Palmetto GBA’s Chief Medical Officer will cover how clinical laboratories billing for genetic testing should prepare for Z-Codes at the upcoming Executive War College in New Orleans
After multiple delays, UnitedHealthcare (UHC) commercial plans will soon require clinical laboratories to use Z-Codes when submitting claims for certain molecular diagnostic tests. Several private insurers, including UHC, already require use of Z-Codes in their Medicare Advantage plans, but beginning June 1, UHC will be the first to mandate use of the codes in its commercial plans as well. Molecular, anatomic, and clinical pathologist Gabriel Bien-Willner, MD, PhD, who oversees the coding system and is Chief Medical Officer at Palmetto GBA, expects that other private payers will follow.
“A Z-Code is a random string of characters that’s used, like a barcode, to identify a specific service by a specific lab,” Bien-Willner explained in an interview with Dark Daily. By themselves, he said, the codes don’t have much value. Their utility comes from the DEX Diagnostics Exchange registry, “where the code defines a specific genetic test and everything associated with it: The lab that is performing the test. The test’s intended use. The analytes that are being measured.”
The registry also contains qualitative information, such as, “Is this a good test? Is it reasonable and necessary?” he said.
Molecular, anatomic, and clinical pathologist Gabriel Bien-Willner, MD, PhD (above), Palmetto GBA’s Chief Medical Officer, will speak about Z-Codes and the MolDX program during several sessions at the upcoming Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management taking place in New Orleans on April 30-May 1. Clinical laboratories involved in genetic testing will want to attend these critical sessions. (Photo copyright: Bien-Willner Physicians Association.)
Palmetto GBA Takes Control
Palmetto’s involvement with Z-Codes goes back to 2011, when the company established the MolDX program on behalf of the federal Centers for Medicare and Medicaid Services (CMS). The purpose was to handle processing of Medicare claims involving genetic tests. The coding system was originally developed by McKesson, and Palmetto adopted it as a more granular way to track use of the tests.
In 2017, McKesson merged its information technology business with Change Healthcare Holdings LLC to form Change Healthcare. Palmetto GBA acquired the Z-Codes and DEX registry from Change in 2020. Palmetto GBA had already been using the codes in MolDX and “we felt we needed better control of our own operations,” Bien-Willner explained.
In addition to administering MolDX, Palmetto is one of four regional Medicare contractors who require Z-Codes in claims for genetic tests. Collectively, the contractors handle Medicare claims submissions in 28 states.
Benefits of Z-Codes
Why require use of Z-Codes? Bien-Willner explained that the system addresses several fundamental issues with molecular diagnostic testing.
“Payers interact with labs through claims,” he said. “A claim will often have a CPT code [Current Procedural Technology code] that doesn’t really explain what was done or why.”
In addition, “molecular diagnostic testing is mostly done with laboratory developed tests (LDTs), not FDA-approved tests,” he said. “We don’t see LDTs as a problem, but there’s no standardization of the services. Two services could be described similarly, or with the same CPT codes. But they could have different intended uses with different levels of sophistication and different methodologies, quality, and content. So, how does the payer know what they’re paying for and whether it’s any good?”
When the CPT code is accompanied by a Z-Code, he said, “now we know exactly what test was done, who did it, who’s authorized to do it, what analytes are measured, and whether it meets coverage criteria under policy.”
The process to obtain a code begins when the lab registers for the DEX system, he explained. “Then they submit information about the test. They describe the intended use, the analytes that are being measured, and the methodologies. When they’ve submitted all the necessary information, we give the test a Z-Code.”
The assessment could be as simple as a spreadsheet that asks the lab which cancer types were tested in validation, he said. On the other end of the scale, “we might want to see the entire validation summary documentation,” he said.
Commercial Potential
Bien-Willner joined the Palmetto GBA in 2018 primarily to direct the MolDX program. But he soon saw the potential use of Z-Codes and the DEX registry for commercial plans. “It became instantly obvious that this is a problem for all payers, not just Medicare,” he said.
Over time, he said, “we’ve refined these processes to make them more reproducible, scalable, and efficient. Now commercial plans can license the DEX system, which Z-Codes are a part of, to better automate claims processing or pre-authorizations.”
In 2021, the company began offering the coding system for Medicare Advantage plans, with UHC the first to come aboard. “It was much easier to roll this out for Medicare Advantage, because those programs have to follow the same policies that Medicare does,” he explained.
