This is the third of a three-part series on revenue cycle management for molecular testing laboratories and pathology practices, produced in collaboration with XiFin Inc.
Automation and AI-Powered Workflow Paves the Way for Consistent, Optimized Molecular Diagnostics and Pathology RCM
Third in a three-part series, this article will discuss how sophisticated revenue cycle management technology, including artificial intelligence (AI) capabilities, drives faster, more efficient revenue reimbursement for molecular and pathology testing.
Financial and operational leaders of molecular testing laboratories and pathology groups are under pressure to maximize the revenue collected from their services rendered. This is no easy task. Molecular claims, in particular, can be especially complex. This article outlines the specific areas in which automation and artificial intelligence (AI)-based workflows can improve revenue cycle management (RCM) for molecular diagnostic and pathology organizations so they can better meet their operational and financial goals.
AI can play a number of important roles in business. When it comes to RCM for diagnostic organizations, first and foremost, AI can inform decision-making processes by generating new or derived data, which can be used in reporting and analytics. It can also help understand likely outcomes based on historical data, such as an organization’s current outstanding accounts receivable (AR) and what’s likely to happen with that AR based on historic performance.
AI is also deployed to accelerate the creation of configurations and workflows. For example, generated or derived data can be used to create configurations within a revenue cycle workflow to address changes or shifts in likely outcomes, such as denial rates. Suppose an organization is using AI to analyze historical denial data and predict denial rates. In that case, changes in those predicted denial rates can be used to modify a workflow to prevent those denials upfront or to automate appeals on the backend. This helps organizations adapt to changes more quickly and accelerates the time to reimbursement.
“Furthermore, AI is used to automate workflows by providing or informing decisions directly,“ says Clarisa Blattner, XiFin Senior Director of Revenue and Payor Optimization. “In this case, when the AI sees shifts or changes, it knows what to do to address them. This enables an organization to take a process in the revenue cycle workflow that is very human-oriented and automate it.”
AI is also leveraged to validate data and identify outcomes that are anomalous, or that lie outside of the norm. This helps an organization:
Ensure that the results achieved meet the expected performance
Understand whether the appropriate configurations are in place
Identify if an investigation is required to uncover the reason behind any anomalies so that they can be addressed
Finally, AI can be employed to generate content, such as letters or customer support materials.
Everything AI starts with data
Everything AI-related starts with the data. Without good-quality data, organizations can’t generate AI models that will move a business forward. In order to build effective AI models, an organization must understand the data landscape and be able to monitor and measure performance and progress and adjust the activities being driven, as necessary.
Dirty, unstructured data leads to unintelligent AI. AI embodies the old adage, “garbage in, garbage out.” The quality of the AI decision or prediction is entirely based on the historical data that it’s seen. If that data is faulty, flawed, or incomplete, it can lead to bad decisions or the inability to predict or make a decision at all. Purposeful data modeling is critical to AI success, and having people and processes that can understand the complicated RCM data and structure it so it can be effectively analyzed is vital to success.
The next step is automation. Having effective AI models that generate strong predictions is only as valuable as the ability to get that feedback into the revenue cycle system effectively. If not, that value is minimal, because the organization must expend a lot of human energy to try to reconfigure or act on the AI predictions being generated.
There is a typical transformation path, illustrated below, that organizations go through to get from having data stored in individual silos to fully embedded AI. If an organization is struggling with aggregating data to build AI models, it’s at stage one. The goal is stage five, where an organization uses AI as a key differentiator and AI is a currency, driving activity.
The transformation starts with structuring data with an underlying data approach that keeps it future-ready. It is this foundation that allows organizations to realize the benefits of AI in a cost-effective and efficient way. Getting the automation embedded in the workflow is the key to getting to the full potential of AI in improving the RCM process.
Real-world examples of how AI and automation improve RCM
One example of how AI can improve the RCM process is using AI to discover complex payer information. One significant challenge for diagnostic service providers is ensuring that the right third-party insurance information for patients is captured. This is essential for clean claims submission. Often, the diagnostic provider is not the organization that actually sees the patient, in which case it doesn’t have the ability to collect that information directly. The organization must rely on the referring physician or direct outreach to the patient for this data when it’s incorrect or incomplete.
Diagnostic providers are sensitive to not burdening referring clients or patients with requests for demographic or payer information. It’s important to make this experience as simple and smooth as possible. Also, insurance information is complicated. A lot of data must be collected or corrected if the diagnostic provider doesn’t have the correct information.
Automating this process is difficult. Frequently, understanding who the payer is and how that payer translates into contracts and mapping within the revenue cycle process requires an agent to be on the phone with the patient. It can be very difficult for a patient to get precise payer plan information from their insurance card without the help of a customer service representative.
