Another report finds nearly half of all healthcare systems planning to opt out of Medicare Advantage plans because of issues caused by prior authorization requirements
Prior-authorization is common and neither healthcare providers (including clinical laboratories) nor Medicare Advantage (MA) health plans are happy with the basic process. Thus, labs—which often must get prior-authorization for molecular diagnostics and genetic tests—may learn from a recent KFF study of denial rates and successful appeals.
“While prior authorization has long been used to contain spending and prevent people from receiving unnecessary or low-value services, it also has been [the] subject of criticism that it may create barriers to receiving necessary care,” KFF, a health policy research organization, stated in a news release.
Nearly all MA plan enrollees have to get prior authorization for high cost services such as inpatient stays, skilled nursing care, and chemotherapy. However, “some lawmakers and others have raised concerns that prior authorization requirements and processes, including the use of artificial intelligence to review requests, impose barriers and delays to receiving necessary care,” KFF reported.
“Insurers argue the process helps to manage unnecessary utilization and lower healthcare costs. But providers say prior authorization is time-consuming and delays care for patients,” Healthcare Dive reported.
“There are a ton of barriers with prior authorizations and referrals. And there’s been a really big delay in care—then we spend a lot of hours and dollars to get paid what our contracts say,” said Katie Kucera (above),Vice President and CFO, Carson Tahoe Health, Carson City, Nev., in a Becker’s Hospital CFO Report which shared the health system’s plan to end participation in UnitedHealthcare commercial and Medicare Advantage plans effective May 2025. Clinical laboratories may want to review how test denials by Medicare Advantage plans, and the time cost of the appeals process, affect the services they provide to their provider clients. (Photo copyright: Carson Tahoe Health.)
Key Findings of KFF Study
To complete its study, KFF analyzed “data submitted by Medicare Advantage insurers to CMS to examine the number of prior authorization requests, denials, and appeals for 2019 through 2022, as well as differences across Medicare Advantage insurers in 2022,” according to a KFF issue brief.
Here are key findings:
Requests for prior authorization jumped 24.3% to 46 million in 2022 from 37 million in 2019.
More than 90%, or 42.7 million requests, were approved in full.
About 7.4%, or 3.4 million, prior authorization requests were fully or partially denied by insurers in 2022, up from 5.8% in 2021, 5.6% in 2020, and 5.7% in 2019.
About 9.9% of denials were appealed in 2022, up from 7.5% in 2019, but less than 10.2% in 2020 and 10.6% in 2021.
More than 80% of appeals resulted in partial or full overturning of denials in the years studied. Still, “negative effects on a person’s health may have resulted from delay,” KFF pointed out.
KFF also found that requests for prior authorization differed among insurers. For example:
Humana experienced the most requests for prior authorization.
Among all MA plans, the share of patients who appealed denied requests was small. The low rate of appeals may reflect Medicare Advantage plan members’ uncertainty that they can question insurers’ decisions, KFF noted.
It’s a big market. Nevertheless, “between onerous authorization requirements and high denial rates, healthcare systems are frustrated with Medicare Advantage,” according to a Healthcare Financial Management Association (HFMA) survey of 135 health system Chief Financial Officers.
According to the CFOs surveyed, 19% of healthcare systems stopped accepting one or more Medicare Advantage plans in 2023, and 61% are planning or considering ending participation in one or more plans within two years.
“Nearly half of health systems are considering dropping Medicare Advantage plans,” Becker’s reported.
Federal lawmakers acted, introducing three bills to help improve timeliness, transparency, and criteria used in prior authorization decision making. Starting in 2023, KFF reported, the federal Centers for Medicare and Medicaid Services (CMS) published final rules on the bills:
Rule One (effective June 5, 2023), “clarifies the criteria that may be used by Medicare Advantage plans in establishing prior authorization policies and the duration for which a prior authorization is valid. Specifically, the rule states that prior authorization may only be used to confirm a diagnosis and/or ensure that the requested service is medically necessary and that private insurers must follow the same criteria used by traditional Medicare. That is, Medicare Advantage prior authorization requirements cannot result in coverage that is more restrictive than traditional Medicare.”
Rule Two (effective April 8, 2024), is “intended to improve the use of electronic prior authorization processes, as well as the timeliness and transparency of decisions, and applies to Medicare Advantage and certain other insurers. Specifically, it shortens the standard time frame for insurers to respond to prior authorization requests from 14 to seven calendar days starting in January 2026 and standardizes the electronic exchange of information by specifying the prior authorization information that must be included in application programming interfaces starting in January 2027.”