As for UHC’s commercial plans, the insurer originally planned to require Z-Codes in claims beginning Aug. 1, 2023, then pushed that back to Oct. 1, according to Dark Daily’s sister publication The Dark Report.
Then it was pushed back again to April 1 of this year, and now to June 1.
“The implementation will be in a stepwise fashion,” Bien-Willner advised. “It’s difficult to take an entirely different approach to claims processing. There are something like 10 switches that have to be turned on for everything to work, and it’s going to be one switch at a time.”
For Palmetto GBA, the commercial plans represent “a whole different line of business that I think will have a huge impact in this industry,” he said. “They have the same issues that Medicare has. But for Medicare, we had to create automated solutions up front because it’s more of a pay and chase model,” where the claim is paid and CMS later goes after errors or fraudulent claims.
“Commercial plans in general just thought they could manually solve this issue on a claim-by-claim basis,” he said. “That worked well when there was just a handful of genetic tests. Now there are tens of thousands of tests and it’s impossible to keep up.
They instituted programs to try to control these things, but I don’t believe they work very well.”
Bien-Willner is scheduled to speak about Palmetto GBA’s MolDX program, Z-Codes, and related topics during three sessions at the upcoming 29th annual Executive War College conference. Clinical laboratory and pathology group managers would be wise to attend his presentations. Visit here (or paste this URL into your browser: https://www.executivewarcollege.com/registration) to learn more and to secure your seat in New Orleans.
Use of such precision diagnostics offer ‘early detection, localization, and the opportunity to monitor response to therapy,’ say the MIT scientists
Oncologists and medical laboratory scientists know that most clinical laboratory tests currently used to diagnose cancer are either based on medical imaging technologies—such as CT scans and mammography—or on molecular diagnostics that detect cancer molecules in the body’s urine or blood.
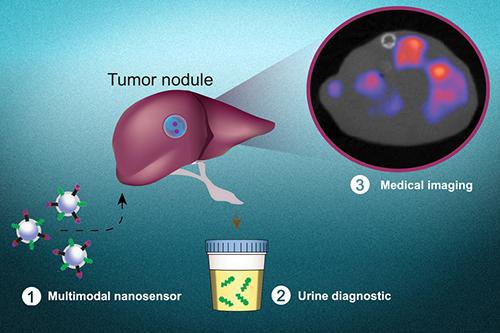
Now, in a study being conducted at the Massachusetts Institute of Technology (MIT), researchers have developed diagnostic nanoparticles that can not only detect cancer cells in bodily fluids but also image the cancer’s location. This is the latest example of how scientists are combining technologies in new ways in their efforts to develop more sensitive diagnostic tests that clinical laboratories and other providers can use to detect cancer and other health conditions.
Precision diagnostics such as molecular, imaging, and analytics technologies are key tools in the pursuit of precision medicine.
“Therapeutic outcomes in oncology may be aided by precision diagnostics that offer early detection, localization, and the opportunity to monitor response to therapy,” the authors wrote, adding, “Through tailored target specificities, this modular platform has the capacity to be engineered as a pan-cancer test that may guide treatment decisions for numerous tumor type.”
Development of Multimodal Diagnostics
The MIT scientists are developing a “multimodal” diagnostic that uses molecular screening combined with imaging techniques to locate where a cancer began in the body and any metastases that are present.
“In principle, this diagnostic could be used to detect cancer anywhere in the body, including tumors that have metastasized from their original locations,” an MIT new release noted.
“This is a really broad sensor intended to respond to both primary tumors and their metastases,” said biological engineer Sangeeta Bhatia, MD, PhD (above), in the news release. Bhatia is the John and Dorothy Wilson Professor of Health Sciences and Technology and Electrical Engineering and Computer Science at MIT and senior author of the study.
“It can trigger a urinary signal and also allow us to visualize where the tumors are,” she added. Bhatia previously worked on the development of cancer diagnostics that can produce synthetic biomarkers which are detectable in urine samples.
“The vision is that you could use this in a screening paradigm—alone or in conjunction with other tests—and we could collectively reach patients that do not have access to costly screening infrastructure today,” said Sangeeta Bhatia, MD, PhD (above), in the MIT news release. “Every year you could get a urine test as part of a general check-up. You would do an imaging study only if the urine test turns positive to then find out where the signal is coming from. We have a lot more work to do on the science to get there, but that’s where we would like to go in the long run.” (Photo copyright: NBC News.)