This is where AI can help. The goal is to require the smallest amount of information from a patient and be able to verify eligibility through electronic means with the payer. Using optical character recognition (OCR), an organization can take an image of the front and back of a patient’s insurance card, isolate the relevant text, and use an AI model to get the information needed in order to generate an eligibility request and confirm eligibility with that payer.
In the event that taking an image of the insurance card is problematic for a patient, the organization can have the patient walk through a simplified online process, for example, through a patient portal, and provide just a few pieces of data to be able to run eligibility verification and get to confirmed eligibility with the payer.
AI can help with this process too. For example, the patient can provide high-level payer information only, such as the name of the commercial payer or whether the coverage is Medicare or Medicaid, the state the patient resides in, and the subscriber ID and AI can use this high-level data to get an eligibility response and confirmed eligibility.
Once the eligibility response is received, the more detailed payer information can be presented back to the patient for confirmation. AI can map the eligibility response to the appropriate contract or payer plan within the RCM system.
Now that the patient’s correct insurance information is captured, the workflow moves on to collecting the patient’s financial responsibility payment. To do that, the organization needs to be able to calculate the patient’s financial responsibility estimate. The RCM system has accurate pricing information and now has detailed payer and plan information, a real-time eligibility response, as well as test or procedure information. This data can be used to estimate patient financial responsibility.
AI can also be used to address and adapt to changes in ordering patterns, payer responses, and payer reimbursement behavior. The RCM process can be designed to incorporate AI to streamline claims, denials, and appeals management, as well as to assign work queues and prioritize exception processing (EP) work based on the likelihood of reimbursement, which improves efficiency.
One other way AI can help is in understanding and or maintaining “expect” prices—what an organization can expect to collect from particular payers for particular procedures. For contracted payers, contracted rates are loaded into the RCM system. It’s important to track whether payers are paying those contracted rates and whether the organization is receiving the level of reimbursement expected. For non-contracted payers, it’s harder to know what the reimbursement rate will be. Historical data and AI can provide a good understanding of what can be expected. AI can also be used to determine if a claim is likely to be rejected because of incorrect or incomplete payer information or patient ineligibility, in which case automation can be applied to resolve most issues.
Another AI benefit relates to quickly determining the probability of reimbursement and assigning how claims are prioritized if a claim requires intervention that cannot be automated. With AI, these claims that require EP are directed to the best available team member, based on that particular team member’s past success with resolving a particular error type.
The goal with EP is to ensure that the claims are prioritized to optimize reimbursement. This starts with understanding the probability of the claim being reimbursed. An AI model can be designed to assess the likelihood of the claim being reimbursed and the likely amount of reimbursement for those expected to be paid. This helps prioritize activities and optimize labor resources. The AI model can also take important factors such as timely filing dates into account. If a claim is less likely to be collected than another procedure but is close to its timely filing deadline, it can be escalated. The algorithms can be run nightly to produce a prioritized list of claims with assignments to the specific team member best suited to address each error.
AI can also be used to create a comprehensive list of activities and the order in which those activities should be performed to optimize reimbursement. The result is a prioritized list for each team member indicating which claims should be worked on first and which specific activities need to be accomplished for each claim.
Summing it all up, organizations need an RCM partner with a solid foundation in data and data modeling. This is essential to being able to effectively harness the power of AI. In addition, the RCM partner must offer the supporting infrastructure to interface with referring clients, patients, and payers. This is necessary to maximize automation and smoothly coordinate RCM activities across the various stakeholders in the process.
Having good AI and insight into data and trends is important, but the ability to add automation to the RCM process based on the AI really solidifies the benefits and delivers a return on investment (ROI). Analytics are also essential for measuring and tracking performance over time and identifying opportunities for further improvement.
Diagnostic executives looking to maximize reimbursement and keep the cost of collection low will want to explore how to better leverage data, AI, automation, and analytics across their RCM process.
This is the third of a three-part series on revenue cycle management for molecular testing laboratories and pathology practices, produced in collaboration with XiFin Inc. Missed the first two articles? www.darkdaily.com
Potentially increasing the revenue write-off burden for clinical laboratories, HRSA changes, insurance contracting, policy and coverage questions for genetic and genomic testing, and patient relationship disconnects will expose cracks in lab test claim generation and billing processes
Last year it was estimated that collection agencies held $140 billion in unpaid medical bills, in addition to the amount of unpaid bills in pre-collection status, according to a New York Times report. More recently, the American Hospital Association showed that hospitals have provided upwards of $700 billion in uncompensated care since 2000, with over $40 billion in 2019 alone.
Because strategies to collect the unpaid can be complicated and time-consuming, many healthcare organizations, including clinical laboratories, choose to write off these uncollectible bills. Dark Daily and The Dark Report have covered clinical laboratory revenue challenges for many years. In considering the paths forward, software-as-a-service (SaaS) provider FrontRunner Healthcare (FrontRunnerHC) recently provided snapshots into the how and where of improved collections.