Rule Three (effective June 3, 2024), requires “Medicare Advantage plans to evaluate the effect of prior authorization policies on people with certain social risk factors starting with plan year 2025.”
KFF’s report details how prior authorization affects patient care and how healthcare providers struggle to get paid for services rendered by Medicare Advantage plans amid the rise of value-based reimbursements.
Clinical laboratory leaders may want to analyze their test denials and appeals rates as well and, in partnership with finance colleagues, consider whether to continue contracts with Medicare Advantage health plans.
Request for money upfront comes at a time when many patients already struggle with medical debt
In its reporting of healthcare trends gathering momentum, a national newspaper caused quite a stir this spring when it published a story documenting how some hospitals now require patients to pay in advance of specified surgeries and procedures. Hospitals are recognizing what clinical laboratories have long known—a larger proportion of Americans do not have the cash to pay a medical bill.
Hospitals and surgery centers are requesting advanced payment for elective procedures such as knee replacements, CT scans, and childbirth procedures, according to an Advisory Board daily briefing.
“In some cases, they may also have a contract with an insurance company. And in that contract are terms that stipulate hospitals need to collect deductibles or co-insurance before a procedure,” Evans added.
According to Bankrate’s 2024 Annual Emergency Savings Report, nearly half of all American’s would be unable to pay cash for an unplanned $1,000 bill. Therefore, one wonders why hospitals would attempt to extract payments from patients in advance of medical visits and clinical laboratory testing. Wouldn’t that just reduce the number of patients electing to undergo needed surgeries and other costly procedures? Nevertheless, it appears that many hospitals struggling financially are doing just that, according to The Wall Street Journal.
Genetic testing laboratories have a similar problem because of high-deductible health plans ($5K/year for individual, $12K/year for family). It means that many patients, even with insurance, struggle to pay a $1,000 to $5,000 bill for a genetic test.
Requesting payment from patients before healthcare visits is not new. However, the practice is on the rise and comes at a time when consumers are already struggling to make ends meet.
“Hospitals collected (in Q1 2024) about 23% of what patients owed them before they set foot in a hospital or doctor’s office. That’s up from about 20% in the same period a year earlier,” said reporter Melanie Evans (above) of The Wall Street Journal, referring to data from 1,850 hospitals analyzed by Kodiak Solutions. Genetic testing laboratories experience similar challenges getting paid due to many people struggling with high deductible health plans. (Photo copyright: LinkedIn.)
Price Transparency Behind Upfront Payments
According to a recent KFF survey of US families, “about half of adults would be unable to pay an unexpected medical bill of $500 in full without going into debt.”
Regardless, asking for payment for nonemergency care has become more common as people increasingly choose health plans with high-deductibles and amid the push for greater price transparency, according to Richard Gundling, Senior Vice President, Content and Professional Practice Guidance at Healthcare Financial Management Association (HFMA), in an interview with Advisory Board.
“It’s very common if not the norm” for hospitals to give patients a cost estimate and ask for advance payment, Gundling stated during the interview.
In fact, healthcare providers and insurers are required to shared charges and estimates as part of newly implemented federal rules. According to the American Hospital Association (AHA) those statutes and rules include:
The Hospital Price Transparency Final Rule (effective January 2021) which requires hospitals to publicly post “standard charges” via machine readable files.
The No Surprises Act which mandates the sharing of “good faith estimates” with uninsured/self-pay patients for most scheduled services and also requires insurers to provide explanation of benefits to enrollees.
According to Consumer Reports, hospitals are finding consumers less reliable payers than insurance companies. “No one would say, ‘Pay up or we won’t treat you.’ But we’re saying that, ‘You have a large out-of-pocket cost, and we want to know how are you going to pay for it,’” explained Jonathan Wiik, Vice President of Health Insights at FinThrive, a revenue cycle management company.
Razor Thin Hospital Margins
For their part, hospitals, health systems, and medical practices wrote off $17.4 billion in bad debt in 2023, Kodiak Solutions, an Indianapolis-based healthcare consulting and software company, reported in a news release.
