Novel scheme by medical laboratory company to induce patients to collect and return their own specimen for testing is central to a federal whistleblower case alleging violations of the Anti-Kickback Statute
Handing out gift cards only to patients who return a specimen to a clinical laboratory company for colorectal cancer screening is a unique approach that is now at the center of a federal qui tamcase filed by a retired Indiana pathologist.
The defendant in this whistleblower lawsuit is Exact Sciences Laboratories and its parent company Exact Sciences Corporation (NASDAQ:EXAS). Last month, a federal judge ruled the court case will proceed following attempts by the defendant’s attorneys to have the case dismissed.
The plaintiffs (United States of America ex rel. Niles Rosen, MD) allege Exact Sciences Laboratories violated the Federal Anti-Kickback Statute (AKS) and False Claims Act by offering $75 gift cards to induce patients to return self-collected fecal samples for the lab’s Cologuard at-home colon cancer screening kit through its Patient Compliance Program.
Exact Sciences refuted the allegations and moved to have the case dismissed claiming it “had a good faith belief that its [Patient Compliance Program] complied with the law and thus lacked the requisite intent for a violation of the AKS,” according to court documents. The court denied Exact Sciences’ motion to dismiss.
“We are grateful for the hard work and courage of those private citizens who bring evidence of fraud to the Department’s attention, often putting at risk their careers and reputations,” said Brian Boynton, JD (above), Principal Deputy Assistant Attorney General and head of the federal Department of Justice (DOJ) Civil Division in a February 7, 2023, DOJ statement. “Our ability to protect citizens and taxpayer funds continues to benefit greatly from their actions.” Clinical laboratory managers will want to follow this and other qui tam cases claiming violation of anti-kickback laws. (Photo copyright: Department of Justice.)
.
Was Exact Sciences’ Patient Compliance Program a Kickback?
Cologuard is a non-invasive testing kit utilized by people to screen for colorectal cancer in the privacy of their own homes. It is intended for those over the age of 45 who are at low or average risk for the disease. Exact Sciences regularly runs television advertisements urging individuals to be screened for colorectal cancer using the Cologuard test.
Following a physician’s order, and after receiving the testing kit in the mail, individuals collect a stool sample using the specimen container in the kit and return the sample to Exact Sciences Laboratories (ESL) for analysis. The test works by looking for certain DNA markers and blood in the stool sample.
According to Report on Medicare Compliance from the Health Care Compliance Association (HCCA), in 2017, a gastroenterologist ordered the Cologuard kit for Rosen, the whistleblower, but Rosen chose not to return a stool sample to ESL. A few months later, ESL sent Rosen a letter offering him a $75 Visa gift card if he performed the at-home specimen collection and then returned it to ESL by March 22, 2018. Persuaded by the offer, Rosen collected a sample, returned it to ESL, and received the gift card.
As part of its Patient Compliance Program, ESL analyzed Rosen’s sample and received $499 from Medicare for performing the test. The complaint filed against Exact Sciences states Medicare paid Exact Sciences more than $160 million for a total of 334,424 Cologuard tests in 2018 while the company offered “unlawful cash equivalent inducements directly to Medicare beneficiaries,” COSMOS reported.
“It was a straight-up kickback,” Rosen’s attorney Marlan Wilbanks, JD, Senior Partner at Atlanta law firm Wilbanks and Gouinlock, told COSMOS. “You can’t offer cash or cash equivalents to anyone to induce them to use a government service.”
DOJ Elects to Not Intervene in Lawsuit
In February 2020, Exact Sciences received a civil investigation demand by the US Department of Justice (DOJ) regarding the gift card incentive. The DOJ later filed a notice that it had elected to decline intervention in the lawsuit. This action did not prevent Rosen from continuing with the lawsuit. Accordingly, in April of 2021, he filed an amended complaint against Exact Sciences alleging violations of the Federal Anti-Kickback Statute and False Claims Act.
Rosen is seeking a monetary award for himself, and on behalf of the US government, for civil penalties, treble damages, fees, and costs.
According to Report on Medicare Compliance, Exact Sciences “refuted the allegations and asserted, among other things, that the arrangement qualifies for the preventive care safe harbor to the anti-kickback statute (AKS) and that the complaint fails for many reasons.”
