In a letter, Congress urged the HHS Secretary to conduct “vigorous oversight and enforces full compliance with the final rule”
Analysis of more than 3,100 hospital websites by The Wall Street Journal (WSJ) has found “hundreds” containing embedded code that prevents search engines from displaying the hospitals’ prices. This is contrary to the Hospital Price Transparency Final Rule (84 FR 65524), passed in November 2019, which requires hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices.
“Hundreds of hospitals embed code in their websites that prevented Alphabet Inc.’s Google and other search engines from displaying pages with the price lists,” the WSJ reported. “Among websites where [the WSJ] found the blocking code were those for some of the biggest US healthcare systems and some of the largest hospitals in cities including New York and Philadelphia.”
Additionally, the WSJ found hospitals were finding ways to “hide” the price lists they did display deep within their websites. The prices can be found, but the effort involves “clicking through multiple layers of pages,” on the providers’ websites, the WSJ added.
Lawmakers Put Pressure on CMS
The WSJ report drew the attention of federal lawmakers who weighed in on the current state of hospital price transparency and on the WSJ’s findings in a letter to Xavier Becerra, Secretary of the federal Department Health and Human Services (HHS).
In their letter, members of the Congressional Committee on Energy and Commerce called for HHS “to revisit its enforcement tools, including the amount of civil penalty, and to conduct regular audits of hospitals for compliance.”
Committee members wrote, “The Hospital Price Transparency Final Rule requires hospitals to make public a machine-readable file containing a list of all standard charges for all items and services and to display charges for the hospital’s 300 most ‘shoppable’ services in a consumer-friendly format. We are concerned about troubling reports of some hospitals either acting slowly to comply with the requirements of the final rule or not taking any action to date to comply.”
The letter, which was signed by the committee’s Chairman Frank Pallone (D, New Jersey) and Committee Ranking Member Cathy McMorris Rodgers (R, Washington State), cited the WSJ investigation as well as other analyses of price transparency at US hospitals.
Cynthia Fisher (above), founder of Patient Rights Advocate, told The Wall Street Journal, “In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the healthcare system.” Now, Fisher added, “it’s the American consumer who is going to drive down the cost of care.” Clinical laboratories will note that consumer demand for, and federal regulation of, price transparency is not limited to hospitals. All healthcare providers need procedures in place that comply with federal guidelines for transparency. (Photo copyright: Morning Consult.)
Additional Studies Show Major Hospitals “Non-Compliant”
One such study cited by the Congressional committee in its letter to HHS was conducted by Health Affairs, which looked into transparency compliance at 100 hospitals. In a blog post, titled, “Low Compliance from Big Hospitals on CMS’s Hospital Price Transparency Rule,” the study authors wrote “our findings were not encouraging: Of the 100 hospitals in our sample, 65 were unambiguously noncompliant.
“Of these 65,” they added:
“12/65 (18%) did not post any files or provided links to searchable databases that were not downloadable.
“53/65 (82%) either did not include the payer-specific negotiated rates with the name of payer and plan clearly associated with the charges (n = 46) or were in some other way noncompliant (n = 7).
“We are troubled by the finding that 65 of the nation’s 100 largest hospitals are clearly noncompliant with this regulation. These hospitals are industry leaders and may be setting the industrywide standard for (non)compliance; moreover, our assessment strategy was purposefully conservative, and our estimate of 65% noncompliance is almost certainly an underestimate,” Health Affairs concluded.
A previous similar investigation by The Washington Post called compliance by hospitals with the pricing disclosure rules “spotty.”
So, why is complying with the federal price transparency rule so challenging for the nation’s largest hospitals? In its reporting on the Wall Street Journal analysis, Gizmodo wrote, “we’ve seen healthcare providers struggle to implement the new law due, in part, to how damn ambiguous it is. Past reports have pointed out that the vague requirements hoisted onto hospitals as part of these new rules often result in these pricing lists being difficult—if not downright—impossible to find, even if the lists are technically ‘machine-readable’ and ‘on the internet.’”