Fixing Data Issues that Lead to Forfeited Clinical Laboratory Revenue
The underpinnings of unpaid lab tests are many. In a recent interview with Dark Daily, FrontRunnerHC CEO and Founder John (JD) Donnelly estimated that about one-third of claims (prior to submission) include incorrect or missing patient information, such as insurance policy identification or demographics. These gaps undermine an organization’s ability to get paid. Donnelly estimates that bad-debt write-offs for commercial payer claims average over 15% of charges. To address these challenges, the company’s clean claims SaaS provides “instantaneous” patient insurance, demographic, and financial information.
Whether lower-dollar accessions such as routine testing, or the higher-dollar accessions of genetic tests, uncollected payments add up. Donnelly said that, in 2021, almost one-third of the company’s clients uncovered revenue ranging from $1 million to over $90 million using the software. Donnelly also estimated that the return for clients averages eight times the value of the investment in using the automated solution.
In one example, Sonora Quest, a joint venture between Banner Health and Quest Diagnostics, reported a 10-15% decline in write-offs due to aged claims, a savings of over $1million annually, as published in a case study. “As an aside, in a presentation at the Executive War College last November, they also attributed improvements in patient satisfaction measures to the software, including a 65% decrease in abandoned calls, 28% improvement in their call service factor, and 19% decrease in patient call volumes,” stated Donnelly.
Questions About Cost of Care Likely Cause Stress for Patients
As many know, nonpay issues are problematic not only for lab businesses and anatomic pathology practices but also for patients and their families who have little predictability with their cost of care in the midst of stressful health events. “From the time a patient is registered to the time the claim is paid, there are more challenges than people realize that jeopardize the patient’s experience as well as the provider’s ability to get reimbursed,” Donnelly explained. Medical laboratory administrators have struggled to respond, often by using traditional manual methods such as call centers, or more recently by considering the use of data automation tools.
From the patient payment perspective, Donnelly said, a good strategy is having the ability, on demand, to understand each patient’s specific financial situation and likelihood to pay. For example, using FrontRunnerHC’s software to gauge patients’ propensity to pay and determine financial disposition strategies, lab administrators may choose to offer payment plans or hardship discounts to those falling under the federal poverty level (FPL). Or they may choose to send a collection agency only the past-due accounts for patients who have a low likelihood to pay rather than sending them all past due accounts and focus in-house efforts on the others. One genetics lab client who recently started leveraging these software capabilities “is already seeing more than 5% in incremental net collections,” according to Donnelly.
Further, an estimated 2 million people switch insurance plans each month, reported Axios. “That velocity of change is tough for providers to manage, but it’s critical as insurance eligibility and registration issues are the number one reason for claims denials,” Donnelly said.
For a sense of the magnitude of the problem, “Between 25 and 33 cents of every dollar you spend on medical care pays for health care’s back office,” wrote Dana Miller Ervin in September 2021 for a series of investigations called “The Price We Pay,” published at WFAE 90.7 news in Charlotte, North Carolina. “Every medical provider and laboratory in the country has to negotiate with insurance companies. And since there are 900 health insurers, 6,000 hospitals and more than 100,000 physician practices—many of which are independent of larger systems—there are hundreds of thousands of negotiations.”
New Clinical Laboratory Business Challenges Making News Now
All these issues affecting revenue cycle management (RCM) for independent clinical laboratories, hospital and health system laboratories, and physician office laboratories could be compounded by three emerging issues.
Donnelly said that many lab clients have yet to be reimbursed for COVID tests they have performed, despite their HRSA-required due diligence prior to submitting the claims before the deadline. To avoid additional reimbursement risk, many labs have made the decision to stop testing the uninsured or charge them for it, ABC News reported in late March. As of early April, however, Congress was in discussions to re-fund at least some of the Uninsured Program, reported Politico.
Secondly, and also daunting, are the questions surrounding payer coverage and reimbursement for genetic tests and genomic testing. Thanks to high-deductible health plans (HDHPs), clinical laboratories and anatomic pathology groups increasingly must collect deductibles that may be the full amount of the test – and directly from patients rather than from insurance companies. Therefore, there is more demand from patients to understand their expected cost before the test, Donnelly added.
Problems can arise, for both labs and patients, if they don’t know whether a test has been preauthorized for medical necessity or if they lack accurate insurance information such as in-network or out-of-network. “Getting all the needed and accurate info upfront prior to it going into the LIS [Laboratory Information System] can be a reimbursement game changer,” stated Donnelly.
“For a high complexity, high-throughput diagnostic lab, an efficient workflow is critical,” stated Kyle Koeppler, President of nuCARE Medical Solutions Inc., a FrontRunnerHC client. “Capturing the correct patient demographics and insurance information at patient intake increases the accuracy of every order and makes every process involving patient information much more efficient,” Koeppler shared. “It’s simply too costly to risk having inaccurate information at intake.”
