Only about a third of the hospitals surveyed are in full compliance with giving public access to prices, the watchdog group contends, but the AHA disputes its methodology
It’s been almost four years since the Centers for Medicare and Medicaid Services (CMS) enacted its Hospital Price Transparency rule which requires hospitals—including their medical laboratories—to make their prices available and easily accessible to the public. But according to a 2024 report from PatientRightsAdvocate.org (PRA), just 34.5% of reviewed hospitals are fully compliant with the transparency rule. That’s a slight decrease from the 36% compliance rate the PRA listed in its 2023 report, the watchdog group stated in a blog post.
Released on Feb. 29, this was the group’s sixth semi-annual hospital price transparency report since the CMS rule took effect in 2021.
The rule “requires hospitals to post all prices online, easily accessible and searchable, in the form of (i) a single machine-readable standard charges file for all items, services, and drugs by all payers and all plans, the de-identified minimum and maximum negotiated rates, and all discounted cash prices, as well as (ii) prices for the 300 most common shoppable services either as a consumer-friendly standard charges display listing actual prices or, alternatively, as a price estimator tool,” the report states.
The required viewable prices are to be for, among others, medical imaging, clinical laboratory testing, and outpatient procedures such as a colonoscopies, etc.
“With full transparency, consumers can benefit from competition to make informed decisions, protect from overcharges, billing errors, and fraud, and lower their costs,” the report states. “Employer and union plans can use pricing and claims data to improve their plan designs and direct members to lower cost, high-quality facilities. However, continued noncompliance impedes this ability.”
At any time, the US Department of Justice (DOJ) could decide to file charges against a hospital or a clinical laboratory for not posting their prices on their websites in compliance with the federal rule. Such an action by DOJ officials would be to specifically put the entire industry on notice that there will be consequences for non-compliance.
The PRA’s report provides hospitals and clinical laboratories with a reminder that consumer watchdogs are also monitoring compliance.
“Our comprehensive study of 2,000 hospitals indicates nearly two-thirds (65.5%) of hospitals reviewed continue failing to fully comply with the rule, yet the Centers for Medicare and Medicaid Services (CMS) has only fined fourteen hospitals for noncompliance out of the thousands found to not be meeting all of the rule’s requirements. When hospitals don’t post their prices, they can charge whatever they want,” wrote PRA Founder and Chairman Cynthia Fisher (above) in a letter to President Biden. Hospital medical laboratories are also required to post their prices for tests. (Photo copyright: PatientRightsAdvocate.org.)
To compile their report, PRA analysts examined the websites of 2,000 US hospitals between September 3, 2023, and January 13, 2023, and found that 1,311, or 65.5%, were not in full compliance, mostly due to “missing or significantly incomplete pricing data,” the report states.
More than 6,000 licensed hospitals operate in the US, the report notes. The group said it focused on hospitals owned by the largest US health systems.
Among the notable findings:
The 2023 report found that 98% of Kaiser Permanente’s 42 hospitals were in full compliance with the rule, but in the 2024 study, none were compliant because the hospitals began posting multiple files instead of a single file.
In total, 103 hospitals rated as noncompliant in the previous report were found to be compliant in the new analysis. Conversely, 135 hospitals previously rated as compliant were listed as noncompliant in the 2024 report.
The report lauded three hospitals for posting “exemplary files” that were “easily accessible, downloadable, machine-readable, and including all negotiated rates by payer and plan.” Those were Cape Cod Hospital in Hyannis, Mass.; Christus Santa Rosa Medical Center in San Antonio; and UW Health University Hospital in Madison, Wis.
In its discussion of the findings, PRA called on CMS to step up enforcement of the pricing transparency rule. The group also wants the government to close what it describes as the “estimator tool loophole,” which allows hospitals to list non-binding price estimates and price ranges instead of concrete prices.
“Price estimator tools do not achieve the goals of price transparency policy and fundamentally undermine the intent of the regulations,” the PRA’s report contends.
In response to the 2023 PRA report, AHA Group Vice President for Public Policy Molly Smith issued the following statement, “Once again, Patient Rights Advocate has put out a report that blatantly misconstrues, ignores, and mischaracterizes hospitals’ compliance with federal price transparency regulations. The AHA has repeatedly debunked point-by-point Patient Rights Advocate’s intentionally misleading ‘reports’ on price transparency.”
