Organizations representing clinical laboratories and other critical healthcare providers urged Congress to pass the Saving Access to Laboratory Services Act by January 1, 2023, to prevent deep cuts in reimbursements
Lessons about the essential role of clinical laboratories during a pandemic was the central theme in a significant publication released recently. The authors were the presidents of two of the nation’s largest healthcare companies and their goal was to connect the value clinical labs delivered during the COVID-19 pandemic to the financial threat labs face should the Protecting Access to Medicare Act of 2014 (PAMA) fee cuts coming to the Medicare Part B Clinical Laboratory Fee Schedule (CLFS) be implemented.
In an article for RealClearPolicy, healthcare executives William G. Morice II, MD, PhD (left), CEO/President, Mayo Clinic Laboratories, and Matt Sause (right), President of Roche Diagnostics North America wrote, “Without PAMA reform, labs could face drastically reduced reimbursement for commonly performed lab tests for a host of diseases.” (Photo copyrights: Mayo Clinic Laboratories/Roche Diagnostics.)
IVD Companies and Clinical Laboratories Sound Alarm
Morice and Sause warn that—without PAMA reform—the nation’s vital medical laboratories will face “drastically reduced reimbursement” for commonly performed lab tests for diseases, including diabetes, heart disease, and cancer. Reimbursement cuts may cause clinical labs serving “the most vulnerable and homebound” to reduce services or close, they noted.
“To emerge from nearly three years of a pandemic by sending the signal that austerity is our nation’s health policy when it comes to testing and diagnostics would be a significant mistake,” they wrote.
“If the proposed cuts to reimbursements for diagnostic tests are allowed to take effect, disparities caused by challenges with accessing diagnostic tests will likely grow even further,” the authors continued.
However, they added, “The Saving Access to Laboratory Services Act [SALSA] would reform PAMA to require accurate and representative data from all laboratory segments that serve Medicare beneficiaries to be collected to support a commonsense Medicare fee schedule that truly represents the market.”
How PAMA Affects Clinical Laboratory Reimbursements
PAMA, which became law in 2014, was aimed at marrying Medicare Part B Clinical Laboratory Fee Schedule (CLFS) reimbursement rates to rates medical laboratories receive from private payers, the National Independent Laboratory Association (NILA) explained in a news release.
But from the start, in its implementation of the PAMA statute, the methods used by the federal Centers for Medicare and Medicaid Services (CMS) to collect data on lab test prices paid by private payers—which were the basis for calculating new lab test prices for the Medicare program—were criticized by many laboratory professionals and other health experts.
Critics frequently pointed out that several types of clinical laboratories were excluded from reporting their private payer lab test prices. Thus, the data collected and used by CMS did not accurately represent the true range of prices paid for clinical lab tests by private health insurance plans, said lab industry groups.
CMS regulations “exclude most hospital outreach laboratories and physician office laboratories from data collection. This approach depresses median prices and has led to deep cuts to lab reimbursement. Many tests were cut up to 30% in 2018 when the new system went into effect,” the America Association for Clinical Chemistry (AACC) noted in a statement.
On September 8, just weeks after publication of the article authored by Morice and Sause, 26 organizations representing clinical laboratories and diagnostics manufacturers sent a letter to Congressional leaders. In it they described the financial impact on labs due to the current law’s omission of some outreach and physician office lab testing, and they urged the passage of the SALSA legislation.
“The significant under-sampling led to nearly $4 billion in cuts to those labs providing the most commonly ordered test services for Medicare beneficiaries,” the organizations wrote in their letter. “For context, the total CLFS spend for 2020 was only $8 billion.”
Reimbursement Cuts to Lab Tests are Coming if SASLA Not Passed
“Without Congressional action, beginning on Jan. 1, 2023, laboratories will face additional cuts of as much as 15% to some of the most commonly ordered laboratory tests,” the NILA said.
“Enactment of the Saving Access to Laboratory Services Act (SALSA/H.R. 8188/S.4449) is urgently needed this year, to allow laboratories to focus on providing timely, high quality clinical laboratory services for patients, continuing to innovate, and building the infrastructure necessary to protect the public health,” NILA added.