Exact Sciences also noted in its motion to dismiss that “encouraging a patient to have a medical service that was already ordered by a provider isn’t an inducement under the AKS.”
At this time, the case remains unresolved and continues in federal court.
DOJ Recovers Billions of Taxpayer Dollars from AKS Violations
A qui tam lawsuit or action is a method available for individuals to help the government circumvent fraud and recover money for taxpayers. Types of fraud included in these cases often pertain to Medicare and Medicaid services, defense contractor fraud, and procurement fraud.
According to the DOJ, over $1.9 billion was recovered as a result of qui tam lawsuits pursued by either the government or whistleblowers during fiscal year 2022. The number of these types of lawsuits has increased dramatically over the years with a total of 652 qui tam cases filed in 2022 alone.
Thus, clinical laboratory professionals should be aware that this type of novel scheme to generate more patients could possibly lead to legal issues. Dark Daily would like to credit Laboratory Economics for calling attention to this fascinating case of alleged illegal inducement involving a medical laboratory company.
Healthcare attorneys advise medical laboratory leaders to ensure staff understand difference between EKRA and other federal fraud laws, such as the Anti-kickback Statute
More than four years have passed since Congress passed the law and yet the Eliminating Kickbacks in Recovery Act of 2018 (EKRA) continues to cause anxiety and confusion. In particular are the differences in the safe harbors between the federal Anti-Kickback Statute (AKS) and Stark Law versus EKRA. This creates uncertainty among clinical laboratory leaders as they try to understand how these disparate federal laws affect business referrals for medical testing.
According to a news alert from Tampa Bay, Florida-based law firm, Holland and Knight, “EKRA was enacted as part of comprehensive legislation designed to address the opioid crisis and fraudulent practices occurring in the sober home industry.” However, “In the four years since EKRA’s enactment, US Department of Justice (DOJ) enforcement actions have broadened EKRA’s scope beyond reducing fraud in the addiction treatment industry to include all clinical laboratory activities, including COVID-19 testing.”
It is important that medical laboratory leaders understand this law. New cases are showing up and it would be wise for clinical laboratory managers to review their EKRA/AKS/Stark Law compliance with their legal counsels.
“Keeping in mind that [EKRA is] a criminal statute, clinical laboratories need to take steps to demonstrate that they’re not intending to break the law,” said attorney David Gee, a partner at Davis Wright Tremaine, in an exclusive interview with The Dark Report. “[Lab leaders should] think about what they can do to make their sales compensation program avoid the things the government has had such a problem with, even if they’re not sure exactly how to compensate under the language of EKRA or how they’re supposed to develop a useful incentive compensation plan when they can’t pay commissions.” David Gee will be speaking about laboratory regulations and compliance at the upcoming Executive War College in New Orleans on April 25-26, 2023. (Photo copyright: Davis Wright Tremaine.)
How Does EKRA Affect Clinical Laboratories?
The federal EKRA statute—originally enacted to address healthcare fraud in addiction treatment facilities—was “expansively drafted to also apply to clinical laboratories,” according to New York-based law firm, Epstein Becker and Green. As such, EKRA “applies to improper referrals for any ‘service,’ regardless of the payor. … public as well as private insurance plans, and even self-pay patients, fall within the reach of the statute.”
In “Revised Stark Law, Anti-Kickback Statute Rules Are Good News for Labs,” Dark Daily’s sister publication The Dark Report noted that EKRA creates criminal penalties for any individual who solicits or receives any remuneration for referring a patient to a recovery home, clinical treatment facility, or clinical laboratory, or who pays or offers any remuneration to induce a referral.
According to Epstein Becker and Green, EKRA:
Applies to clinical laboratories, not just toxicology labs.
Has relevance to all payers: Medicare, Medicaid, private insurance plans, and self-pay.
Is a criminal statute with “extreme penalties” such as 10 years in prison and $200,000 fine per occurrence.
Exceptions are not concurrent with AKS.
Areas being scrutinized include COVID-19 testing, toxicology, allergy, cardiac, and genetic tests.
“For many clinical laboratories, a single enforcement action could have a disastrous effect on their business. And unlike other healthcare fraud and abuse statutes, such as the AKA, exceptions are very limited,” Epstein Becker and Green legal experts noted.