And lest we forget, the Protecting Access to Medicare Act (PAMA) is looming with its reimbursement cuts planned through 2026, and requirements of many labs to report private payer rates on a test-by-test basis. While delayed again, the 2023 PAMA reporting requirements and payment cuts must not be ignored, and planning is needed in order to ensure appropriate reimbursement, Donnelly added.
Addressing Long Payment Cycles for Claims, Dead Ends, and Decreased Collection Rates
The CAQH report cites that data automation resulted in efficiency savings of $122 billion annually for the US healthcare system in 2020 yet “meaningful opportunities for additional savings remain.”
Data automation can reduce the burden of labor-intensive functions in coding, billing, filing appeals, and collecting from payers and patients and, therefore, reduce overall RCM costs. The Council for Affordable Quality Healthcare’s (CAQH) 2020 Index reported, “Considering the millions of times these transactions occur every day, the savings potential across the healthcare economy [from streamlining administrative processes] is significant.”
“One way to avoid potential write-offs is by reworking a claim, but the rework is often left undone,” stated John (JD) Donnelly (above), CEO and Founder of FrontRunnerHC. “The better way to avoid a potential write-off is to ensure you’ve got a clean claim in the first place.” (Photo copyright: FrontRunnerHC.)
The intended outcome is an increase in the total amount of revenue collected from the same number of claims.
To that end, FrontRunnerHC’s software links critical data within its partner ecosystem. This ecosystem includes the well-established credit reporting agencies as well as data available through connected healthcare payers and providers equipped with electronic data interchange (EDI) capabilities. “While an employee may be able to manually work about six accessions in an hour, clients can process approximately 40,000 patients in an hour through software automation, leaving staff to work on more value-added initiatives,” stated Donnelly.
Ideally, missing and inaccurate patient information or insurance verification, which are crucial for producing prompt payments and clean claims, should be corrected before a specimen is collected, Donnelly said. However, if the laboratory is nursing aging accounts receivable (AR), Donnelly advises an audit and cleanup of the AR backlog as a first step to quickly fix information errors and reduce write-offs. “In your AR bucket of $10 million, you may have $3 million that’s collectible or $9.8 million that’s collectible. By leveraging software to clean up what can be collected, clients can go after the money they deserve.”
Improve Collections Through Data Automation While Assisting in the Patient Financial Journey
With the rise of telehealth/telemedicine, healthcare consumerism, and care delivered to nontraditional sites, it makes sense that the idea of the clinical laboratory as a silent partner in healthcare could be changing.
“Could we one day see patients asked for not only their preferred pharmacy but their preferred clinical laboratory as well?” Donnelly pondered and added, “I think the answer is yes, and it’s sooner than many think.”
Understanding the patient’s experience is a key step in providing patient-centered care. Therefore, patient experience programs that originate at clinical laboratories where specimens are processed, but before specimens have been collected, could make these labs more visible in their markets and enable them to capitalize on the advantages of data automation to sustainably improve revenue cycle management.
“The patient’s financial journey which runs in parallel to their clinical journey can get pretty bumpy, and those bumps impact their overall experience as well as the provider’s bottom line,” added Donnelly. “Getting accurate patient information upfront and catching any changes to the information as needed throughout the process helps clients create a smoother patient journey by enabling them to quickly manage through the bumps or eliminate them altogether.”
—Liz Carey
This article was produced in collaboration with FrontRunnerHC.
Because of ‘shelter in place’ orders, many anatomic pathologists are reviewing digital images from home during the COVID-19 outbreak and demonstrating the value of whole slide imaging, digital pathology, and CMS’ recent amended remote sign-out policy
COVID-19 is already triggering many permanent changes in the way healthcare is organized and delivered in the United States. However, not until the SARS-CoV-2 pandemic eases will the full extent of these changes become visible. This will be particularly true for anatomic pathology and the profession’s expanded use of telepathology, digital pathology, and whole-slide imaging.
Since early March, specimen referrals and revenues have collapsed at anatomic pathology groups and laboratories across the nation. Dark Daily’s sister publication, The Dark Report (TDR), was first to quantify the magnitude of this collapse in tissue referrals to pathology groups. In an interview with The Dark Report, Kyle Fetter, Executive Vice President and General Manager of Diagnostic Services at XIFIN, Inc., explained that pathology clients using XIFIN’s revenue cycle management services were seeing an average 40% decrease in specimens. And, for certain pathology sub-specialties, the drop-off in specimen referrals was as much as 90%. (See TDR, “From Mid-March, Labs Saw Big Drop in Revenue,” April 20, 2020.)