In an editorial she wrote for Clinical Lab Products, titled, “Be a Labvocate: Help Pass SALSA Legislation,” Kristina Martin, Clinical Pathology Operations Director, Department of Pathology, University of Michigan Medicine said, “The SALSA legislation provides a permanent, pragmatic approach to evaluating the CLFS, eliminating huge swings, either positive or negative as it pertains to Medicare reimbursement. It also allows for a more comprehensive evaluation of data to be collected from a broader sampling of laboratory sectors.”
Uses statistical sampling for widely available tests performed by a “representative pool of all clinical laboratory market segments.”
Introduces annual “guardrails” aimed at creating limits for reductions as well as increases in CLFS rates.
Excludes Medicaid managed care rates since they are not true “market rates.”
Gives labs the option to exclude mailed remittances from reporting if less than 10% of claims.
Eases clinical labs’ reporting requirements by changing data collection from three years to four.
Make Your Views Known
Proponents urge Congress to act on SALSA before the end of the year. Clinical laboratory leaders and pathologists who want to express their views on SALSA, test reimbursement, and the importance of access to medical laboratory testing can do so through Stop Lab Cuts.org. The website is sponsored by the ACLA.
In their letter, the Representatives wrote, “As you are aware, the recently enacted Paycheck Protection Program and Health Care Enhancement Act (PPPHCE Act) invests $25 billion in the [Public Health and Social Services Emergency Fund (PHSSEF)], including $11 billion for states, localities, territories, and tribes, to enhance all aspects of COVID-19 testing capacity. This funding is in addition to the funds already appropriated to the PHSSEF under the CARES Act.
“While laboratories are eligible, along with other providers, for these funds,” they continued, “there have been no federal funds specifically designated for the laboratories that have stepped up in this public health crisis and have made significant investments to expand access to COVID-19 testing despite 40-60 percent reductions in regular commercial volume due to the economic lockdowns.
“As laboratories work to maintain their investments in critical resources for testing platforms, reagents, swabs, and PPE, as well as hiring, training, and overtime pay for the laboratory workforce, we urge HHS to direct a portion of funding that has not already been allocated towards these efforts. These funds will ensure that labs can continue to rapidly scale up diagnostic and antibody testing, particularly for healthcare workers, first responders, and other Americans on the frontlines of this pandemic,” concluded the Representatives.
ACLA President Made Similar Plea for Direct Funding to Clinical Laboratories
“In order to deliver accurate, reliable results for patients at a national scale, we must allocate funding to support [clinical laboratories’] expanded efforts,” she said in a statement following an April 27 meeting at the White House.
In her letter, Khani wrote, “It is essential that HHS allocate $10 billion from the fund to support labs’ further expansion of testing capacity to fulfill the testing needs of all of the states and to protect the lives and livelihood of all Americans.
“Further,” she continued, “HHS should note that investing in the nation’s laboratories will not only enhance testing capacity in the short-term, but it also will allow the country to benefit from a robust testing infrastructure for the duration of the COVID-19 pandemic and beyond.”
President Trump signed H.R.266 into law on April 24. It includes $25 billion earmarked for research, development, validation, manufacturing, purchasing, administering, and expanding capacity for COVID-19 testing. According to the language of H.R.266, that includes, “tests for both active infection and prior exposure, including molecular, antigen, and serological tests, the manufacturing, procurement and distribution of tests, testing equipment and testing supplies, including personal protective equipment needed for administering tests, the development and validation of rapid, molecular point-of-care tests, and other tests, support for workforce, epidemiology, to scale up academic, commercial, public health, and hospital laboratories, to conduct surveillance and contact tracing, support development of COVID-19 testing plans, and other related activities related to COVID-19 testing.”
“As the demand for testing continues to grow, clinical laboratories need dedicated funding to plan for challenges that lie ahead. Strong federal coordination and leadership is essential, and we’re looking forward to working with HHS to ensure that laboratories have the resources necessary to continue to expand our role at the forefront of the nation’s response,” said Julie Khani (above), President of the American Clinical Laboratory Association (ACLA), in a press release following the June 8 letter sent to HHS by 30 members of Congress requesting funds from H.R.266 be sent directly to clinical laboratories. Khani will be speaking on federal policies now impacting clinical laboratories at the upcoming 25th annual Executive War College on Laboratory and Pathology Management in New Orleans on July 14-15. (Photo copyright: ACLA.)