“Therefore, a lab could potentially find itself protected under an AKS safe harbor and still potentially be in violation of EKRA,” they continued. “The US Department of Health and Human Services (HHS) and the DOJ have not provided any clarity regarding this statute (EKRA). Without this much needed guidance clinical laboratories have been left wondering what they need to do to avoid liability.”
EKRA versus AKS and Stark Law
HHS compared AKS and the Stark Law (but not EKRA) by noting on its website prohibition, penalties, exceptions, and applicable federal healthcare programs for each federal law:
AKS has criminal fines of up to $25,000 per violation and up to a five-year prison term, as well as civil penalties.
The Stark Law has civil penalties only.
AKS prohibits anyone from “offering, paying, soliciting, or receiving anything of value to induce or reward referrals or generate federal healthcare program business.”
The Stark Law addresses referrals from physicians and prohibits the doctors “from referring Medicare patients for designated health services to an entity with which the physician has a financial relationship.”
EKRA is more restrictive than AKS, as it prohibits some compensation that AKS allows, healthcare attorney Emily Johnson of McDonald Hopkins in Chicago told The Dark Report.
Recent enforcement actions may help lab leaders better understand EKRA’s reach. According to Holland and Knight:
Malena Lepetich of Belle Isle, Louisiana, owner and CEO of MedLogic LLC in Baton Rouge, was indicted in a $15 million healthcare fraud scheme for “allegedly offering to pay kickbacks for COVID-19 specimens and respiratory pathogen testing.”
In S-G Labs Hawaii, LLC v. Graves, a federal court concluded the laboratory recruiter’s contract “did not violate EKRA because the recruiter was not referring individual patients but rather marketing to doctors. According to the court, EKRA only prohibits percentage-based compensation to marketers based on direct patient referrals.”
In another federal case, United States v. Mark Schena, the court’s rule on prohibition of direct and indirect referrals of patients to clinical labs sent a strong signal “that EKRA most likely prohibits clinical laboratories from paying their marketers percentage-based compensation, regardless of whether the marketer targets doctors or prospective patients.”
What can medical laboratory leaders do to ensure compliance with the EKRA law?
In EKRA Compliance, Law and Regulations for 2023, Dallas law firm Oberheiden P.C., advised clinical laboratories (as well as recovery homes and clinical treatment facilities) to have EKRA policies and procedure in place, and to reach out to staff (employed and contracted) to build awareness of statute prohibitions and risks of non-compliance.
One other useful resource for clinical laboratory executives and pathologists with management oversight of their labs’ marketing and sales programs is the upcoming Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management. The conference takes place on April 25-26, 2023, at the Hyatt Regency in New Orleans. A panel of attorneys with deep experience in lab law and compliance will discuss issues associated with EKRA, the Anti-Kickback Statutes, and the Stark self-referral law.
Judge will decide the restitution Holmes must pay to defrauded Theranos investors at future court date; Ex-COO Ramesh “Sunny” Balwani to be sentenced next month
Clinical laboratory leaders and anatomic pathologists who closely followed the fraud trial of Elizabeth Holmes may have wondered how the Theranos founder and ex-CEO would be punished for her crimes. Now we know.
Late into the four-hour sentencing hearing, Holmes tearfully spoke, according to a twitter post by NBC reporter Scott Budman, who was in the courtroom. “I am devastated by my failings,” Holmes said. “I have felt deep pain for what people went through because I have failed them … To investors, patients, I am sorry.”
Davila ordered Holmes to surrender to authorities on April 27 to begin her time behind bars. She is free until that time. Her upcoming prison term caps off one of the biggest downfalls ever of an American entrepreneur.
Elizabeth Holmes (above), founder and former CEO of Theranos, the now defunct clinical laboratory company, as she enters the federal courthouse in San Jose, Calif., prior to her sentencing on Friday. In January, Holmes was convicted on three counts of wire fraud and one count of conspiracy. Last summer, Theranos’ former CLIA laboratory director, pathologist Adam Rosendorff, MD, expressed remorse over his testimony which led to Holmes’ defense team requesting a new trial. The judge denied that request and allowed the sentencing of Holmes to proceed as scheduled. (Photo copyright: Jim Wilson/The New York Times.)