The College of American Pathologists (CAP) appealed to the Centers for Medicare and Medicaid Services (CMS) to allow pathologists to work remotely. In response, CMS issued a memorandum which stated, “Due to the public health emergency posed by COVID-19 and the urgent need to expand laboratory capacity, CMS is exercising its enforcement discretion to adopt a temporary policy of relaxed enforcement in connection with laboratories located at temporary testing sites under the conditions outlined herein.”
Since then, many physicians, including pathologists, have quickly adapted to working remotely in some form.
Push for Remote Pathology Services Acknowledges Anatomic Pathologist Shortage
The CMS memorandum (QSO-20-21-CLIA), which the federal agency issued to laboratory surveyors on March 26, 2020, notes that CMS will exercise “enforcement discretion to ensure pathologists may review pathology slides remotely” if certain defined conditions are met.
CMS’ decision, which “is applicable only during the COVID-19 public health emergency,” is intended to increase capacity by allowing remote site review of clinical laboratory data, results, and pathology slides.
Ordinarily, CLIA regulations for cytology (a branch of study that focuses on the biological structure of cells) state that cytology slide preparations must be evaluated on the premises of a laboratory that is certified to conduct testing in the subspecialty of cytology. However, a fast-acting Congressional letter sent by 37 members of Congress to US Department of Health and Human Services (HHS) Secretary Alex Azar II, MD, states, “it is unwise and unnecessary to overburden the remaining pathologists with excess work due to staffing shortages, thereby increasing the risk of burnout, medical error, and further shortages in staffing due to exposure. The number of COVID-19 cases will increase and peak over the next two months and will stretch existing healthcare systems to their limits.”
Decreasing Number of ‘Active Pathologists’ Drives Adoption of Telepathology, Digital Pathology, and Whole-slide Imaging
The current COVID-19 outbreak is just the latest factor in support of enabling remote review of anatomic pathology images and cases. The trend of using telepathology, whole-slide imaging (WSI), and digital pathology systems has been gathering momentum for several years. Powerful economic forces support this trend.
The Dark Report devoted its June 10, 2019, issue to a deep dive of the challenges currently facing the anatomic pathology profession. In particular, TDR noted a study published May 31, 2019, in the Journal of the American Medical Association (JAMA) Network Open, titled, “Trends in the US and Canadian Pathologist Workforces from 2007 to 2017.” The study’s authors—pathologists in the United States and Canada—reported that between 2007 and 2017 the number of active pathologists in the United States decreased from 15,568 to 12,839—a 17.53% decline.
TDR noted that these findings imply there are fewer pathologists in the United States today in active practice to handle the steady increase in the number of cases requiring diagnostic review. In turn, this situation could lead to delays in diagnoses detrimental to patient care.
In the United States, the COVID-19 pandemic created an “immediate need for remote sign-outs, reviews, and consults,” said Mike Bonham, MD, PhD (above), Chief Medical Officer for Proscia, a digital pathology software developer, in an interview with Dark Daily. “In the context of highly relevant workflow and workforce challenges, it reinforces the opportunity for wider adoption of digital pathology.” Prior to the outbreak of COVID-19, several distinct forces were driving adoption and use of digital pathology in combination with traditional microscopy, he said. (Photo copyright: Proscia.)
Distinct Forces Beginning to Reshape Anatomic Pathology
In recent years, the anatomic pathology profession has faced growing financial pressure, a shrinking workforce, and a surge in the global demand for pathology—issues that come at a time when biopsies and cancer diagnostics require greater expertise.
The UCSF School of Medicine started with frozen slide sections and moved to the broader volume of pathology slides. Since 2015, UCSF’s School of Medicine has moved toward a fully digital pathology operation and has serialized the adoption by specialty, according to Zoltan Laszik, MD, PhD, attending physician at UCSF and Professor of Clinical Pathology in UCSF’s Departments of Pathology and Laboratory Medicine.
Laszik is among a handful of specialists and digital pathology early adopters who collaborated on the new Dark Daily white paper, which is available for free download.
Through the adoption of digital pathology, glass slides are digitized using a whole-slide image scanner, then analyzed through image viewing software. Although the basic viewing functionality is not drastically different than that provided by a microscope, digitization does bring improvements in lab efficiency, diagnostic accuracy, image management, workflows, and revenue enhancements.
Additionally, artificial intelligence (AI)-based computational applications have emerged as an integral part of the digital pathology workflow in some settings, the white paper explains.
“These developments are important to anatomic pathologists because the traditional pathology business model continues to transform at a steady pace,” noted Robert L. Michel, Editor-in-Chief of The Dark Report.
Anthony Magliocco, MD, FRCPC, FCAP, President and CEO of Protean BioDiagnostics and former Professor and Chair of Pathology at Moffitt Cancer Center, is featured in the white paper as well. His new pathology service model provides routine pathology services, precision oncology, second opinions, liquid biopsies, genetics, and genomics to cancer centers from a Florida-based specialty laboratory.