Financial Struggles for Hospitals and Clinical Laboratories
This new round of stimulus funding comes at a time when many providers and clinical laboratories are struggling financially, despite the influx of COVID-19 patients.
“Across the country, laboratories have made significant investments to expand capacity, including purchasing new platforms, retraining staff, and managing the skyrocketing cost of supplies. To continue to make these investments and expand patient access to high-quality testing in every community, laboratories will need designated resources. Without sustainable funding, we cannot achieve sustainable testing,” said Khani in an ACLA statement.
As the COVID-19 coronavirus pandemic evolves, federal regulations, as well as emergency funding for COVID-19 testing that is provided by federal legislation, will evolve in unexpected ways. For that reason, clinical laboratory leaders will want to closely track announcements by such federal agencies as the Department of Health and Human Services, the Centers for Medicare and Medicaid Services, the Food and Drug Administration, the Centers for Disease Control and Prevention, and the Federal Emergency Management Administration as decisions are made about how to assign the $25 billion authorized in H.R.266 for “testing.”
Limited availability of COVID-19 clinical lab tests is major topic at federal briefings and news stories, yet many of nation’s labs are laying off staff and at point of closing
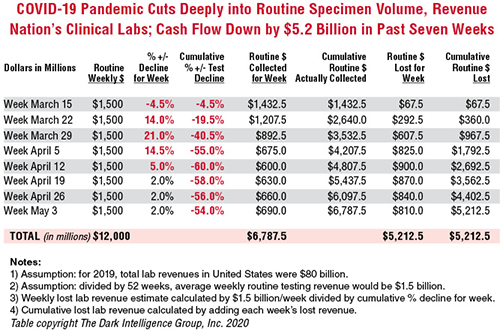
Cash flow at the nation’s clinical laboratories has crashed, with revenues down by more than $5 billion since early March. This is the biggest financial disaster for the nation’s clinical laboratory industry in its 100-year history and it couldn’t come at a worse time for the American public and the US healthcare system.
At the precise moment when the nation needs clinical laboratories to begin performing millions of tests for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, those same labs are watching their cash flow collapse.
Data from multiple sources gathered by The Dark Report, sister publication of Dark Daily, confirm that—beginning in early March and continuing through last week—clinical laboratories in the United States saw incoming flows of routine specimens decline by between 50% and 60%. During this same time, lab revenue fell by similar amounts.
Clinical Lab Industry Currently Losing $800 to $900 Million Weekly
To give this decline context, the healthcare system spends about $80 billion annually on medical laboratory testing. Thus, labs across the US generated about $1.5 billion in revenue each week during 2019 and into 2020. By April 5, the decline in routine lab specimen volumes reached 55% to 60%. Since then, the clinical lab industry now loses between $800 million and $900 million each week. Total revenue loss from previous levels is already estimated to be $5.2 billion, and it is growing by an additional $800 million to $900 million every week that patients stay away from hospitals and physicians’ offices.
In the eight weeks since the COVID-19 pandemic caused patients to cease coming to hospitals and visiting their doctors, incoming routine specimens and revenue fell by 60%, causing cumulative lost routine revenue of $5.2 billion for the clinical laboratory industry in the United States. Each week that the existing shelter-in-place directives are effective, labs lose another $800 million to $900 million. The Dark Report based these estimates on data provided by multiple companies working with lab billing/claims, middleware analytical solutions, and customer relationship management (CRM) and electronic health record (EHR) products. (Chart copyright: The Dark Intelligence Group, Inc.)
The recent dire financial condition of labs small and large has gone unremarked by federal healthcare officials at the daily White House COVID-19 Task Force briefings. National news sources have yet to report on this development and its implications for successfully expanding the availability and numbers of COVID-19 tests in response to the pandemic.
The rapid and deep decline in specimens and revenue is not limited to clinical laboratories. Biopsy cases referred to anatomic pathology groups have declined by 50% to 60%. Some subspecialty pathology labs saw case referrals drop by 80% or more.
The nation’s two biggest clinical laboratory companies confirmed similar declines in their normal daily flow of routine specimens. Both companies recently reported first-quarter earnings (which included the month of March).