“Meanwhile,” Gizmodo continued, “as [the WSJ] points out, the order doesn’t specify exactly how much detail these hospitals are even supposed to offer on their pricing sheets—meaning that it’s up to the hospitals whether they want to include rates pertaining to specific health insurance plans, or whether they want to simply include different plan’s rates in aggregate.”
And in their letter to HHS, the Congressional committee wrote, “… some hospitals are providing consumers a price estimator tool instead of providing the full list of charges and payer-negotiated rates in one file, and some are making consumers fill out lengthy forms for estimates. Some hospitals also are providing the data in a non-useable format or failing to provide the codes for items and services.”
Clinical Laboratories Must Comply with Price Transparency Rules
Clearly, transparency in healthcare has a long way to go. Nevertheless, hospital medical laboratory leaders should expect reinforcing guidance from CMS on making price information on commonly used clinical laboratory tests fully accessible, understandable, and downloadable.
As Dark Daily noted in previous coverage, consumer demand for price transparency is only expected to increase. Clinical laboratories need to have a strategy and process for helping consumers and patients see test prices in advance of service.
Oddly, as upcoding severity levels have risen, reported higher-severity inpatient hospital stays have dropped, OIG reported
Medicare upcoding fraud is a growing problem for the federal Centers for Medicare and Medicaid Services (CMS). Now, a report from the US Department of Health and Human Services (HHS) Office of Inspector General (OIG) suggests that the practice is increasingly occurring for high-severity inpatient hospital stays that account for the most expensive part of US healthcare.
“The [COVID-19] pandemic has placed unprecedented stress on the country’s healthcare system, making it more important than ever to ensure that Medicare dollars are spent appropriately,” the OIG report states.
The OIG website notes, “Medicare pays for many physician services using Evaluation and Management (commonly referred to as “E/M”) codes. New patient visits generally require more time than follow-up visits for established patients, and therefore E/M codes for new patients command higher reimbursement rates than E/M codes for established patients.”
The OIG describes one type of upcoding as “… an instance when [providers] provide a follow-up office visit or follow-up inpatient consultation, but bill using a higher-level E/M code as if [they] had provided a comprehensive new patient office visit or an initial inpatient consultation.
“Another example of upcoding related to E/M codes is misuse of Modifier 25,” the OIG continued. “Modifier 25 allows additional payment for a separate E/M service rendered on the same day as a procedure. Upcoding occurs if a provider uses Modifier 25 to claim payment for an E/M service when the patient care rendered was not significant, was not separately identifiable, and was not above and beyond the care usually associated with the procedure.”
How OIG Conducted the Study of Hospital Coding Practices
To perform its research, the OIG analyzed Medicare Part A claims for hospital stays for the six-year period from fiscal year (FY) 2014 through FY 2019. The OIG identified trends in billing and payments for inpatient hospital stays at the highest severity levels, as determined by the Medicare Severity Diagnosis Related Group (MS-DRG).
The OIG investigation revealed that the number of hospital stays billed at the highest severity level increased almost 20% between 2014 and 2019, while the number of stays billed at other severity levels decreased. These expenditures accounted for nearly half of all Medicare spending on inpatient hospital stays, the OIG reported.
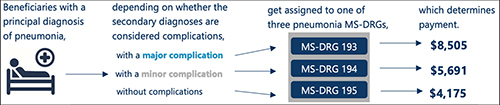
According to the OIG report, “Medicare pays hospitals more for beneficiaries in MS-DRGs with higher severity levels because they are typically more costly to treat.” The graphic above taken from the OIG report illustrates “how the presence of complications can affect Medicare payment for three beneficiaries with the same principal diagnosis.” (Graphic copyright: Federal Office of Inspector General Department of Health and Human Services.)
As Severity Levels Went Up, Inpatient Length of Stays Went Down
Interestingly, the average length of inpatient stays at the highest severity level decreased, and the average length of hospital stays overall remained largely the same, decreasing by just 0.1 days. In addition, the total number of inpatient hospital stays decreased by 5%.