To register for this important learning opportunity, click here or place this URL in your web browser: https://www.darkdaily.com/webinar/streamlined-operations-increased-revenue-higher-quality-of-care-conclusive-evidence-on-the-value-of-adopting-digital-pathology-in-your-lab/.
These digital pathology technologies represent an innovative movement shaping the present and future of pathology services. Pathologists wanting to learn more are encouraged to sign up for the May 13 webinar, which will build on the body of evidence and commentary that is included in the new white paper, and which will be available for free on-demand download following the live broadcast.
Consumer demand and federal requirements for price transparency affect how clinical laboratories and anatomic pathology groups meet patients’ expectations while navigating complex payer agreements
Regardless of a clinical laboratory’s payer mix and revenue cycle management (RCM) system, the demand for greater price transparency impacts laboratory services just as it does other healthcare services. Addressing new federal policies that support price transparency may require medical laboratory managers to alter how they approach RCM and patient communications.
Patient access management (PAM) is what some early-adopter medical labs and pathology groups are using to respond to these new federal policies and changing patient expectations. PAM can be an effective tool to fulfill complex payer requirements and implement consumer-friendly healthcare services. Not only does this comply with federal guidelines, it helps independent laboratories increase revenue by lowering denial rates.
How
and When Clinical Laboratories Should Implement Patient Access Management
Revenue
cycle experts say clinical laboratories are in a position to take an active
role in the pricing transparency debate.
“If labs don’t control the pricing narrative, someone else will,” stated Walt Williams, Director of Revenue Cycle Optimization and Strategy for Quadax, a firm that has studied revenue trends in healthcare for more than 40 years, in an exclusive interview with Dark Daily.
He
says, given these new demands on clinical laboratories and pathology groups,
implementing patient access management practices ensures a satisfactory patient
and physician experience and reduces the financial risk related to trends in
uncollected revenue.
“In this
age of increasing consumerism—along with the complex challenges of navigating
the payer landscape and pre-empting administrative denials—it’s no wonder
independent labs are turning to new patient access technology solutions to
avoid leaving money on the table,” Williams said.
Patient
access management solutions allow clinical laboratories to:
obtain
accurate patient demographic information,
verify
insurance coverage and eligibility, and
gain
clarity on payer rules regarding prior authorization and medical necessity.
These
capabilities enable medical laboratories to secure appropriate reimbursement
closer to the date of service. PAM also can provide the ordering-physician with
financial counseling and guidelines on a patient’s financial obligation. This
would be shared with the patient to help prevent surprise billing.
New
Fact of Life for Labs: Patients Are the New Payers
Medical laboratory patient-access representatives must employ proper patient-liability collection techniques before, during, and after each date of service. This has become increasingly challenging as more patients join high-deductible health plans (HDHPs) and take on more financial responsibility. The problem for labs is that meeting the expectations of consumers requires a different toolset than meeting the needs of complex payer requirements.
Additionally, evolving policies in prior authorization, medical necessity, and coding (see, “Labs Get High Denial Rates Under New NCCI Rules,” The Dark Report) are resulting in potential payment traps for patients and known revenue traps for providers and suppliers.
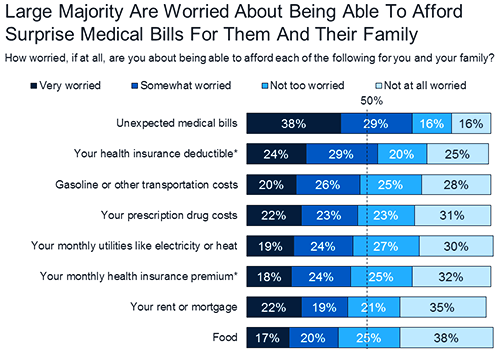
The graphic above, taken from a KFF Health Tracking Poll conducted in 2018, lists “unexpected medical bills” as the top financial fear among Americans. “Four in 10 (39%) insured adults ages 18-64 say there has been a time in the past 12 months when they received care from a doctor, hospital, or lab that they thought was covered and their health plan either didn’t cover the bill at all or covered less than they expected,” the KFF poll notes. This illustrates the critical importance for clinical laboratories to implement patient access management protocols. (Graphic copyright: Kaiser Family Foundation.)
While
the current high cost of healthcare will likely continue for some time,
publishing information about the lab’s policies can help consumers view choices
when it comes to selecting laboratory tests and anticipating potential payment
obligations.
Henry Ford Health System, for example, posted information about prior authorization as it relates to its pathology and laboratory services.