Precision Diagnostic Assists Assessment of Response to Cancer Therapy
For their research, the scientists added a radioactive tracer known as copper-64 to the nanoparticles. This enabled the particles to be used for positron emission tomography (PET) imaging. The particles were coated with a peptide that induced them to accumulate at tumor sites and insert themselves into cell membranes, producing a strong imaging signal for tumor detection.
The researchers tested their diagnostic nanoparticles in mouse models of metastatic colon cancer where tumor cells had traversed to the liver or the lungs. After treating the cancer cells with a chemotherapy regimen, the team successfully used both urine and imaging to determine how the tumors were responding to the treatment.
Bhatia is hopeful that this type of diagnostic could be utilized in assessing how patients are responding to treatment therapies and the monitoring of tumor recurrence or metastasis, especially for colon cancer.
What is unique about the approach used by Bhatia’s team is that one application of the copper-64 tracer can be used in vivo, in combination with imaging technology. The other application of the copper-64 tracer is in vitro in a urine specimen that can be tested by clinical laboratories.
“Those patients could be monitored with the urinary version of the test every six months, for instance. If the urine test is positive, they could follow up with a radioactive version of the same agent for an imaging study that could indicate where the disease had spread,” Bhatia said in the news release. “We also believe the regulatory path may be accelerated with both modes of testing leveraging a single formulation.”
The graphic above, taken from the MIT news release, shows how “multimodal nanosensors (1) are engineered to target and respond to hallmarks in the tumor microenvironment. The nanosensors provide both a noninvasive urinary monitoring tool (2) and an on-demand medical imaging agent (3) to localize tumor metastasis and assess response to therapy,” the news release states. (Photo and caption copyright: Massachusetts Institute of Technology.)
Precision Medicine Cancer Screening Using Nano Technologies
Bhatia hopes that the nanoparticle technology may be used as a screening tool in the future to detect any type of cancer.
Her previous research with nanoparticle technology determined that a simple urine test could diagnose bacterial pneumonia and indicate if antibiotics could successfully treat that illness, the news release noted.
Nanoparticle-based technology might be adapted in the future to be part of a screening assay that determines if cancer cells are present in a patient. In such a scenario, clinical laboratories would be performing tests on urine samples while imaging techniques are simultaneously being used to diagnose and monitor cancers.
Surgical pathologists may also want to monitor the progress of this research, as it has the potential to be an effective tool for monitoring cancer patients following surgery, chemotherapy, or radiation therapy.
Limited availability of COVID-19 clinical lab tests is major topic at federal briefings and news stories, yet many of nation’s labs are laying off staff and at point of closing
Cash flow at the nation’s clinical laboratories has crashed, with revenues down by more than $5 billion since early March. This is the biggest financial disaster for the nation’s clinical laboratory industry in its 100-year history and it couldn’t come at a worse time for the American public and the US healthcare system.
At the precise moment when the nation needs clinical laboratories to begin performing millions of tests for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, those same labs are watching their cash flow collapse.
Data from multiple sources gathered by The Dark Report, sister publication of Dark Daily, confirm that—beginning in early March and continuing through last week—clinical laboratories in the United States saw incoming flows of routine specimens decline by between 50% and 60%. During this same time, lab revenue fell by similar amounts.
Clinical Lab Industry Currently Losing $800 to $900 Million Weekly
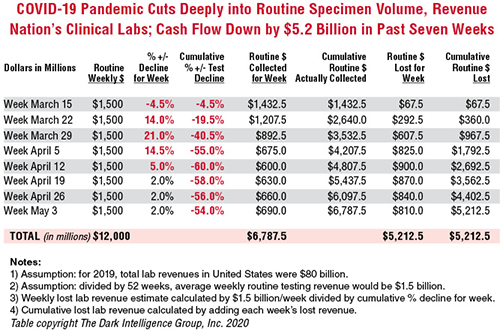
To give this decline context, the healthcare system spends about $80 billion annually on medical laboratory testing. Thus, labs across the US generated about $1.5 billion in revenue each week during 2019 and into 2020. By April 5, the decline in routine lab specimen volumes reached 55% to 60%. Since then, the clinical lab industry now loses between $800 million and $900 million each week. Total revenue loss from previous levels is already estimated to be $5.2 billion, and it is growing by an additional $800 million to $900 million every week that patients stay away from hospitals and physicians’ offices.