The OIG report noted that “the increase in the number of stays billed at the highest severity level implies that beneficiaries were sicker overall. However, the decrease in the average length of stays at the highest severity level potentially undermines that idea because it is not consistent with sicker beneficiaries. Length of stay generally has a positive relationship to severity of stay; sicker beneficiaries stay in the hospital longer.”
The OIG confirmed that in FY 2019, Medicare spent $109.8 billion for 8.7 million hospital stays. Approximately 3.5 million (or 40%) of those stays were billed at the highest severity level, as determined by the MS-DRG. In addition, nearly half of the $109.8 billion spent, or $54.6 billion, was for stays billed at the highest severity level and Medicare paid an average of $15,500 per stay at that level.
The OIG report states that “stays at the highest severity level are vulnerable to inappropriate billing practices, such as upcoding—the practice of billing at a level that is higher than warranted. Specifically, nearly a third of these stays lasted a particularly short amount of time and over half of the stays billed at the highest severity level had only one diagnosis qualifying them for payment at that level. Further, hospitals varied significantly in their billing of these stays, with some billing much differently than most.”
The OIG study also found that over half of the inpatient stays billed at the highest severity level achieved that level due to only one diagnosis. According to the OIG, the severity of an inpatient stay depends on a patient’s secondary diagnosis and it only takes one secondary diagnosis to propel a patient into the highest severity level. The OIG determined that if the diagnosis was inaccurate or inappropriate, higher payments would not be warranted.
OIG Recommends CMS Conduct Targeted Reviews
The report found that the most frequently billed MS-DRG in FY 2019 was septicemia or severe sepsis and that hospitals billed for 581,000 of these stays, for which Medicare paid $7.4 billion. In addition, kidney and urinary tract infections, pneumonia, and renal failure were among the most common conditions to have a complication that led to a high severity classification.
In its report, the OIG recommended more oversight from CMS to ensure that Medicare dollars are spent appropriately. The OIG also suggests that CMS conduct targeted reviews of MS-DRGs and hospital stays that are vulnerable to upcoding, as well as the hospitals that frequently bill them.
Clinical Laboratories Are Forewarned
Medicare audits continue to be more detailed and rigorous and all healthcare providers—including clinical laboratories and anatomic pathology groups—should be prepared to present all necessary documentation to support claims if and when they are audited.
Improvements in software, machine learning, and artificial intelligence (AI) give Medicare officials and the OIG powerful tools to spot questionable provider billing. This includes medical laboratories whose billing patterns could arouse suspicions and trigger audits.
Upcoding is a long-standing problem for the Medicare program. What is changing is that federal officials now have better tools and resources to use in identifying patterns of upcoding that fall outside accepted parameters.
Medical laboratories gain competitive advantage by using GPS and real-time vehicle tracking to improve performance of their couriers
Like everything else in laboratory medicine, even such once-simple operational areas as logistics and courier services are becoming complicated—and more expensive. The reasons are familiar to all clinical laboratory managers and pathologists.
For example, sophisticated new diagnostic technologies require that specimens be transported with greater care to ensure that they arrive at the medical laboratory with full integrity. (more…)
Obamacare reforms scheduled for 2014 may have negative financial impact for pathology groups and clinical laboratories
It was not welcome news to many healthcare policymakers when McKinsey & Company released the findings of a survey that indicated that as many as 30% of employers were likely to cease offering health insurance coverage to employees when certain mandates of the Affordable Care Act (ACA) take effect in 2014. Criticism of the McKinsey study was swift, and newspapers and television news outlets gave wide coverage to these criticisms.
For pathologists and clinical laboratory managers, this dust-up over the findings of the McKinsey survey of major employers provides a clue as to the more rancorous debates that are yet to come as, year by year, different mandates of the Obamacare law take effect. The details of McKinsey’s survey about how employers are likely to handle employee health insurance coverage are an example of such debates.
Clinical Laboratory Actions Should Be Listed in the HIPDB
The HIPDB is a national database of adverse actions taken by federal agencies against “healthcare practitioners, providers and suppliers,” who are defined in the OIG report as medical doctors, laboratories, clinics, nursing homes, managed care facilities, prescription drug plans and durable medical equipment (DME) suppliers.