“With the amounts that health plans require patients to pay continuing to grow, provider organizations need a strategy to avoid intensifying pressure on their already thin margins,” said Colleen Hall, Senior Vice President, Revenue Cycle, Kodiak, in the news release.
“Patient collections have become an increasingly difficult challenge for hospitals due primarily to a shift in payer mix. Because of rising deductibles and increased patient responsibility, the percentage of healthcare provider revenue collected directly from patients increased to more than 30% from less than 10% over 10 years,” the HFMA noted.
Thus, the financial tension being experienced by both patients and providers, and the need for patients to prepay for some treatment, are extreme challenges. The situation may call for clinical laboratory leaders to not only focus on quality testing and efficient workflow, but also affordability and access to services.
Medical laboratories and anatomic pathologists may need to squeeze into narrow networks to be paid under value-based schemes, especially where Medicare Advantage is concerned
Pathologists have likely heard the arguments in favor of value-based payment versus fee-for-service (FFS) reimbursement models: FFS encourages providers to order medically unnecessary procedures and lab tests. FFS removes incentives for providers to order patient services more carefully. Fraudsters can generate huge volumes of FFS claims that take payers months/years to recognize and stop.
Studies that favor value-based payment schemes support these claims. But do hospitals and other healthcare providers also accept them? And how is value-based reimbursement really doing?
To find out, Chicago-based thought leadership and advisory company 4Sight Health culled data from various organizations’ reports that suggest value-based reimbursement shows signs of growth as well as signs of stagnation.
Value-Based Payment Has Its Ups and Downs
Healthcare journalist David Burda is News Editor and Columnist at 4Sight Health. In his article, “Is Value-Based Reimbursement Mostly Dead or Slightly Alive?” Burda commented on data from various industry reports that indicated value-based reimbursement shows “signs of life.” For example:
More doctors are accepting pay-for-performance payments: 44.5% in 2020, up from 42.3% in 2018, according to an American Medical Association (AMA) biennial report on physician participation in value-based reimbursement, titled, “Policy Research Perspectives: Payment and Delivery in 2020.”
On the other hand, Burda reported that value-based reimbursement also has these declining indicators:
39.3% of provider payments “flowed” through FFS plans in 2020 with no link to cost or quality. This was unchanged since 2019. (HCPLAN report)
19.8% of FFS payments to providers in 2020 were linked to cost or quality, down from 22.5% in 2019. (HCPLAN report)
88% of doctors reported accepting FFS payments in 2019, an increase from 87% in 2018. (AMA report)
Does Today’s Healthcare Industry Support Value-based Care?
A survey of 680 physicians conducted by the Deloitte Center for Health Solutions suggests the answer could be “not yet.” In “Equipping Physicians for Value-Based Care,” Deloitte reported:
“Physician compensation continues to emphasize volume more than value.
“Availability and use of data-driven tools to support physicians in practicing value-based care continue to lag.
“Existing care models do not support value-based care.”
Deloitte analysts wrote, “Physicians increasingly recognize their role in improving the affordability of care. We repeated a question we asked six years ago and saw a large increase in the proportion of physicians who say they have a prominent role in limiting the use of unnecessary treatments and tests: 76% in 2020 vs. 57% in 2014.
“Physicians also recognize that today’s care models are not geared toward value,” Deloitte continued. “They see many untapped opportunities for improving quality and efficiency. They estimate that even today, sizable portions of their work can be performed by nonphysicians (30%) in nontraditional settings (30%) and/or can be automated (18%), creating opportunities for multidisciplinary care teams and clinicians to work at the top of their license.”
Hospital CFOs Also See Opportunities for Value-based Care
This could be problematic for clinical laboratories, according to Robert Michel, Editor-in-Chief of Dark Daily and our sister publication The Dark Report. According to Guidehouse, “Nearly 60% of health systems plan to advance into risk-based Medicare Advantage models in 2022.”
Medicare Advantage (MA) enrollments have escalated over 10 years: 26.4 million people of the 62.7 million eligible for Medicare chose MA in 2021, noted a Kaiser Family Foundation brief that also noted MA enrollment in 2021 was up by 2.4 million beneficiaries or 10% over 2020.