In the eight weeks since the COVID-19 pandemic caused patients to cease coming to hospitals and visiting their doctors, incoming routine specimens and revenue fell by 60%, causing cumulative lost routine revenue of $5.2 billion for the clinical laboratory industry in the United States. Each week that the existing shelter-in-place directives are effective, labs lose another $800 million to $900 million. The Dark Report based these estimates on data provided by multiple companies working with lab billing/claims, middleware analytical solutions, and customer relationship management (CRM) and electronic health record (EHR) products. (Chart copyright: The Dark Intelligence Group, Inc.)
The recent dire financial condition of labs small and large has gone unremarked by federal healthcare officials at the daily White House COVID-19 Task Force briefings. National news sources have yet to report on this development and its implications for successfully expanding the availability and numbers of COVID-19 tests in response to the pandemic.
The rapid and deep decline in specimens and revenue is not limited to clinical laboratories. Biopsy cases referred to anatomic pathology groups have declined by 50% to 60%. Some subspecialty pathology labs saw case referrals drop by 80% or more.
The nation’s two biggest clinical laboratory companies confirmed similar declines in their normal daily flow of routine specimens. Both companies recently reported first-quarter earnings (which included the month of March).
Quest Diagnostics, LabCorp Each Disclose Volume Declines of 50% to 60%
During its Q1 2020 earnings conference call, Chairman, President, and CEO of Quest Diagnostics (NYSE:DGX), Steve Rusckowski, stated, “In April, volume declines continue to intensify as we are seeing signs that volume declines are bottoming out at around 50% to 60%.”
The drop-off in routine lab test referrals was the similar at LabCorp (NYSE:LH). “In our diagnostics business, at the end of the quarter, we experienced reductions in demand for testing of 50% to 55% versus the company’s normal daily levels,” explained Glenn Eisenberg, Executive Vice President and CFO during LabCorp’s Q1 2020 earnings call. “This reduction in demand impacted testing volume broadly but was more heavily weighted towards routine procedures.”
Interviews with independent clinical lab owners and the administrative directors of hospital and health system labs further confirm this rapid and dramatic decline in the number of routine specimens arriving in their labs. Fewer specimens mean fewer claims, which means less revenue to laboratories.
Two Different Financial Futures for ‘Have’ Labs and ‘Have Not’ Labs
What happens next to the clinical laboratory industry in the United States—and to its ability to continue ramping up the availability of adequate numbers of COVID-19 tests in major cities, small towns, and rural areas—will be a story of “haves” and “have nots.”
The “haves” are clinical labs that have access to money. These are publicly-traded lab companies, academic medical center labs, and the sophisticated labs of health networks that operate multiple hospitals. In each case, these organizations have capital reserves and access to loans that will probably enable them to sustain COVID-19 lab testing services at the large volumes required to respond to the pandemic.
clinical labs operated by community hospitals and rural hospitals that were not financially robust before the onset of the pandemic; and,
specialty lab companies that perform a specific number of proprietary diagnostic tests (and for which demand has collapsed as patients stopped seeing their doctors).
Medicare Led Payers in the ‘Lab Test Price Race to the Bottom’
Prior to the onset of the SARS-CoV-2 pandemic, the finances of the “have-not” labs were already shaky, with many on the verge of filing bankruptcy, closing, or selling to a bigger lab company. Much blame for the deteriorating finances at a large proportion of community lab companies, community hospital labs, and rural hospital labs can be attributed to the deep, multi-year price cuts to the Medicare Part B clinical laboratory fee schedule as mandated by the Protecting Access to Medicare Act of 2014 (PAMA).
Medicare’s multi-year cuts to lab test prices were immediately copied by most state Medicaid programs. During this period, private payers followed Medicare’s lead and enacted their own deep cuts to the prices they paid labs for both routine tests and molecular/genetic tests.
That is why—when the pandemic intensified in early March—the 50% to 60% drop in specimens and revenue that hit these labs starved them of essential cash flow. When polled, the owners and directors of these labs acknowledge layoffs of the majority of their staff in all departments. They also reported substantial delays—both in submitted lab test claims and in getting payment for those claims—because claims-processing departments at the labs and private health insurers are understaffed due to shelter-in-place directives.
