Trifecta of forces at work that will affect the clinical laboratory and pathology industries have been described as a ‘perfect storm’ requiring lab and practice managers to be well informed
Digital pathology, artificial intelligence (AI) in healthcare, and the perfect storm of changing federal regulations, took centerstage at the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management in New Orleans this week, where more than 1,000 clinical laboratory and pathology leaders convened over three days.
This was the largest number of people ever onsite for what has become the world’s largest event focused exclusively on lab management topics and solutions. Perhaps the highlight of the week was the federal Food and Drug Administration’s (FDA’s) announcement of its final rule on Laboratory Developed Tests (LDTs). Overall, the conference featured more than 120 speakers, many of them national thought leaders on the topic of clinical lab and pathology management. More than 65% of the audience onsite were executive level lab managers.
“The level of interest in the annual Executive War College is testimony to the ongoing need for dynamic, engaging, and highly relevant conference events,” said Robert Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “These in-person gatherings present great opportunities for clinical laboratory and pathology managers and leaders to network and speak with people they otherwise might not meet.” (Photo copyright: Dark Intelligence Group.)
Demonstrating Clinical Value
For those who missed the action onsite, the following is a synopsis of the highlights this week.
Lâle White, Executive Chair and CEO of XiFin, spoke about the future of clinical laboratory testing and the factors reshaping the industry. There are multiple dynamics impacting healthcare economics and outcomes—namely rising costs, decreasing reimbursements, and the move to a more consumer-focused healthcare. But it is up to labs, she said, to ensure their services are not simply viewed as a commodity.
“Laboratory diagnostics have the potential to change the economics of healthcare by really gaining efficiencies,” she noted. “And it’s up to labs to demonstrate clinical value by helping physicians manage two key diagnostic decision points—what tests to order, and what to do with the results.”
But even as labs find ways to increase the value offered to clinicians, there are other disruptive factors in play. Consumer-oriented tech companies such as Google, Apple, and Amazon are democratizing access to patient data in unforeseen ways, and Medicare Advantage plans are changing the way claims are processed and paid.
Clinical labs are fundamental components of the public health infrastructure. So, the CDC plans on focusing on delivering high-quality laboratory science, supported by reliable diagnostics and informatics for disease outbreaks and exposures, and engaging with public and private sector partners.
The history of MolDX and Z-Codes were the topics discussed by Gabriel Bien-Willner, MD, PhD, Chief Medical Officer for healthcare claims and transaction processing company Palmetto GBA. Molecular testing is highly complex, and the lack of well-defined billing codes and standardization makes it difficult to know if a given test is reasonable and necessary.
Z-Codes were established to clarify what molecular testing was performed—and why—prompting payers to require both Z-Codes and Current Procedural Terminology (CPT) codes when processing molecular test claims. Medicare’s MolDX program further streamlines the claims process by utilizing expertise in the molecular diagnostics space to help payers develop coverage policies and reimbursement for these tests.
FDA Final Rule on LDT Regulation
Timothy Stenzel, MD, PhD, CEO of Grey Haven Consulting and former director of the FDA’s Office of In Vitro Diagnostics reviewed the latest updates from the FDA’s Final Rule on LDT (laboratory developed test) regulation. Prior to the FDA releasing its final rule, some experts suggested that the new regulations could result in up to 90% of labs discontinuing their LDT programs, impacting innovation, and patient care.
However, the final rule on LDTs is very different from the original proposed rule which created controversy. The final rule actually lowers the regulatory burden to the point that some labs may not have to submit their LDTs at all. The FDA is reviewing dozens of multi-cancer detection assays, some of which have launched clinically as LDTs. The agency is likely to approve those that accurately detect cancers for which there is no formal screening program.
Stenzel explained the FDA’s plan to down-classify most in vitro diagnostic tests, changing them from Class III to Class II, and exempting more than 1,000 assays from FDA review. He also discussed the highlights of the Quality Management System Regulation (QMSR). Launched in January, the QMSR bought FDA requirements in line with ISO 13485, making compliance easier for medical device manufacturers and test developers working internationally.
Looming Perfect Storm of Regulatory Changes
To close out Day 1, Michel took to the stage again with a warning to clinical laboratories about the looming “Perfect Storm” trifecta—the final FDA ruling on LDTs, Z-Code requirements for genetic testing, and updates to CLIA ’92 that could result in patient data being considered a specimen.
Laboratory leaders must think strategically if their labs are to survive the fallout, because the financial stress felt by labs in recent years will only be exacerbated by macroeconomic trends such as:
Staff shortages,
Rising costs,
Decreasing and delayed reimbursements, and
Tightening supply chains.
Lab administrators looking for ways to remain profitable and prosperous should look beyond the transactional Clinical Lab 1.0 fee-for-service model and adopt Clinical Lab 2.0, which embraces HEDIS (Healthcare Effectiveness Data and Information Set) scores and STAR ratings to offer more value to Medicare Advantage and other payers.
Wednesday’s General Session agenda was packed with information about the rise of artificial intelligence, big data, and precision medicine in healthcare. Taking centerstage on the program’s final day was Michael Simpson, President and CEO of Clinisys. Simpson gave a global perspective on healthcare data as the new driver of innovation in diagnostics and patient care.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
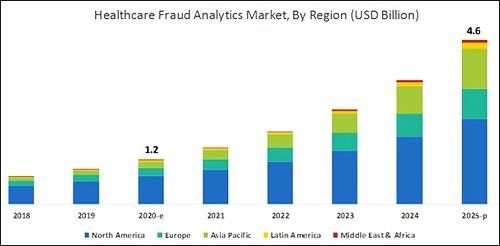
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.
Confusion, unhappiness, and many unresolved issues remain about the way government and private payers are handling claims for molecular diagnostic tests covered by the 114 new CPT codes
Dust is settling from the fiasco triggered by the Medicare program’s failure to be ready on January 1, 2013, to settle molecular diagnostic test claims filed under the 114 new Tier 1 and Tier 2 molecular CPT codes. The damage is not just limited to Medicare test claims, but also involves private health plans that were waiting to let the Medicare program set precedents on coverage and prices for the new molecular test codes.
Many Clinical Laboratories Must Cope With an Unsatisfactory Situation
Although federal Medicare officials and Medicare contractors have scrambled to rectify the situation, even today there is much unhappiness across the clinical laboratory industry about the current state of things. That unhappiness extends to state Medicaid and private payers because many of these payers have been slow to publish coverage guidelines and prices for these new molecular test CPT codes.