The graph above is taken from the Kaiser Family Foundation report, “Medicare Advantage in 2021: Enrollment Update and Key Trends.” According to the KFF, “In 2021, more than four in 10 (42%) Medicare beneficiaries—26.4 million people out of 62.7 million Medicare beneficiaries overall—are enrolled in Medicare Advantage plans; this share has steadily increased over time since the early 2000s.” Since MA employs narrow networks for its healthcare providers, it’s likely this trend will continue to affect clinical laboratories that may find it difficult to access these providers. (Graphic copyright: Kaiser Family Foundation.)
“The shift from Medicare Part B—where any lab can bill Medicare on behalf of patients for doctor visits and outpatient care, including lab tests—to Medicare Advantage is a serious financial threat for smaller and regional labs that do a lot of Medicare Part B testing. The Medicare Advantage plans often have networks that exclude all but a handful of clinical laboratories as contracted providers,” Michel cautioned. “Moving into the future, it’s incumbent on regional and smaller clinical laboratories to develop value-added services that solve health plans’ pain points and encourage insurers to include local labs in their networks.”
Medical laboratories and anatomic pathology groups need to be aware of this trend. Michel says value-based care programs call on clinical laboratories to collaborate with healthcare partners toward goals of closing care gaps.
“Physicians and hospitals in a value-based environment need a different level of service and professional consultation from the lab and pathology group because they are being incented to detect disease earlier and be active in managing patients with chronic conditions to keep them healthy and out of the hospital,” he added.
Value-based reimbursement may eventually replace fee-for-service contracts. The change, however, is slow and clinical laboratories should monitor for opportunities and potential pitfalls the new payment arrangements might bring.
Experts say Amazon could be planning a roll-out of healthcare services to its Prime members and others
Clinical laboratory leaders will want to note that the Telehealth and home healthcare industries have expanded with the launch of Amazon Care, a virtual medical clinic and home care services program from global retailer Amazon.com, Inc. (NASDAQ:AMZN).
Amazon is piloting Amazon Care as a benefit for its 53,000
Seattle-area employees and their families, according to published reports. Could
this indicate the world’s largest online retailer is moving into the primary
care space? If so, clinical laboratory leaders will want to follow this
development closely, because the program will need clinical laboratory support.
Amazon has successfully disrupted multiple industries in its
corporate life and some experts speculate Amazon may be using its own employees
to design a new medical delivery model for national roll-out.
The S&P report goes on to state, “In as little as five years, the Seattle-based e-commerce company could interlink its system of capabilities and assets to launch various healthcare products, insurance plans, virtual care services, and digital health monitoring to a broader population. The rollout would be part of a larger plan by Amazon to deliver convenient, cost-effective access to care and medications across the U.S., likely tied to Amazon’s Prime membership program, according to experts.”
Modern Healthcare reported that Amazon Care services include telemedicine and home visits to employees enrolled in an Amazon health insurance plan.
Experts contacted by S&P Global Market Intelligence
suggest Amazon:
Plans a “suite of customized health plans and
services for businesses and consumers;”
May offer health services to its five million
seller business and more than 100 million Amazon Prime members; and
Sees healthcare as a growing market and wants
greater involvement in it.
How Amazon Care Works
Amazon Care offers online, virtual care through a
downloadable mobile device application (app) as well as in-person home care for
certain medical needs, such as:
Colds, allergies, infections, and minor injury;
Preventative consults, vaccines, and lab tests;
Sexual health services; and
General health inquiries.
Becker’s Hospital Review reported that once a participant downloads the Amazon Care app to a smartphone or tablet and signs up for the program, he or she can:
Communicate with healthcare providers via text
or video;
Plan personal visits if needed;
Set payment methods in their user profile; and
Receive a “potential diagnosis” and treatment
plan.
The graphic above is taken from the S&P Global Market Intelligence report, which states, “Amazon is one of several tech firms vying for a share of the healthcare market where national spending is expected to reach $6.0 trillion by 2027, up from $3.6 trillion in 2018, according to the Centers for Medicare and Medicaid Services.” (Graphic copyright: S&P Global Market Intelligence.)
“The service eliminates travel and wait time, connecting employees and their family members to a physician or nurse practitioner through live chat or voice,” an Amazon spokesperson told CNBC, “with the option for in-person follow-up services from a registered nurse ranging from immunizations to instant strep throat detection.”
The “mobile health nurse” may also collect clinical laboratory
specimens, the Verge
reported.
Amazon has partnered with Oasis Medical Group, a family primary care practice in Seattle, to provide healthcare services for Amazon Care patients.