Consumer-Facing
Price Transparency and CMS Requirements
Rooted
in price transparency regulations issued in July 2018, the federal Centers for
Medicare and Medicaid Services (CMS) encouraged “all providers and suppliers of
healthcare services to undertake efforts to engage in consumer-friendly
communication of their charges to help patients understand what their potential
financial liability might be for services they obtain, and to enable patients
to compare charges for similar services. We encourage providers and suppliers
to update this information at least annually, or more often as appropriate, to
reflect current charges.”
How
should we define “standard charges” in provider and supplier settings? Is the
best measure of a provider’s or supplier’s standard charges its chargemaster,
price list, or charge list?
What
types of information would be most beneficial to patients … enable patients to
use charge and cost information in their decision-making?
How
can information on out-of-pocket costs be provided to better support patient
choice and decision-making? What can be done to better inform patients of their
financial obligations?
What
changes would need to be made by providers and suppliers to provide patients
with information on what Medicare pays for a particular service performed by
that provider or supplier?
These
considerations and more can help the development of patient access management
and consumer-friendly communication initiatives that are tailored to clinical laboratory
services.
Patient
Access Management for Clinical Laboratories
Patient
access management facilitates critical components of the revenue cycle.
However, it must be fine-tuned to fit each healthcare provider’s unique revenue
cycle process. This includes clinical laboratory and anatomic pathology
services.
“Having
business rules and workflows based on best practices to verify patient
demographics, support insurance discovery, and navigate prior authorizations
are now a minimum requirement for any healthcare provider to maintain financial
viability,” Williams notes.
To help clinical laboratories fulfill CMS’ patient access guidelines—including best practices for reversing the trend of uncollected revenue—a free white paper titled, “Patient Access Antidote: Retaining More Revenue with Front-End Solutions,” has been published by Dark Daily in partnership with Quadax.
The
white paper will provide useful insights regarding front-end patient access
management. And it will equip clinical laboratories and pathology groups with
the expert tools and solutions they need to optimize their cash flow and
successfully meet key revenue cycle objectives.
Every medical laboratory ready to begin the move away from fee-for-service payment and towards value-based reimbursement needs to start offering lab tests that support the practice of precision medicine
Nearly every clinical laboratory and pathology group in America today is aware of the opportunity to provide medical laboratory tests that enable physicians to successfully practice precision medicine. The goal of precision medicine is to enable a patient to get a more accurate diagnosis, receive the most appropriate therapy, and have his/her condition monitored with unprecedented insight during the course of treatment.
The good news for the clinical laboratory industry concerning precision medicine is that it is the fastest-growing sector of lab testing and these are the tests that contribute the greatest value in patient care. For example, molecular and genetic tests are revolutionizing the diagnosis and treatment of infectious disease. These are the clinical lab tests that enable a physician to identify the specific subtype of the bacteria or virus, then help him or her select the therapeutic drug that will have maximum benefit for the patient.
Clinical Laboratories Support Cancer Diagnosis with Companion Diagnostic Tests
It is equally true that the diagnosis and treatment of cancer is undergoing a major transformation. Genetic knowledge is being used to develop both diagnostic tests and new therapies that enable physicians to better diagnose cancer, and then treat it with the drugs identified by a companion diagnostic test as having the best potential to cure the patient or slow the progression of the disease.
But if there is an area of precision medicine with immense potential, it is pharmacogenomics and its associated testing.
In 2015, the Kaiser Family Foundation reported that more than four billion prescriptions were filled in the United States. As science understands more about the human genome, proteome, metabolome, and microbiome (to name just a few of the “omes”), it becomes possible to design clinical laboratory tests that:
1. Contribute to a more accurate diagnosis;
2. Identify which prescription drugs will be of the greatest benefit; and
3. Inform the physician as to which drugs will not be effective and may even be harmful to the patient.
More Good News for Medical Laboratories
There is even more good news. Many clinical laboratories, hospital labs, and pathology groups already have lab instruments capable of performing the tests used in precision medicine. For these labs, no major up-front investment is needed to begin offering tests that allow physicians to practice precision medicine.
“Many of our lab clients got started in this way,” stated Don Rule, MBA, Founder and Chief Executive Officer of Translational Software in Bellevue, Wash. “They realized that their existing lab instruments could run some of the lab tests physicians use when practicing precision medicine. This would be a low-cost way to enter the precision medicine field and they could, on a small scale with minimal risk, begin offering these tests to gain experience, learn more about the market, and identify which such tests would have highest value to the physicians in the communities they serve.”
Is Your Pathology Group Interested in Supporting Precision Medicine?
“For a lab that is serious about understanding the current and future clinical demand for precision medicine tests, several careful steps are recommended,” he continued. “One step is to build demand by educating clinicians and their staffs about the best ways to use these tests to improve patient care. Keep in mind that more of a physician’s reimbursement is now keyed to the patient outcomes they deliver. These doctors recognize that labs helping them do a better job with precision medicine are also helping them demonstrate greater value in the patient care they provide.