Quest Diagnostics, LabCorp Each Disclose Volume Declines of 50% to 60%
During its Q1 2020 earnings conference call, Chairman, President, and CEO of Quest Diagnostics (NYSE:DGX), Steve Rusckowski, stated, “In April, volume declines continue to intensify as we are seeing signs that volume declines are bottoming out at around 50% to 60%.”
The drop-off in routine lab test referrals was the similar at LabCorp (NYSE:LH). “In our diagnostics business, at the end of the quarter, we experienced reductions in demand for testing of 50% to 55% versus the company’s normal daily levels,” explained Glenn Eisenberg, Executive Vice President and CFO during LabCorp’s Q1 2020 earnings call. “This reduction in demand impacted testing volume broadly but was more heavily weighted towards routine procedures.”
Interviews with independent clinical lab owners and the administrative directors of hospital and health system labs further confirm this rapid and dramatic decline in the number of routine specimens arriving in their labs. Fewer specimens mean fewer claims, which means less revenue to laboratories.
Two Different Financial Futures for ‘Have’ Labs and ‘Have Not’ Labs
What happens next to the clinical laboratory industry in the United States—and to its ability to continue ramping up the availability of adequate numbers of COVID-19 tests in major cities, small towns, and rural areas—will be a story of “haves” and “have nots.”
The “haves” are clinical labs that have access to money. These are publicly-traded lab companies, academic medical center labs, and the sophisticated labs of health networks that operate multiple hospitals. In each case, these organizations have capital reserves and access to loans that will probably enable them to sustain COVID-19 lab testing services at the large volumes required to respond to the pandemic.
clinical labs operated by community hospitals and rural hospitals that were not financially robust before the onset of the pandemic; and,
specialty lab companies that perform a specific number of proprietary diagnostic tests (and for which demand has collapsed as patients stopped seeing their doctors).
Medicare Led Payers in the ‘Lab Test Price Race to the Bottom’
Prior to the onset of the SARS-CoV-2 pandemic, the finances of the “have-not” labs were already shaky, with many on the verge of filing bankruptcy, closing, or selling to a bigger lab company. Much blame for the deteriorating finances at a large proportion of community lab companies, community hospital labs, and rural hospital labs can be attributed to the deep, multi-year price cuts to the Medicare Part B clinical laboratory fee schedule as mandated by the Protecting Access to Medicare Act of 2014 (PAMA).
Medicare’s multi-year cuts to lab test prices were immediately copied by most state Medicaid programs. During this period, private payers followed Medicare’s lead and enacted their own deep cuts to the prices they paid labs for both routine tests and molecular/genetic tests.
That is why—when the pandemic intensified in early March—the 50% to 60% drop in specimens and revenue that hit these labs starved them of essential cash flow. When polled, the owners and directors of these labs acknowledge layoffs of the majority of their staff in all departments. They also reported substantial delays—both in submitted lab test claims and in getting payment for those claims—because claims-processing departments at the labs and private health insurers are understaffed due to shelter-in-place directives.
COVID-19 Test Revenue Helps Only Labs Performing Those Tests
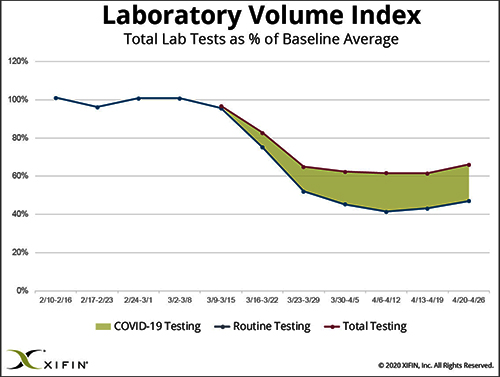
Revenue from COVID-19 testing is helping certain labs offset the revenue loss from fewer routine specimens. XIFIN, Inc., a San Diego company that provides revenue cycle management (RCM) services for clinical laboratories and pathology groups, analyzed the lab test claims for COVID-19 rapid molecular tests. It determined that labs performing these tests are generating enough revenue from these test claims to equal about 20% of their pre-pandemic revenue.