Paving the Way to Amazon Care
The Healthcare Financial Management Association (HFMA) compares Amazon’s piloting of Amazon Care to similar healthcare projects that studied population health by first involving employee health plans.
HFMA’s analysis noted that Amazon Care is similar to Haven, a patient advocate organization based in Boston and New York that was created in 2018 by Amazon, JPMorgan Chase, and Berkshire Hathaway to lower healthcare costs and improve outcomes for participating companies.
Tech Crunch reported that in 2018 Amazon also purchased PillPack for nearly $1 billion and integrated its prescription delivery services into Amazon Care.
More recently, Amazon acquired Health Navigator and plans to bring those offerings to Amazon Care as well, CNBC reported. Founded in 2014, Health Navigator provides caregivers with symptom-checking tools that enable remote diagnoses.
Should Telemedicine Firms Be Nervous?
Dark Daily recently reported on Doctor on Demand’s launch of its own virtual healthcare telehealth platform called Synapse. The e-briefing also covered Doctor on Demand’s partnership with Humana (NYSE:HUM) to provide virtual primary care services to the insurer’s health plan members, including online doctor visits at no charge and standard medical laboratory tests for a $5 copayment.
So, should telemedicine firms be concerned about Amazon competing in their marketplace? Business Insider predicts Amazon will need time to beef up its medical resources to serve people online and in-person through Amazon Care.
But that’s the point of Amazon’s pilot, isn’t it? What comes
from it will be interesting to watch.
“Meanwhile, telemedicine firms can ink strategic
partnerships and strengthen their existing payer relationships to safeguard
against Amazon’s surge into the space,” Business Insider advised.
It remains to be seen how medical laboratory testing and reports
would fit into an expanded Amazon Care health network. Or, how clinical laboratories
will get “in-network” with Amazon Care, as it grows to serve customers beyond
Amazon’s employees.
As Dark Daily recently advised, medical laboratory leaders will want to ensure their lab’s inclusion in virtual care networks, which someday may include Amazon Care.
Clinical laboratories that service both settings could be impacted as new CMS proposed rule attempts to align Medicare’s payment policies for outpatient and in-patient settings
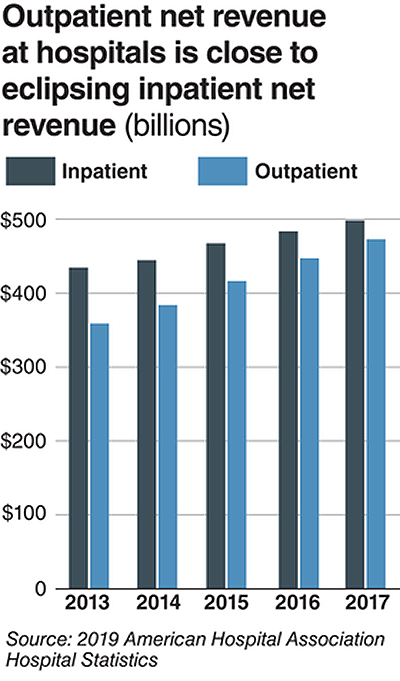
Hospital outpatient revenue is catching up to inpatient
revenue, according to data released from the American
Hospital Association (AHA). This increase is part of a growing trend to
reduce healthcare costs by treating patients outside of hospital settings. It’s
a trend that is supported by the White House and Medicare and continues to
impact clinical
laboratories, which serve both hospital inpatient and outpatient customers.
The AHA published this study data in its annual Hospital Statistics, 2019Edition. The data comes from a 2017 survey of 5,262
US hospitals. The report includes data about utilization, revenue, expenses,
and other indicators for 2017, as well as historical data.
The AHA statistics on outpatient revenue suggest providers
nationwide are working to keep people out of more expensive hospital settings. Hospitals,
like medical
laboratories, appear to be succeeding at developing outpatient and outreach
services that generate needed operating revenue.
This aligns with Medicare’s push to make healthcare more accessible through outpatient settings, such as urgent care clinics and physician’s offices. A growing trend Dark Daily has covered extensively.
Outpatient Revenue
Climbs
In its coverage of
the AHA’s study, Modern Healthcare reported that 2017
hospital net inpatient revenue was $498 billion and net outpatient revenue was
$472 billion.