Citing CMS data, Smith said that as of 2022, 70% of US hospitals had complied with two key federal rules:
One requiring hospitals to post machine-readable files with pricing information.
The other mandating a list of prices for at least 300 “shoppable” services.
More than 80% of hospitals had complied with at least one of the rules, she contended in an AHA press release.
Speaking to the New Orleans Times-Picayune, PRA Founder and Chairman Cynthia Fisher said her group performs a more in-depth study of pricing data compared with CMS.
“They did not do a comprehensive review,” she told the publication. “We do a deep dive for full compliance.”
The PRA study came on the heels of a January report from Turquoise Health that offered a rosier assessment of hospital compliance, albeit with different criteria. According to the Turquoise report, as of Dec. 15, 2023:
90.7% of 6,357 US hospitals had posted machine-readable files,
83.1% posted information about negotiated rates, and
77.3% posted cash rates.
The Turquoise Health end-to-end price transparency platform uses a 5-point system to rate the quality of hospitals’ machine-readable files and said that more than 50% scored five stars. Clinical laboratory managers and pathologists may find it timely to review their lab organization’s compliance with this federal price transparency rule.
This may be a new ‘sign of the times’ as hospitals, clinical laboratories, and other healthcare providers working with AI find they also need to hire their own prompt engineers
AI “prompting,” according to Florida State University, “refers to the process of interacting with an AI system by providing specific instructions or queries to achieve a desired outcome.”
According to workable.com, prompt engineers specialize “in developing, refining, and optimizing AI-generated text prompts to ensure they are accurate, engaging, and relevant for various applications. They also collaborate with different teams to improve the prompt generation process and overall AI system performance.”
Healthcare institutions are getting more serious about using AI to improve daily workflows and clinical care, including in the clinical laboratory and pathology departments. But adopting the new technology can be disruptive. To ensure the implementation goes smoothly, hospitals are now seeking prompt engineers to guide the organization’s strategy for using AI.
When Boston Children’s Hospital leaders set out to find such a person, they looked for an individual who had “a clinical background [and] who knows how to use these tools. Someone who had experience coding for large language models and natural language processing, but who could also understand clinical language,” according to MedPage Today.
“We got many, many applications, some really impressive people, but we were looking for a specific set of skills and background,” John Brownstein, PhD, Chief Innovation Officer at Boston Children’s Hospital and Professor of Biomedical Informatics at Harvard Medical School, told MedPage Today.
“It was not easy to find [someone]—a bit of a unicorn-type candidate,” noted Brownstein, who is also a medical contributor to ABC News.
After a four-month search, the hospital hired Dinesh Rai, MD, emergency room physician and AI engineer, for the position. According to Brownstein, Rai had “actually practiced medicine, lived in a clinical environment,” and had “successfully launched many [AI] applications on top of large language models,” MedPage Today reported.
“Some of the nuances I bring to the table in terms of being a physician and having worked clinically and understanding really deeply the clinical workflows and how we can implement the [AI] technology—where its limits are, where it can excel, and the quickest way to get things [done],” Dinesh Rai, MD (above), told MedPage Today. “I’m happy to be able to help with all of that.” Hospital clinical laboratory and pathology managers may soon by engaging with prompt engineers to ensure the smooth use of AI in their departments. (Photo copyright: LinkedIn.)
Prompt Engineers are like F1 Drivers
“It’s kind of like driving a car, where basically anyone can drive an automatic car, and anyone can go onto ChatGPT, write some text, and get a pretty solid response,” said Rai, describing the act of AI prompting to MedPage today.
Then, there are “people who know how to drive manual, and there are people who will know different prompting techniques, like chain-of-thought or zero-shot prompting,” he added. “Then you have those F1 drivers who are very intimate with the mechanics of their car, and how to use it most optimally.”