COVID-19 Test Revenue Helps Only Labs Performing Those Tests
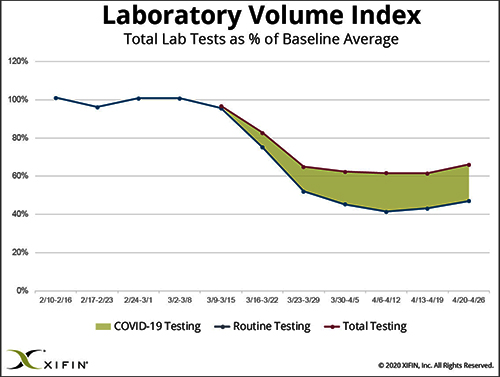
Revenue from COVID-19 testing is helping certain labs offset the revenue loss from fewer routine specimens. XIFIN, Inc., a San Diego company that provides revenue cycle management (RCM) services for clinical laboratories and pathology groups, analyzed the lab test claims for COVID-19 rapid molecular tests. It determined that labs performing these tests are generating enough revenue from these test claims to equal about 20% of their pre-pandemic revenue.
The chart above was prepared by XIFIN, Inc., of San Diego and is based on the changes XIFIN observed in the volume of routine clinical laboratory test claims generated by client labs on a weekly basis. In the first two months of 2020, routine lab test claims ran at expected levels until the first week of March. During the rest of March, routine lab test claims declined by 60%. During April, incoming routine lab test claims remained 55% to 60% below pre-pandemic levels. The shaded area shows the number of COVID-19 test claims coming into clinical labs. XIFIN says COVID-19 test claims make up about 20% of the decline in routine test specimens for those labs performing COVID-19 tests. The Dark Report estimates that the clinical laboratory industry has lost $800 million to $900 million in routine test revenue each week since March 23. Weekly revenue losses will continue at this rate until patients begin visiting their physicians and hospitals again perform elective services. (Chart copyright: XIFIN, Inc.)
Many CLIA-certified community laboratories and hospital labs have the diagnostic instruments and experience to perform rapid molecular tests for COVID-19. But when contacted, they tell us that their suppliers do not ship them even minimal quantities of the COVID-19 kits, the reagents, and the consumables. Thus, they cannot meet the needs of their client physicians. Instead, they watch as these physicians refer COVID-19 tests to the nation’s largest labs. The supply shortage prevents these smaller labs from doing larger numbers of COVID-19 test for the patients in the communities they serve. It also prevents them from earning the revenues from COVID-19 testing that currently helps the nation’s “have” labs offset the decline in revenue from routine testing.
Congress, national healthcare policymakers, and state governors need to immediately address this situation. Each week that passes during the COVID-19 pandemic and the shelter-in-place directives drains another $800 million to $900 million in revenue from routine lab testing that previously flowed into the nation’s clinical laboratories.
‘Have-not’ Clinical Labs in Small Towns Will Quietly Shrink and Disappear
Without timely intervention and financial support, the nation’s network of ‘have not’ labs, which have so capably served towns away from big metropolitan centers and rural areas, will quietly begin shrinking. One at a time, labs in small towns will close or sell. Local lab facilities will be shuttered and specimens from small-town patients will be transported to big labs hundreds or thousands of miles away.
It is also true that the financial disaster besetting the nation’s clinical laboratory industry will have comparable dramatic consequences for the in vitro diagnostics (IVD) manufacturers that sell them automation, analyzers, reagents, and other supplies. Since early March, IVD manufacturers watched as the pandemic caused orders for new instruments to collapse. During these same weeks, their clinical lab customers ceased ordering routine test kits at pre-pandemic levels. Dark Daily will cover the challenges confronting the IVD and other diagnostics industries in future e-briefings.
Announcing Free COVID-19 STAT Intelligence Briefings for Clinical Labs
With the COVID-19 pandemic creating chaos in nearly every aspect of healthcare, business, and society, clinical labs and their suppliers need timely intelligence and analysis about the innovations and successes achieved by their peers. This week, Dark Daily and The Dark Report are launching COVID-19 STAT Intelligence Briefings (Copy and paste this URL into your browser: https://www.covid19briefings.com). This comprehensive service is free and will cover four basic areas of needs for clinical laboratories as they ramp up COVID-19 testing:
Daily and weekly COVID-19 testing dashboards to guide every lab’s short-term planning;
Proven steps for labs to introduce and validate COVID-19 tests (both rapid molecular tests and serology tests);
Getting paid for COVID-19 testing to ensure every lab’s financial stability and clinical quality; and
Legal and regulatory updates for labs doing COVID19 tests to ensure full compliance.