.
Defense Lawyers Plan to Appeal
Dean Johnson, JD, a California criminal defense lawyer, told NBC Bay Area News during live coverage of the hearing on Friday that Holmes’ defense team will appeal her conviction.
“I have no doubt there will be an appeal in this case,” Johnson said.
Judge Edward Davila, who oversaw Holmes’ trial and sentencing hearing in US District Court in San Jose, Calif., estimated that the total loss for Theranos investors was $121 million. Investors had committed funds to support the company’s flawed Edison blood testing technology. A separate restitution hearing for Holmes will be scheduled for a later date.
Beyond the sentencing, Holmes, 38, will be saddled by infamy for the rest of her life, with her past reputation as a charismatic innovator ruined.
“The judge [said] evidence shows Elizabeth Holmes was leader of the company, but not necessarily the leader of the criminal acts,” Budman tweeted. Those words clearly pointed to Balwani, who Holmes’ defense team had painted as exerting control over her and the company.
Prosecutors Sought a Stiffer Sentence for Holmes
Prosecutors had asked Davila to sentence Holmes to 15 years in prison, arguing that her conviction represented “one of the most substantial white collar offenses Silicon Valley or any other district has seen,” according to NBC Bay Area News, which cited court documents. The government also wanted her to pay $803 million in restitution.
Holmes’ defense team, however, wished for no prison time at all, instead asking that Holmes serve time under house arrest. “If a period of confinement is necessary, the defense suggests that a term of 18 months or less, with a subsequent supervised release period that requires community service, will amply meet that charge,” her lawyers wrote in a court filing.
Prior to the sentencing, Davila received 130 letters supporting Holmes and asking for leniency, NPR reported. Among them was a note from William “Billy” Evans, Holmes’ partner.
“If you are to know Liz, it is to know that she is honest, humble, selfless, and kind beyond what most people have ever experienced,” Evans wrote, NPR reported. “Please let her be free.”
Holmes and Evans have a 16-month-old son together, and she is pregnant with the couple’s second child. Her first pregnancy caused her trial to be rescheduled. Prior to last week’s sentencing, some reporters covering the trial speculated that because Holmes was the mother of an infant—and now pregnant again—the judge might be more lenient in sentencing. The 11-year, four-month sentence indicates that the judge was not much influenced by that factor.
Last Minute Pitch for New Trial Failed
Holmes’ legal wranglings continued until the very end.
However, Rosendorff later told the court that he stood by his testimony about problems with Theranos’ blood testing technology.
In denying the request for a new trial, Davila wrote, “The court finds Dr. Rosendorff’s statements under oath to be credible,” according to The Washington Post.
From Teen Founder to Disgraced Entrepreneur
Holmes founded Theranos in 2003 at age 19 while she was attending Stanford University as a chemical engineering major. She dropped out of Stanford as a sophomore to focus on her new company.
Theranos claimed its technology—known as Edison—could perform diagnostics tests using a finger prick and a micro-specimen vial instead of a needle and several Vacutainers of blood. The company said it could return results to patients and clinicians in four hours for about half of the cost of typical lab test fees.
However, the promise of this technology began to unravel in 2015 following an investigative article by The Wall Street Journal that revealed the company ran only a handful of tests using its technology, instead relying on traditional testing for most of its specimen work.
Following The Journal’s exposé, the Centers for Medicare and Medicaid Services (CMS) sanctioned Theranos and Holmes in 2016. Meanwhile, the US Securities and Exchange Commission (SEC) investigated Holmes for raising hundreds of millions from investors by exaggerating or making false statements about the company’s technology and financial performance.
In 2018, the US Department of Justice (DOJ) indicted Holmes and Balwani, and Theranos closed shortly after.
Fortunately, the Theranos saga has not stunted investment in healthcare technology startups. Spending was in the tens of billions in 2021, although that number has dropped this year as the COVID-19 pandemic has waned, according to TechCrunch. Nevertheless, it is safe to assume that healthcare tech investors are scrutinizing scientific data from startups more thoroughly because of the Theranos fraud case.