The Becker’s Hospital CFO Report notes that
gross inpatient revenue in 2017 was $92.7 billion higher than gross outpatient
revenue. But in 2016, gross inpatient revenue was much further ahead—$129.5
billion more than gross outpatient revenue. The “divide” between inpatient and
outpatient revenue is narrowing, Becker’s reports.
The graphic above illustrates the shrinking gap between hospital inpatient and outpatient revenues. “Outpatient revenue will ultimately eclipse inpatient revenue,” Chuck Alsdurf, Director of Healthcare Finance Policy and Operational Initiatives at the Healthcare Financial Management Association (HFMA), told Modern Healthcare. (Graphic copyright: Modern Healthcare/AHA.)
The Becker’s
report also stated:
Admissions increased by less than 1% to 34.3
million in 2017, up from 34 million in 2016;
Inpatient days were flat at 186.2 million;
Outpatient visits rose by 1.2% to 766 million in
2017; and,
Outpatient revenue increased 5.7% between 2016
and 2017.
Similar Study Offers Additional
Insight into 2018 Outpatient Revenue
A benchmarking report by Crowe,
a public accounting, consulting, and technology firm, which analyzed data from
622 hospitals for the period January through September of 2017 and 2018, showed
the following, as reported by RevCycleIntelligence:
Inpatient volume was up 0.6% in 2018 and gross
revenue per case grew by 5.3%;
Outpatient services rose 2.4% in 2018 and gross
revenue per case was up 7.1%.
Physicians’ Offices
Have Lower Prices for Some Hospital Outpatient Services
Everything, however, is relative. When certain healthcare
services traditionally rendered in physician’s offices are rendered, instead,
in hospital outpatient settings, the numbers tell a different story.
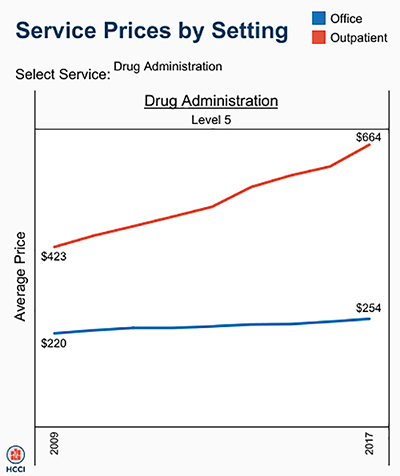
In fact, according to the Health
Care Cost Institute (HCCI), the price for services was “always higher” when
performed in an outpatient setting, as compared to doctor’s offices.
HCCI analyzed services at outpatient facilities as well as
those appropriate to freestanding physician offices. They found the following
differences in 2017 prices:
Diagnostic and screening ultrasound: $241 in
physician’s office—$650 in hospital outpatient setting;
Level 5 drug administration: $254 in office—$664
in hospital outpatient setting;
Upper airway endoscopy: $527 in office—$2,679 in
hospital outpatient setting.
One example where hospital outpatient settings provide similar services at increased costs is in drug administration, as the graphic above illustrates. “The difference was higher than I expected. With some services, the price is two or three times higher when rendered in the outpatient setting,” Julie Reiff, HCCI researcher and report author, told Fierce Healthcare. (Graphic copyright: HCCI.)
Medicare Proposed
Rule Would Change How Hospital Outpatient Clinics Get Paid
Meanwhile, the Centers for
Medicare and Medicaid Services (CMS) has released its final rule (CMS-1695-FC),
which make changes to Medicare’s hospital outpatient prospective payment and
ambulatory surgical center payment systems and quality reporting programs.
In a news
release, CMS stated that it “is moving toward site neutral payments for
clinic visits (which are essentially check-ups with a clinician). Clinic visits
are the most common service billed under the OPPS [Medicare’s Hospital
Outpatient Prospective Payment System). Currently, CMS often pays more for
the same type of clinic visit in the hospital outpatient setting than in the
physician office setting.”
“CMS is also proposing to close a potential loophole through
which providers are billing patients more for visits in hospital outpatient
departments when they create new service lines,” the news release states.
Hospitals are fighting the policy change through a lawsuit, Fierce Healthcare reported.
In summary, clinical laboratories based in hospitals and
health systems are in the outpatient as well as inpatient business. Medical laboratory
tests contribute to growth in outpatient revenue, and physician offices compete
with clinical laboratories for some outpatient tests and procedures. Thus, a new
site-neutral CMS payment policy could affect the payments hospitals receive for
clinic visits by Medicare patients.