Also, to help clinical laboratory leaders deal with the coming wave of COVID-19 serology tests, we are producing a free webinar led by James O. Westgard, PhD, FACB, and Sten Westgard, Director of Client Services and Technology, of Westgard QC, Inc.
Each week that the SARS-CoV-2 pandemic continues, and strict shelter-in-place directives are in place, the clinical laboratory industry loses another almost $900 million in revenue from lower volumes of routine testing. No industry can survive when its incoming revenue collapses by 50% to 60% for sustained periods of time.
Will Congress Recognize the Need for a Financial Rescue of ‘Have-not’ Labs?
Thus, it is incumbent on Congress, elected officials, and healthcare policymakers to recognize the financial consequences of the pandemic to the nation’s clinical laboratories. That is particularly true of the ‘have-not’ clinical labs. They do not have the same access to decisionmakers in government as billion-dollar lab companies.
And yet, these labs located in small communities and rural areas often are the only local labs that can do STAT testing in a couple of hours, and where clinical pathologists are personally familiar with local physicians and patients.
These “have-not” labs are vital healthcare resources. They should receive the help they need to get through this unprecedented crisis that is the COVID-19 pandemic.
The 80 scientists and engineers that comprise the consortium believe synthetic biology can address key challenges in health and medicine, but technical hurdles remain
Synthetic biology now has a 20-year development roadmap. Many predict this fast-moving field of science will deliver valuable products that can be used in diagnostics—including clinical laboratory tests, therapeutics, and other healthcare products.
Eighty scientists from universities and companies around the world that comprise the Engineering Biology Research Consortium (EBRC) recently published the 20-year roadmap. They designed it to “provide researchers and other stakeholders (including government funders)” with what they hope will be “a go-to resource for engineering/synthetic biology research and related endeavors,” states the EBRC Roadmap website.
Medical laboratories and clinical pathologists may soon have new tools and therapies for targeting specific diseases. The EBRC defines synthetic biology as “the design and construction of new biological entities such as enzymes, genetic circuits, and cells or the redesign of existing biological systems. Synthetic biology builds on the advances in molecular, cell, and systems biology and seeks to transform biology in the same way that synthesis transformed chemistry and integrated circuit design transformed computing.”
Synthetic biology is an expanding field and there are predictions that it may produce research findings that can be adapted for use in clinical pathology diagnostics and treatment for chronic diseases, such as cancer.
Another goal of the roadmap is to encourage federal
government funding for synthetic biology.
“The question for government is: If all of these avenues are now open for biotechnology development, how does the US stay ahead in those developments as a country?” said Douglas Friedman, EBRC’s Executive Director, in a news release. “This field has the ability to be truly impactful for society and we need to identify engineering biology as a national priority, organize around that national priority, and take action based on it.”
Designing or Redesigning Life Forms for Specific
Applications
Synthetic biology is an interdisciplinary field that combines
elements of engineering, biology, chemistry, and computer science. It enables
the design and construction of new life forms—or redesign of existing ones—for
a multitude of applications in medicine and other fields.
Another recent example comes from the Wyss Institute at Harvard. Scientist there developed a direct-to-consumer molecular diagnostics platform called INSPECTR that, they say, uses programmable synthetic biosensors to detect infectious pathogens or host cells.
The Wyss Institute says on its website that the platform can
be packaged as a low-cost, direct-to-consumer test similar to a home pregnancy
test. “This novel approach combines the specificity, rapid development, and
broad applicability of a molecular diagnostic with the low-cost, stability, and
direct-to-consumer applicability of lateral flow immunoassays.”
In March, Harvard announced that it had licensed the technology to Sherlock Biosciences.
Howard Salis, PhD (above), Associate Professor of biological engineering and chemical engineering at Pennsylvania State University (Penn State), co-chaired the EBRC Roadmapping Working Group that produced the roadmap. In a Penn State news story, Salis explained synthetic biology’s potential. “There are both traditional and startup companies leveraging synthetic biology technologies to develop novel biotech products,” he said. “Organisms that produce biorenewable materials; diagnostics to detect the Zika virus, Ebola and tuberculosis; and soil bacteria that fix nitrogen into ammonia for improved plant growth.” (Photo copyright: Twitter.)
