engineering professor Hyo-Jick Choi, PhD, (right) and graduate student Ilaria Rubino (left) examine filters treated with a salt solution that kills viruses. Choi and his research team have devised a way to improve the filters in surgical masks, so they can trap and kill airborne pathogens. Clinical laboratory workers will especially benefit from this protection. (Photo and caption copyright: University of Alberta.)
How Current Masks Spread Disease
How do current masks spread infectious disease? According to UAlberta researchers:
A cough or a sneeze transmits airborne pathogens such as influenza in aerosolized droplets;
Virus-laden droplets can be trapped by the mask;
The virus remains infectious and trapped in the mask; and,
Risk of spreading the infection persists as the mask is worn and handled.
“Aerosolized pathogens are a leading cause of respiratory infection and transmission. Currently used protective measures pose potential risk of primary and secondary infection and transmission,” the researchers noted in their paper, published in Scientific Reports.
That’s because today’s loose-fitting masks were designed primarily to protect healthcare workers against large respiratory particles and droplets. They were not designed to protect against infectious aerosolized particles, according to the Centers for Disease Control and Prevention (CDC).
In fact, the CDC informed the public that masks they wore during 2009’s H1N1 influenza virus outbreak provided no assurance of infection protection.
“Face masks help stop droplets from being spread by the person wearing them. They also keep splashes or sprays from reaching the mouth and nose of the person wearing the face mask. They are not designed to protect against breathing in very small particle aerosols that may contain viruses,” a CDC statement noted.
Pass the Salt: A New Mask to Kill Viruses
Choi and his team took on the challenge of transforming the filters found on many common protective masks. They applied a coating of salt that, upon exposure to virus aerosols, recrystallizes and destroys pathogens, Engineering360 reported.
“Here we report the development of a universal, reusable virus deactivation system by functionalization of the main fibrous filtration unit of surgical mask with sodium chloride salt,” the researchers penned in Scientific Reports.
The researchers exposed their altered mask to the influenza virus. It proved effective at higher filtration compared to conventional masks, explained Contagion Live. In addition, viruses that came into contact with the salt-coated fibers had more rapid infectivity loss than untreated masks.
How Does it Work?
Here’s how the masks work, according to the researchers:
Aerosol droplets carrying the influenza virus contact the treated filter;
The droplet absorbs salt on the filter;
The virus is exposed to increasing concentration of salt; and,
The virus is damaged when salt crystallizes.
“Salt-coated filters proved highly effective in deactivating influenza viruses regardless of [influenza] subtypes,” the researchers wrote in Scientific Reports. “We believe that [a] salt-recrystallization-based virus deactivation system can contribute to global health by providing a more reliable means of preventing transmission and infection of pandemic or epidemic diseases and bioterrorism.”
Other Reports on Dangerous Exposure for Clinical Laboratory Workers
This is not the first time Dark Daily has reported on dangers to clinical laboratory technicians and ways to keep them safe.
In “Health of Pathology Laboratory Technicians at Risk from Common Solvents like Xylene and Toluene,” we reported on a 2011 study that determined medical laboratory technicians who handle common solvents were at greater risk of developing auto-immune connective tissue diseases.
The UAlberta team may have come up with an inexpensive, simple, and effective way to protect healthcare workers and clinical laboratory technicians. Phlebotomists, laboratory couriers, and medical technologists also could wear the masks as protection from accidental infection and contact with specimens. It will be interesting to follow the progress of this special mask with its salty filter.