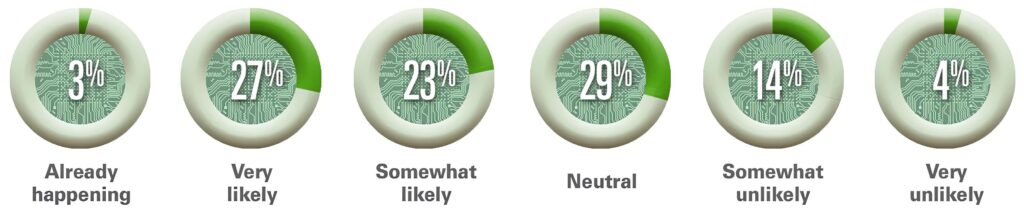
The American Hospital Association (AHA) believes that AI “holds great promise in helping healthcare providers gain insights and improve health outcomes.” In an article titled, “How AI Is Improving Diagnostics, Decision-Making and Care,” the AHA noted that, “Although many questions remain regarding its safety, regulation, and impact, the use of AI in clinical care is no longer in its infancy and is expected to experience exponential growth in the coming years.
“AI is improving data processing, identifying patterns, and generating insights that otherwise might elude discovery from a physician’s manual effort. The next five years will be critical for hospitals and health systems to build the infrastructure needed to support AI technology, according to the recently released Futurescan 2023,” the AHA wrote.
The graphic above is taken from the American Hospital Association’s article about Futurescan’s 2023 survey results on AI in healthcare. “Healthcare executives from across the nation were asked how likely it is that by 2028 a federal regulatory body will determine that Al for clinical care delivery augmentation (e.g., assisted diagnosis and prescription, personalized medication and care) is safe for use by our hospital or health systems,” AHA stated. This would include the use of AI in clinical laboratories and pathology group practices. (Graphic copyright: American Hospital Association.)
The AHA listed the top three opportunities for AI in clinical care as:
Clinical Decision Tools: “AI algorithms analyze a vast amount of patient data to assist medical professionals in making more informed decisions about care.”
Diagnostic and Imaging: The use of AI “allows healthcare professionals to structure, index, and leverage diagnostic and imaging data for more accurate diagnoses.”
Patient Safety: The use of AI improves decision making and optimizes health outcomes by evaluating patient data. “Systems that incorporate AI can improve error detection, stratify patients, and manage drug delivery.”
The hiring of a prompt engineer by Boston Children’s Hospital is another example of how AI is gaining traction in clinical healthcare. According to the Futurescan 2023 survey, nearly half of hospital CEOs and strategy leaders believe that health systems will have the infrastructure in place by 2028 to successfully utilize AI in clinical decision making.
“I’m lucky to [be] in an organization that has recognized the importance of AI as part of the future practice of medicine,” Rai told MedPage Today.
Pathologists and managers of clinical laboratories and genetic testing companies will want to track further advancements in artificial intelligence. At some point, the capabilities of future generations of AI solutions may encourage labs to hire their own prompt engineers.
Initially thought to be an attack by a nation-state, actual culprit turned out to be a known ransomware group and each day brings new revelations about the cyberattack
Fallout continues from cyberattack on Change Healthcare, the revenue cycle management (RCM) company that is a business unit of Optum, itself a division of UnitedHealth Group. Recent news accounts say providers are losing an estimated $100 million per day because they cannot submit claims to Change Healthcare nor receive reimbursement for these claims.
The cyberattack took place on February 21. The following day, UnitedHealth Group filed a Material Cybersecurity Incidents report (form 8-K) with the US Securities and Exchange Commission (SEC) in which it stated it had “identified a suspected nation-state associated cybersecurity threat actor [that] had gained access to some of the Change Healthcare information technology systems.”
A few days later the real identity of the threat actor was revealed to be a ransomware group known as “BlackCat” or “ALPHV,” according to Reuters.
Change Healthcare of Nashville, Tenn., is “one of the largest commercial prescription processors in the US,” Healthcare Dive reported, adding that hospitals, pharmacies, and military facilities had difficulty transmitting prescriptions “as a result of the outage.”
Change Healthcare handles about 15 billion payments each year.
According to a Change Healthcare statement, the company “became aware of the outside threat” and “took immediate action to disconnect Change Healthcare’s systems to prevent further impact.”
Change Healthcare has provided a website where parties that have been affected by the cyberattack can find assistance and updated information on Change’s response to the intrusion and theft of its data.