Fundamental Challenges with Synthetic Biology
The proponents of synthetic biology hope to make it easier
to design and build these systems, in much the same way computer engineers
design integrated circuits and processors. The EBRC Roadmap may help scientist
worldwide achieve this goal.
However, in “What is Synthetic/Engineering Biology?” the EBRC also identifies the fundamental challenges facing the field. Namely, the complexity and unpredictability inherent in biology, and a limited understanding of how biological components interact.
The EBRC roadmap report, “Engineering Biology: A Research
Roadmap for the Next-Generation Bioeconomy,” covers five categories of applications:
Health and medicine are of primary interest to pathologists.
Synthetic Biology in Health and Medicine
The Health and Medicine section of the report identifies
four broad societal challenges that the EBRC believes can be addressed by
synthetic biology. For each, the report specifies engineering biology
objectives, including efforts to develop new diagnostic technologies. They
include:
Existing and emerging infectious diseases: Objectives include development of tools for treating infections, improving immunity, reducing dependence on antibiotics, and diagnosing antimicrobial-resistant infections. The authors also foresee tools for rapid characterization and response to “known and unknown pathogens in real time at population scales.”
Non-communicable diseases and disorders, including cancer, heart disease, and diabetes: Objectives include development of biosensors that will measure metabolites and other biomolecules in vivo. Also: tools for identifying patient-specific drugs; tools for delivering gene therapies; and genetic circuits that will foster tissue formation and repair.
Environmental health threats, such as toxins, pollution, and injury: Objectives include systems that will integrate wearable tech with living cells, improve interaction with prosthetics, prevent rejection of transplanted organs, and detect and repair of biochemical damage.
Healthcare access and personalized medicine: The authors believe that synthetic biology can enable personalized treatments and make new therapies more affordable.
Technical Themes
In addition to these applications, the report identifies
four “technical themes,” broad categories of technology that will spur the
advancement of synthetic biology:
Gene editing, synthesis, and assembly: This refers to tools for producing chromosomal DNA and engineering whole genomes.
Biomolecule, pathway, and circuit engineering: This “focuses on the importance, challenges, and goals of engineering individual biomolecules themselves to have expanded or new functions,” the roadmap states. This theme also covers efforts to combine biological components, both natural and non-natural, into larger, more-complex systems.
Host and consortia engineering: This “spans the development of cell-free systems, synthetic cells, single-cell organisms, multicellular tissues and whole organisms, and microbial consortia and biomes,” the roadmap states.
Data Integration, modeling, and automation: This refers to the ability to apply engineering principles of Design, Build, Test and Learn to synthetic biology.
The roadmap also describes the current state of each
technology and projects likely milestones at two, five, 10, and 20 years into
the future. The 2- and 5-year milestones are based on “current or recently
implemented funding programs, as well as existing infrastructure and facilities
resources,” the report says.
The longer-term milestones are more ambitious and may
require “significant technical advancements and/or increased funding and
resources and new and improved infrastructure.”
Synthetic biology is a significant technology that could
bring about major changes in clinical pathology diagnostics and treatments.
It’s well worth watching.
Research goal was to isolate circulating tumor cells in venipuncture samples with improved purity compared to standard spiral chips
Many research teams are pursuing the goal of creating assays that detect circulating tumor cells (CTCs) that would allow earlier and more accurate diagnosis of cancer. Now comes news of a unique technology developed at the University of Michigan (U-M) Ann Arbor that showed promised in an early study.
The method of using CTCs to diagnose cancer in patients, while further analyzing specific characteristics of a given cancer case, shows promise as an innovative tool for clinical laboratories and oncologists. However, current approaches face challenges when it comes to proving accuracy and establishing thresholds that might indicate the need for further action.
Researchers at U-M believe they may have solved that problem. They created “Labyrinth,” a “label-free microfluidic device” that condenses 637mm of channels—including 11 loops and 56 corners—onto a 500μm-wide chip that uses inertia and Dean flow to separate white blood cells and CTCs from venipuncture samples at rates as high as 2.5ml per minute. These results improve upon the traditional spiral chip design.
Publishing their findings in Cell Systems, first author of the study Eric Lin, PhD, noted, “With the recent advances in tools for genomic characterization, it is more compelling than ever to look at the tumor heterogeneity to understand tumor progression and resistance to therapies. The Labyrinth device enabled high yields of CTCs without the bias induced by antibody-based selection, allowing the identification of true biological tumor heterogeneity.”