The chart above was prepared by XIFIN, Inc., of San Diego and is based on the changes XIFIN observed in the volume of routine clinical laboratory test claims generated by client labs on a weekly basis. In the first two months of 2020, routine lab test claims ran at expected levels until the first week of March. During the rest of March, routine lab test claims declined by 60%. During April, incoming routine lab test claims remained 55% to 60% below pre-pandemic levels. The shaded area shows the number of COVID-19 test claims coming into clinical labs. XIFIN says COVID-19 test claims make up about 20% of the decline in routine test specimens for those labs performing COVID-19 tests. The Dark Report estimates that the clinical laboratory industry has lost $800 million to $900 million in routine test revenue each week since March 23. Weekly revenue losses will continue at this rate until patients begin visiting their physicians and hospitals again perform elective services. (Chart copyright: XIFIN, Inc.)
Many CLIA-certified community laboratories and hospital labs have the diagnostic instruments and experience to perform rapid molecular tests for COVID-19. But when contacted, they tell us that their suppliers do not ship them even minimal quantities of the COVID-19 kits, the reagents, and the consumables. Thus, they cannot meet the needs of their client physicians. Instead, they watch as these physicians refer COVID-19 tests to the nation’s largest labs. The supply shortage prevents these smaller labs from doing larger numbers of COVID-19 test for the patients in the communities they serve. It also prevents them from earning the revenues from COVID-19 testing that currently helps the nation’s “have” labs offset the decline in revenue from routine testing.
Congress, national healthcare policymakers, and state governors need to immediately address this situation. Each week that passes during the COVID-19 pandemic and the shelter-in-place directives drains another $800 million to $900 million in revenue from routine lab testing that previously flowed into the nation’s clinical laboratories.
‘Have-not’ Clinical Labs in Small Towns Will Quietly Shrink and Disappear
Without timely intervention and financial support, the nation’s network of ‘have not’ labs, which have so capably served towns away from big metropolitan centers and rural areas, will quietly begin shrinking. One at a time, labs in small towns will close or sell. Local lab facilities will be shuttered and specimens from small-town patients will be transported to big labs hundreds or thousands of miles away.
It is also true that the financial disaster besetting the nation’s clinical laboratory industry will have comparable dramatic consequences for the in vitro diagnostics (IVD) manufacturers that sell them automation, analyzers, reagents, and other supplies. Since early March, IVD manufacturers watched as the pandemic caused orders for new instruments to collapse. During these same weeks, their clinical lab customers ceased ordering routine test kits at pre-pandemic levels. Dark Daily will cover the challenges confronting the IVD and other diagnostics industries in future e-briefings.
Announcing Free COVID-19 STAT Intelligence Briefings for Clinical Labs
With the COVID-19 pandemic creating chaos in nearly every aspect of healthcare, business, and society, clinical labs and their suppliers need timely intelligence and analysis about the innovations and successes achieved by their peers. This week, Dark Daily and The Dark Report are launching COVID-19 STAT Intelligence Briefings (Copy and paste this URL into your browser: https://www.covid19briefings.com). This comprehensive service is free and will cover four basic areas of needs for clinical laboratories as they ramp up COVID-19 testing:
Daily and weekly COVID-19 testing dashboards to guide every lab’s short-term planning;
Proven steps for labs to introduce and validate COVID-19 tests (both rapid molecular tests and serology tests);
Getting paid for COVID-19 testing to ensure every lab’s financial stability and clinical quality; and
Legal and regulatory updates for labs doing COVID19 tests to ensure full compliance.
Also, to help clinical laboratory leaders deal with the coming wave of COVID-19 serology tests, we are producing a free webinar led by James O. Westgard, PhD, FACB, and Sten Westgard, Director of Client Services and Technology, of Westgard QC, Inc.
Each week that the SARS-CoV-2 pandemic continues, and strict shelter-in-place directives are in place, the clinical laboratory industry loses another almost $900 million in revenue from lower volumes of routine testing. No industry can survive when its incoming revenue collapses by 50% to 60% for sustained periods of time.
Will Congress Recognize the Need for a Financial Rescue of ‘Have-not’ Labs?
Thus, it is incumbent on Congress, elected officials, and healthcare policymakers to recognize the financial consequences of the pandemic to the nation’s clinical laboratories. That is particularly true of the ‘have-not’ clinical labs. They do not have the same access to decisionmakers in government as billion-dollar lab companies.