“The fallout is only starting to happen now. It will get worse for consumers,” Andrew Newman (above), founder and Chief Technology Officer, ReasonLabs, told FOX Business, adding, “We know that the likely destination for [the Change Healthcare] data is the Dark Web, where BlackCat will auction it all off to the highest bidder. From there, consumers could expect to suffer from things like identity theft, credit score downgrades, and more.” Clinical laboratories are also targets of cyberattacks due to the large amount of private patient data stored on their laboratory information systems. (Photo copyright: ReasonLabs.)
Millions of Records May be in Wrong Hands
Reuters reported that ALPHV/BlackCat admitted it “stole millions of sensitive records, including medical insurance and health data from the company.”
The ransomware group has been focusing its attacks on healthcare with 70 incidents since December, according to federal agencies.
In a letter to HHS, AHA warned, “Change Healthcare’s downed systems will have an immediate adverse impact on hospital finances. … Their interrupted technology controls providers’ ability to process claims for payment, patient billing, and patient cost estimation services.”
“My understanding is Change/Optum touches almost every hospital in the US in one way or another,” John Riggi, AHA’s National Advisor for Cybersecurity and Risk, told Chief Healthcare Executive. “It has sector wide impact in potential risk. So, really, this is an attack on the entire sector.” Riggi spent nearly 30 years with the FBI.
Some physician practices may also have been impacted by the Change Healthcare cyberattack, according to the Medical Group Management Association (MGMA). In a letter to HHS, MGMA described negative changes in processes at doctors’ offices. They include delays in paper and electronic statements “for the duration of the outage.”
In addition, “prescriptions are being called into pharmacies instead of being electronically sent, so patients’ insurance information cannot be verified by pharmacies, and [the patients] are forced to self-pay or go without necessary medication.”
Here are “just a few of the consequences medical groups have felt” since the Change Healthcare cyberattack, according to the MGMA:
Substantial billing and cash flow disruptions, such as a lack of electronic claims processing. Both paper and electronic statements have been delayed. Some groups have been without any outgoing charges or incoming payments for the duration of the outage.
Limited or no electronic remittance advice from health plans. Groups are having to manually pull and post from payer portals.
Prior authorization submissions have been rejected or have not been transmittable at all. This further exacerbates what is routinely ranked the number one regulatory burden by medical groups and jeopardizes patient care.
Groups have been unable to perform eligibility checks for patients.
Many electronic prescriptions have not been transmitted, resulting in call-in prescriptions to pharmacies or paper prescriptions for patients. Subsequently, patients’ insurance information cannot be verified by pharmacies, and they are forced to self-pay or go without necessary medication.
Lack of connectivity to important data infrastructure needed for success in value-based care arrangements, and other health information technology disruptions.
Medical laboratory leaders and pathologists are advised to consult with their colleagues in IT and cybersecurity on how to best prevent ransomware attacks. Labs hold vast amount of private patient information. Recent incidents suggest more steps and strategies may be needed to protect laboratory information systems and patient data.
Some hospital organizations are pushing back, stating that the new regulations are ‘too rigid’ and interfere with doctors’ treatment of patients
In August, the Biden administration finalized provisions for hospitals to meet specific treatment metrics for all patients with suspected sepsis. Hospitals that fail to meet these requirements risk the potential loss of millions of dollars in Medicare reimbursements annually. This new federal rule did not go over well with some in the hospital industry.
Sepsis kills about 350,000 people every year. One in three people who contract the deadly blood infection in hospitals die, according to the Centers for Disease Control and Prevention (CDC). Thus, the federal government has once again implemented a final rule that requires hospitals, clinical laboratories, and medical providers to take immediate actions to diagnose and treat sepsis patients.
The effort has elicited pushback from several healthcare organizations that say the measure is “too rigid” and “does not allow clinicians flexibility to determine how recommendations should apply to their specific patients,” according to Becker’s Hospital Review.
Perform blood tests within a specific period of time to look for biomarkers in patients that may indicate sepsis, and to
Administer antibiotics within three hours after a possible case is identified.
It also mandates that certain other tests are performed, and intravenous fluids administered, to prevent blood pressure from dipping to dangerously low levels.