The graphic above, taken from the University of Michigan study, demonstrates the “High-throughput and label-free Labyrinth device that enables single CTC isolation and gene expression characterization.” According to the researchers, “Labyrinth offers a cell-surface marker-independent single-cell isolation platform to study heterogeneous CTC subpopulations.” The U-M study shows promise in creating tools for oncologist and clinical laboratory cancer treatment. (Image copyright: University of Michigan/Cell Systems.)
Challenges in the Isolation of CTCs
The Labyrinth chip is not the first device to assist in isolating CTCs. The U-M study notes that while immune-affinity capture is a validated approach to prognosis, therapeutic monitoring and molecular diagnostics, it does not work with all cancer cases. The researchers also note the method creates challenges in single-cell analysis later.
Existing label-free methods of isolation, such as deterministic lateral displacement, microfluidic flow fractionation, and acoustic-based separation, avoid these concerns but face issues of their own. The researchers noted, “Issues encountered with these approaches include pore clogging, high-pressure drop, pre-fixation to prevent CTC loss, low throughput, and excessive non-specific cell retention.”
The researchers further clarified that a major factor separating the Labyrinth chip from other methods is the ability to identify CTC subpopulations without the need for manual selection based on positive or negative protein expression. Thus, improving the ability to conduct further single-cell analysis from the results. Testing of the Labyrinth chip involved a variety of cancer cell lines, including:
· Human breast (MCF-7);
· Pancreatic (PANC-1);
· Prostate (PC-3); and,
· Lung (H1650).
And while standard spiral chips are already a common method for conducting size-based sorting, the purity of results is less than ideal with thousands of other cells remaining in the sample.
The researchers reported that the Labyrinth chip recovered 91.5% (plus or minus 0.9%) of cancer cells and removed 91.4% (plus or minus 3.3%) of white blood cells in a spiked buffer test.
“Bigger cells, like most cancer cells, focus pretty fast due to the curvature. But the smaller the cell is, the longer it takes to get focused,” Sunitha Nagrath, PhD, Associate Professor of Chemical Engineering and a lead developer of the Labyrinth chip, stated in a U-M news release. “The corners produce a mixing action that makes the smaller white blood cells come close to the equilibrium position much faster.”
Labyrinth also supports a series configuration of multiple chips. While testing two chips in series, researchers noted “a two-log improvement in tumor cell enrichment over the single Labyrinth.” They claim this is a higher purity than other label-free methods they studied, while adding only five minutes to processing times.
Sunitha Nagrath, PhD (above), is an Associate Professor of Chemical Engineering at the University of Michigan, and one of the lead developers of the Labyrinth chip. “You cannot put a box around these cells,” she noted in the U-M news release. “The markers for them are so complex, there is no one marker we could target for all these stages.” (Photo copyright: University of Michigan.)
Current Testing Using the Labyrinth Chip
The chip is already in use in a clinical trial for an aggressive form of breast cancer by Max Wicha, MD, Madeline and Sidney Forbes Professor of Oncology, Founding Director Emeritus, University of Michigan Comprehensive Cancer Center, and co-author of the Cell Systems study, who lead the study along with Nagrath.
The trial involves the attempted activation of adult system cells by blocking the signaling molecule interleukin-6. Wicha suspects the molecule enables cancer stem cells as well. “We think that this may be a way to monitor patients in clinical trials,” he said in the U-M news release. “Rather than just counting the cells, by capturing them, we can perform molecular analysis [to] know what we can target with treatments.”
The news release further highlights how this chip is specifically suited to such a task. As cancer stem cells transition from stem-like cells to more ordinary cell types, their gene expression shifts as well. This creates an issue when using conventional cell targeting. Nagrath notes this concern, stating, “The markers for [cancer stem cells] are so complex, there is no one marker we could target for all these stages.”
The Labyrinth chip shows potential for overcoming one of the biggest hurdles to leveraging CTCs to diagnose cancers and develop personalized therapies. Currently, the chip can output to Fluidigm, DEPArray by Silicon Biosystems, and RainDance Technologies’ RainDrop Digital PCR System.
The U-M researchers hope that future research will yield additional applications and compatible systems to further improve the ability for medical laboratories to use CTCs in the early detection and monitoring of cancer cases.