And yet, these labs located in small communities and rural areas often are the only local labs that can do STAT testing in a couple of hours, and where clinical pathologists are personally familiar with local physicians and patients.
These “have-not” labs are vital healthcare resources. They should receive the help they need to get through this unprecedented crisis that is the COVID-19 pandemic.
To offset the loss of revenue from the price cuts to Medicare Part B clinical laboratory tests, labs will need to aggressively—but wisely—slash costs to balance their budgets
Many experienced industry executives expect this to be the single most financially disruptive event to hit the clinical laboratory profession in more than 20 years. This will not only have a substantial negative financial impact on all labs—large and small—but two sectors of the clinical lab industry are considered to be so financially vulnerable they could cease to exist.
At Greatest Risk of Financial Failure are Community Laboratories
The first sector is comprised of smaller community lab companies that operate in towns and rural areas. These labs are at the greatest risk because they are the primary providers of lab testing services to the nursing homes and skilled nursing facilities in their neighborhoods. And because they have a high proportion of Medicare Part B revenue.
Thus, the expected Medicare price cuts to the high-volume automated lab tests—such as chemistry panels and CBCs (complete blood count) that are the bread-and-butter tests for these labs—will swiftly move them from minimal profit margins to substantial losses. Since these labs have a cost-per-test that is significantly higher than the nation’s largest public lab companies, they will be unable to financially survive the 2018 Medicare fee cuts.
The second sector at risk is comprised of rural hospitals and modest-sized community hospitals. What officials at CMS and their consulting companies overlooked when they created the PAMA (Protecting Access to Medicare Act) private payer market price reporting rule is that these hospitals provide lab testing services to nursing homes and office-based physicians in their service areas.
Because of the low volumes of testing in these hospital labs, they also have a larger average cost-per-test than the big public labs. Thus, the 2018 cuts to Medicare Part B lab test prices will erode or erase any extra margin from this testing that now accrues to these hospitals.
Rural and Small Community Hospitals Rely on Lab Outreach Revenue
The financial disruption these Medicare lab test price cuts will cause to rural and community hospitals is a real thing. These hospitals rely on outreach lab test revenues to subsidize many other clinical services within the hospital. One rural hospital CEO confirmed the importance of lab outreach revenue to her organization. Michelle McEwen, FACHE, CEO of Speare Memorial Hospital in Plymouth, N.H., spoke to The Dark Report in 2012 about the financial disruption that was happening when a major health insurer excluded her hospital’s laboratory from its network.
Speare Memorial is a 25-bed critical access hospital in the central part of the state between the lakes region and the White Mountain National Forest. McEwen was blunt in her assessment of the importance of clinical laboratory outreach revenues to her hospital. “The funds generated by performing these [outreach] lab tests are used to support the cost of providing laboratory services to all patients 24/7, including stat labs for emergency patients and inpatients,” McEwen explained. “These funds also help support other services in the hospital where losses are typically incurred, such as the emergency room and obstetric programs.” (See “Critical Access Hospitals Losing Lab Test Work,” The Dark Report, April 2, 2012.)
All Medical Laboratories Will Suffer Financial Pain from Medicare Price Cuts
But it is not just community lab companies and rural hospitals that are at risk of financial failure as the Medicare Part B cuts are implemented by CMS on Jan. 1, 2018. Any clinical laboratory serving Medicare patients will experience a meaningful drop in revenue. Many larger hospital and health system laboratories are recasting their financial projections for 2018 to identify how big a drop in revenue they will experience and what cost-cutting strategies will be needed to at least break even on their lab outreach business.
This explains why the first big trend of 2018 will be substantial revenue cuts from the Medicare program. It also explains why the second big trend of 2018 will be smart cost-cutting as labs attempt to balance their books and lower spending proportional to the reduced income they project.
Labs Have a Decade of Successful Cost-Cutting, More Cuts are Difficult
Aggressive cost-cutting, however, puts the nation’s medical laboratories at risk for a different reason. For the past decade, most well-run labs have already harvested the low-hanging fruit from obvious sources of cost reduction. They installed latest-generation automation. They re-engineered workflows using the techniques of Lean, Six Sigma, and process improvement.