“These are core things that everyone should do every time they see a septic patient,” said Steven Simpson, MD, Professor of medicine at the University of Kansas told Fierce Healthcare. Simpson is also the chairman of the Sepsis Alliance, an advocacy group that works to battle sepsis.
Simpson believes there is enough evidence to prove that the SEP-1 guidelines result in improved patient care and outcomes and should be enforced.
“It is quite clear that this works better than what was present before, which was nothing,” he said. “If the current sepsis mortality rate could be cut by even 5%, we could save a lot of lives. Before, even if you were reporting 0% compliance, you didn’t lose your money. Now you actually have to do it,” Simpson noted.
“We are encouraged by the increased attention to sepsis and support CMS’ creation of a sepsis mortality measure that will encourage hospitals to pay more attention to the full breadth of sepsis care,” Chanu Rhee, MD (above), Infectious Disease/Critical Care Physician and Associate Hospital Epidemiologist at Brigham and Women’s Hospital told Healthcare Finance. The new rule, however, requires doctors and medical laboratories to conduct tests and administer antibiotic treatment sooner than many healthcare providers deem wise. (Photo copyright: Brigham and Women’s Hospital.)
Healthcare Organizations Pushback against Final Rule
“By encouraging the use of broad spectrum antibiotics when more targeted ones will suffice, this measure promotes the overuse of the antibiotics that are our last line of defense against drug-resistant bacteria,” the AHA’s letter states.
In its recent coverage of the healthcare organizations’ pushback to CMS’ final rule, Healthcare Finance News explained, “The SEP-1 measure requires clinicians to provide a bundle of care to all patients with possible sepsis within three hours of recognition. … But the SEP-1 measure doesn’t take into account that many serious conditions present in a similar fashion to sepsis … Pushing clinicians to treat all these patients as if they have sepsis … leads to overuse of broad-spectrum antibiotics, which can be harmful to patients who are not infected, those who are infected with viruses rather than bacteria, and those who could safely be treated with narrower-spectrum antibiotics.”
CMS’ latest rule follows the same evolutionary path as previous federal guidelines. In August 2007, CMS announced that Medicare would no longer pay for additional costs associated with preventable errors, including situations known as Never Events. These are “adverse events that are serious, largely preventable, and of concern to both the public and healthcare providers for the purpose of public accountability,” according to the Leapfrog Group.
In 2014, the CDC suggested that all US hospitals have an antibiotic stewardship program (ASP) to measure and improve how antibiotics are prescribed by clinicians and utilized by patients.
Research Does Not Show Federal Sepsis Programs Work
He points to analysis which showed that though use of broad-spectrum antibiotics increased after the original 2015 SEP-1 regulations were introduced, there has been little change to patient outcomes.
“Unfortunately, we do not have good evidence that implementation of the sepsis policy has led to an improvement in sepsis mortality rates,” Rhee told Fierce Healthcare.
Rhee believes that the latest regulations are a step in the right direction, but that more needs to be done for sepsis care. “Retiring past measures and refining future ones will help stimulate new innovations in diagnosis and treatment and ultimately improve outcomes for the many patients affected by sepsis,” he told Healthcare Finance.
Sepsis is very difficult to diagnose quickly and accurately. Delaying treatment could result in serious consequences. But clinical laboratory blood tests for blood infections can take up to three days to produce a result. During that time, a patient could be receiving the wrong antibiotic for the infection, which could lead to worse problems.
The new federal regulation is designed to ensure that patients receive the best care possible when dealing with sepsis and to lower mortality rates in those patients. It remains to be seen if it will have the desired effect.
Newly-defined Cardiovascular-Kidney-Metabolic Syndrome (CKM) means physicians will be in close collaboration with clinical laboratories to make accurate diagnoses
In a presidential advisory, the AHA defines a newly described systemic health disorder called Cardiovascular-Kidney-Metabolic Syndrome (CKM). The syndrome “is a systemic disorder characterized by pathophysiological interactions among metabolic risk factors, CKD (chronic kidney disease), and the cardiovascular system leading to multi-organ failure and a high rate of adverse cardiovascular outcomes.”
A CKM diagnosis, which is meant to identify patients who are at high risk of dying from heart disease, is based on a combination of risk factors, including:
weight problems,
issues with blood pressure, cholesterol, and/or blood sugar,
reduced kidney function.