“There are other steps required to launch an effective, clinically successful precision medicine testing program,” Rule noted. “For example, labs need to understand how to be paid by the health insurers in their region. That includes getting in-network and teaching physicians and lab staff how to follow each payer’s clinical and coding criteria so that clean claims will be paid in a timely manner.
“Another step is to build the market in a careful fashion,” he emphasized. “For example, labs should identify the thought leaders among their clients and work with them to demonstrate the clinical utility of tests performed in support of precision medicine. And above all, it’s important to focus on patients that are most likely to get some insight from testing. When your lab starts with the right population, it’s remarkable how often you will uncover actionable issues.”
Clinical Labs Can Enter Precision Medicine by Initially Referring Tests
“It’s also feasible for a lab to start its precision medicine strategy by referring out testing in the early stages and using third-party experts to do the interpretations,” Rule advised. “Then, as specimen volume increases, and the lab’s clinical team gains more experience with these molecular and genetic tests, it becomes easy to bring that testing in-house to develop the market further with faster turnaround times and in-house expertise that local physicians appreciate.”
Two expert speakers will cover the essentials that all labs should know about building a market presence in precision medicine. First to present is Don Rule of Translational Software. Rule currently provides a variety of services to more than 80 lab clients, which includes the annotation and interpretation of gene sequences. In addition, Rule and his team provide consulting expertise to help labs develop their strategies for precision medicine, identify the best tests to offer physicians, and develop the steps needed to obtain network status with payers.
Webinar Will Present the Best Successes of Molecular, Genetic Testing Labs
Rule will share the experiences and best successes of the molecular and genetic testing labs he has worked with since 2009. He will discuss the types of lab tests used in precision medicine in different specialties, identify the fastest-growing sectors, and note which instruments already found in most clinical laboratories can be used to provide lab tests used for precision medicine.
Don Rule (above left), Founder and CEO of Translational Software, and Kyle Fetter (above right), Vice President of Advanced Diagnostics at XIFIN, will share their unique insights, knowledge, and experience at developing a precision medicine lab testing program for clinical laboratories that want to build more market share, make the billing/collections team more effective, and increase revenue. (Photo copyright: Dark Daily.)
As one example, a growing number of long-term care facilities are using tests to practice precision medicine—and paying for these tests under value-based arrangements—because so many of their patients are taking from 10 to 15 prescriptions each day. If a lab test indicates that the patient may not be getting therapeutic benefit from a specific drug (or that there are negative side effects from the polypharmacy), then the long-term care facility is money ahead because of less spending on drugs and the decreased care costs from patients who remain healthier. In the extreme case, the care facility might lose a patient to a skilled nursing facility due to mental fog or a fall that is precipitated by adverse drug effects.
Making the Case for a Precision Medicine Lab Testing Program
Additional topics to be discussed are:
• How to make the case to administration and the clinicians;
• How to build demand; and
• How to identify thought leaders and work with them to educate the physicians in the lab’s service region.
The second speaker will address the important topic of how to get paid. Kyle Fetter, MBA, is Vice President of Advanced Diagnostics at XIFIN, Inc., based in San Diego. XIFIN provides revenue cycle management (RCM) services to more than 200 labs and handles as many as 300 million lab test claims annually. What this means is that Fetter sees which labs are most successful with their coding, billing, and collections for molecular and genetic tests. He also sees how different payers are handling these claims.
During his presentation, Fetter will provide you and your lab team with valuable knowledge about the best ways to collect the information needed to submit clean claims and be paid promptly. He will illustrate ways to optimize the process of gathering this data and the different software tools that not only make the job easier, but help ensure that a higher proportion of claims are clean and paid at first submission.
Secrets of Preparing for Payer Challenges, Denials, and Audits
But the single best element of Fetter’s presentation will be how labs performing molecular and genetic testing should prepare, as part of the normal course of business, for the inevitable challenges, denials, and audits. He will describe the elements of a system that helps labs be ready to make the case that claims are properly documented, and that they represent appropriate and necessary tests for the patient.
You can find details for this important webinar at this link. (Or copy this URL and paste it into your browser: https://www.darkdaily.com/webinar/what-molecular-and-genetic-testing-labs-need-to-know-to-succeed-with-commercialization-of-their-precision-medicine-products.)
This webinar is perfect for any lab that is already performing molecular and genetic tests, and which is interested in building more market share, making the billing/collections team more effective, and increasing revenue.
For every lab watching the precision medicine space, this webinar is a “must attend” because it delivers to you and your lab team the collective knowledge and insights from two experts who are working with hundreds of the nation’s most successful labs. It is your guaranteed way to get the accurate, relevant information you need to craft your own lab’s strategy for expanding its molecular and genetic testing opportunities.






, Founder and CEO of Translational Software, and Kyle Fetter")