During these same years, most medical laboratories also reduced technical staff and trimmed management ranks. That has created two new problems:
First, there are not enough managers in many labs to both handle the daily flow of work while also tackling specific projects to cut costs and boost productivity. Basically, these labs are already at their management limit, with no excess capacity for their lab managers to initiate and implement cost-cutting projects.
Second, technical staffs are already working at near peak capacity. Increased use of automation at these labs has reduced lab costs because labs were able to do the same volume of testing with fewer staff. However, the reduced staffs that oversee the lab automation are now working at their own peak capacity. Not only are they highly stressed from the daily routine, they also do not have spare time to devote to new projects designed to further cut costs.
Each Year Will Bring Additional Cuts to Medicare Part B Lab Prices
This is why all clinical laboratories in the United States will find it difficult to deal with the Medicare Part lab test fee cuts that will total $400 million during 2018. And what must be remembered is that, in 2019 and beyond, CMS officials will use the PAMA private payer market price reporting rule to make additional fee cuts. Over 10 years, CMS expects these cuts will reduce spending by $5.4 billion from the current spending level.
Taken collectively, all these factors indicate that many medical laboratories in the United States will not survive these Medicare fee cuts. The basic economics of operating a clinical laboratory say that less volume equals a higher average cost per test and higher volume equals a lower average cost per test.
Medical Labs with Highest Costs Most at Risk of Failure from Price Cuts
What this means in the marketplace is that labs with the highest average cost per test make the least profit margin on a fee-for-service payment. The opposite is true for labs with the lowest average cost per test. They will make a greater profit margin on that same fee-for-service payment.
Carry this fundamental economic principle of medical laboratory operations forward as Medicare Part B lab test fee cuts happen in 2018. Labs with the highest average cost per test will be first to go from a modest profit or break-even to a loss. As noted earlier, the clinical lab sectors that have the highest average cost per test are smaller community labs, along with rural and community hospitals. That is why they will be first to go out of business—whether by sale, bankruptcy, or by simply closing their doors.
Learning How to Cut Lab Costs While Protecting Quality
Every pathologist and lab administrator seeking the right strategies to further cut costs in their lab, while protecting quality and enhancing patient services, will want to consider sending a team from their laboratory to the 11th Annual Lab Quality Confab that takes place in New Orleans on October 24-25, 2018.
Anticipating the greater need for shrewd cost-cutting that also protects the quality of the lab’s testing services, this year’s Lab Quality Confab has lined up more than 51 speakers and 39 sessions. Of particular interest are these extended workshops that come with certifications:
Lab Quality Confab is recognized for its use of lab case studies—taught by the nation’s early adopter lab organizations. Certification classes are available to gain proficiency in the use of Lean methods and Six Sigma tools, such as:
Developing single-piece and small batch workflow to cut TAT and lift productivity.
Given the strong interest in smart ways to cut costs, boost productivity, and balance revenue-versus-cost, registrations for this year’s Lab Quality Confab is running at a record pace. The full agenda can be viewed at this link (or copy this URL and paste into your browser: http://www.labqualityconfab.com/agenda).
Of special interest to lab leaders preparing to stay ahead of the financial impact of the Medicare Part B fee cuts, Lab Quality Confab offers deep discounts for four or more attendees from the same lab organization. This allows your lab’s most effective cost-cutters to see, hear, and learn together, so that when they return they can get a flying start helping you align your lab’s costs to the expected declines in revenue that will happen on Jan. 1, 2018.
As of January 1, CMS has begun accepting private payer market price data from certain medical laboratories required to report this information
Only 12 months remain before clinical laboratories in the United States face the ticking financial time bomb set to explode on January 1, 2018. That time bomb is the cuts to Medicare Part B clinical laboratory test fees that the federal Centers for Medicare and Medicaid Services (CMS) will implement on that date.
The Dark Report, Dark Daily’s sister publication, predicts that the Protecting Access to Medicare Act of 2014 (PAMA) private payer market price reporting final rule—if implemented by CMS as currently written—has the potential to be the single most financially disruptive event to hit the clinical laboratory industry during the past 25 years. At greatest risk are the nation’s smaller community laboratories and rural hospitals that rely on revenue from Medicare Part B lab testing to remain financially viable. (more…)