Meanwhile, the saga of Theranos continues to leave a bad taste in the mouths of many clinical laboratory managers and pathologists. That’s because, during the peak period of adulation and spectacular news coverage about Elizabeth Holmes and her plans to totally disrupt the clinical laboratory industry, hospital and health system CEOs believed that they would be able to downsize their in-house medical laboratories and obtain lab tests from Theranos at savings of 50% or more. Consequently, during the years 2013 through the end of 2015, some hospital lab leaders saw requests for capital investment in their labs denied or delayed.
One example of how hospital CEOs embraced news of Theranos’ blood testing technology took place at the Cleveland Clinic. Elizabeth Holmes did such a good job selling the benefits of the Edison technology, then-CEO, Toby Cosgrove, MD, placed Theranos at number three on its list of top ten medical innovations for 2015.
In later years, Cosgrove admitted that no one at Cleveland Clinic or its pathologists were allowed to examine the analyzers and evaluate the technology.
It was for these reasons that the demise of Theranos was welcomed by many hospital lab administrators and pathologists. The fact that two of Theranos’ senior executives have been convicted of fraud validates many of the serious concerns that medical laboratory professionals had at that time, but which most major news reporters and media ignored and failed to report to the public.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
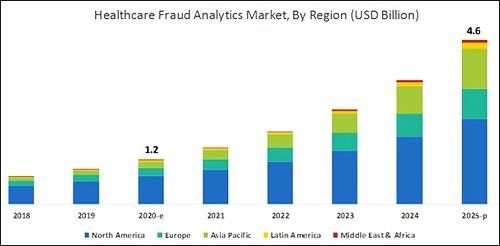
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.
Book provides detailed road map for clinical laboratory professionals who believe they have a valid case to file under the federal qui tam statute, as well as lab owners who want to understand what motivates whistleblowers and what practices to avoid
Several high-profile whistleblower cases uncovering massive fraud have shocked the clinical laboratory industry over the past decade. Media coverage nearly always focuses on the court battle and subsequent renderings of justice. But little is written about what it is like to be a whistleblower who wants to hold a medical laboratory accountable for alleged violations of federal and state laws.
Now, a new “tell-all” book penned by Chris Riedel, a whistleblower who owned a clinical laboratory company in California, details the exploits of clinical laboratory whistleblowers over the past 15 years. The intriguing white-collar crime thriller, titled, “Blood Money: One Man’s Bare-Knuckle Fight to Protect Taxpayers from Medical Fraud,” outlines Riedel’s battle with major clinical laboratory players—including the so-called “Blood Brothers” Labcorp (NYSE:LH) and Quest Diagnostics (NYSE:DGX)—to expose medical laboratory fraud.
‘Most Whistleblowers Get Absolutely Destroyed’
The book takes the reader on a gripping journey into extortion, money laundering, attempted murder, buried gold in a CEO’s backyard, fraudsters hiding money in the Cayman Islands, and, according to the author, an Assistant Attorney General sabotaging her own state’s case and a corrupt state Governor who undermined litigation by his own Attorney General.
“I wrote it to be a true crime thriller, so I’m hoping people who love thrillers will enjoy it as a true crime story,” Riedel said in an exclusive interview with Dark Daily. “For anyone who’s considering filing a whistleblower lawsuit, this is an absolute must read.
“Most whistleblowers get absolutely destroyed,” he explained. “When companies find out who’s trying to attack their business model, they do everything they can to destroy the whistleblower’s life. Many end up bankrupt, unemployable, and divorced.
“There are things you can do to protect yourself and I list those in my rules for whistleblowers. I hope enough people will read it—particularly in Congress and maybe the Department of Justice (DOJ)—to put pressure on the DOJ to change their behavior. They are far too willing to accept what they call ‘affordable civil settlements’ as opposed to punishing companies and people for their theft,” Riedel said.
Chris Riedel (above) has worked in the healthcare industry as an executive and an entrepreneur for more than 40 years. He founded five companies, including two medical laboratories and a cardiovascular disease management company. For the past 15 years, he has been tirelessly working to fight against medical companies that are defrauding US taxpayers. His actions have resulted in a court verdict and settlements totaling more than $550 million. (Photo copyright: Leadership Books.)
Riedel became a whistleblower in 2005 when he filed a case under California law that was sealed until 2009. Jerry Brown, California Attorney General at that time, joined the case and unsealed it.
Riedel had acted after his sales representatives informed him that his company, Hunter Laboratories, needed to come up with a way to compete against larger labs’ pricing to survive. Knowing the test-price-discounting practices transpiring within the lab industry in California, Riedel determined he had three choices:
Violate federal and state laws to compete,
Close his business, which would cause him to lay off more than 150 employees and lose most of his life’s savings, or
Try to stop the other companies from participating in fraudulent practices.
“It is very frustrating for honest CEOs of clinical labs to see that they cannot compete well against those lab companies employing fraudulent schemes. Rather than compete on the quality of service of their products as honest companies do, fraudsters compete based on the value of their illegal inducements,” he states on his website. “I felt the pain that many other honest CEO’s and lab owners have had to endure as they try to compete with fraud and watch their life’s work destroyed.”
He chose to try leveling the playing field for all labs and stop taxpayers from being fleeced. After filing that first whistleblower lawsuit in California in 2005, he later filed similar whistleblower lawsuits in other states that had statutes defining how labs were to price lab tests for their Medicaid programs.
Riedel encountered many roadblocks and frustrations during the initial lawsuit, including some genuinely frightening moments. He described one such experience for Dark Daily.
“Quest and Labcorp together went to Blue Shield of California, a major insurance company, and they got our clinical lab kicked out of network. They offered Blue Shield a 10% discount on all their laboratory testing if they would kick Hunter Laboratories out of network,” Riedel explained. “Since [Quest and Labcorp] represented about 70% to 80% of the total outpatient laboratory testing for Blue Shield, it was too good for this insurer to pass up.
“When your lab loses a major insurance carrier like that, you can’t survive. What doctor is going to want to start with a clinical lab that doesn’t have Blue Shield? And existing clients don’t want to subject their patients to having much higher out-of-pocket expenses.
“From that point on, it was like a dagger in our heart,” he added. “We were literally two weeks away from both corporate and personal bankruptcy when we reached our historic settlement with Quest. Had it not been for that settlement, our 150 employees would have lost their jobs, we would have lost our house, and we would have been completely bankrupt. That was very scary, and I had a very hard time dealing with it.”
Uncovering Medical Laboratory Fraud
While performing his research for the whistleblower case, Riedel was astonished by the information and fraud he discovered.
“There was one point where we had to prove that Quest and Labcorp were passing out discounts to some clients that were at or below cost, without giving those same prices to the Medi-Cal program, as required by state law at that time,” Riedel explained. “I personally reviewed over a million documents. It took more than five years, but it was worth it.
“I eventually found three documents that exposed the complete fraud by Quest. These documents showed what Quest had billed Medi-Cal, how much money the company lost client billing and capitation contracts, and how much business they ‘pulled through’ from the government and insurance payers that made up for the staggering losses on deeply discounted client and capitated billing. That was like the silver bullet.”
In the process, Riedel also discovered what it was like to work with the federal Department of Justice.
“The DOJ hates people who file more than one whistleblower lawsuit,” he added. “They don’t like the statute to begin with, and they barely tolerate whistleblowers, so when they find someone who does it time and again, they really don’t like it.”
“Blood Money” (above) contains practical advice and suggestions that are useful for both clinical laboratory executives and pathologists who want to keep their lab operations compliant with federal law, thus not giving whistleblowers any issues to pursue a qui tam lawsuit, as well as lab whistleblowers who observe violations within their clinical labs—or at competing labs—and who want to do something that may rectify the situation. (Photo copyright: Chris Riedel.)
Riedel is considering writing a second book and is trying to decide which qui tam lawsuits will provide the best subject matter.
“I am currently investigating what would be a multi-billion-dollar lawsuit against an insurance company and that is going to be, by far, the biggest of the cases I have ever been involved in. That might make a good book all by itself,” he said.
Riedel finds his work fighting fraud against the government rewarding and plans to continue his efforts in the future.
“Even though it’s risky—and the book details how my life was almost destroyed when the Blood Brothers counter attacked—I enjoy the investigative work and legal challenges. For me, it is very fulfilling, and I am proud to carry the torch for taxpayers,” he says in a statement on his website.
The 368-page book should be of interest to clinical laboratory personnel, healthcare professionals, those considering becoming a whistleblower, and basically anyone involved in medical laboratory testing.