CKM is a new term and doctors will be ordering medical laboratory tests associated with diagnosing patients with multiple symptoms to see if they match this diagnosis. Thus, clinical laboratory managers and pathologists will want to follow the adoption/implementation of this new recommendation.
“The advisory addresses the connections among these conditions with a particular focus on identifying people at early stages of CKM syndrome,” said Chiadi Ndumele, MD, PhD (above), Associate Professor of Medicine at Johns Hopkins University and one of the authors of the AHA paper, in a news release. “Screening for kidney and metabolic disease will help us start protective therapies earlier to most effectively prevent heart disease and best manage existing heart disease.” Clinical laboratories will play a key role in those screenings and in diagnosis of the new syndrome. (Photo copyright: Johns Hopkins University.)
Stages of CKM Syndrome
In its presidential advisory, the AHA wrote, “Cardiovascular-Kidney-Metabolic (CKM) syndrome is defined as a health disorder attributable to connections among obesity, diabetes, chronic kidney disease (CKD), and cardiovascular disease (CVD), including heart failure, atrial fibrillation, coronary heart disease, stroke, and peripheral artery disease. CKM syndrome includes those at risk for CVD and those with existing CVD.”
The five stages of CKM syndrome, which the AHA provided to give a framework for patients to work towards regression of the syndrome, are:
Stage 0: No CKM risk factors. Individuals should be screened every three to five years for blood pressure, cholesterol, and blood sugar levels, and for maintaining a healthy body weight.
Stage 1: Excess body fat and/or an unhealthy distribution of body fat, such as abdominal obesity, and/or impaired glucose tolerance or prediabetes. Patients have risk factors such as weight problems or prediabetes and are encouraged to make healthy lifestyle changes and try to lose at least 5% of their body weight.
Stage 2: Metabolic risk factors and kidney disease. Includes people who already have Type 2 diabetes, high blood pressure, high triglyceride levels, and/or kidney disease. Medications that target kidney function, lower blood sugar, and which help with weight loss should be considered at this stage to prevent diseases of the heart and blood vessels or kidney failure.
Stage 3: Early cardiovascular disease without symptoms in people with metabolic risk factors or kidney disease or those at high predicted risk for cardiovascular disease. People show signs of disease in their arteries, or have heart function issues, or may have already had a stroke or heart attack or have kidney or heart failure. Medication may also be needed at this stage.
Stage 4: Symptomatic cardiovascular disease in people with excess body fat, metabolic risk factors or kidney disease. In this stage, people are categorized as with or without having kidney failure. May also have already had a heart attack, stroke or heart failure, or cardiovascular conditions such as peripheral artery disease or atrial fibrillation.
“We now have several therapies that prevent both worsening kidney disease and heart disease,” said Chiadi Ndumele, MD, PhD, Associate Professor of Medicine at Johns Hopkins University and one of the authors of the Circulation paper, in a news release. “The advisory provides guidance for healthcare professionals about how and when to use those therapies, and for the medical community and general public about the best ways to prevent and manage CKM syndrome.”
According to an AHA 2023 Statistical Update, one in three adults in the US have three or more risk factors that contribute to cardiovascular disease, metabolic disorders, or kidney disease. While CKM affects nearly every major organ in the body, it has the biggest impact on the cardiovascular system where it can affect the blood vessels, heart muscle function, the rate of fatty buildup in the arteries, electrical impulses in the heart and more.
“There is a need for fundamental changes in how we educate healthcare professionals and the public, how we organize care and how we reimburse care related to CKM syndrome,” Ndumele noted. “Key partnerships among stakeholders are needed to improve access to therapies, to support new care models, and to make it easier for people from diverse communities and circumstances to live healthier lifestyles and to achieve ideal cardiovascular health.”
New AHA Risk Calculator
In November, the AHA announced PREVENT (Predicting risk of cardiovascular disease EVENTs), a tool that doctors can use to assess a person’s risk for heart attack, stroke, and heart failure. The new risk calculator, which incorporates CKM, allows physicians to evaluate younger people as well, and examine their long-term risks for cardiovascular issues.
Doctors can use PREVENT to assess people ages 30 to 79 and predict risk for heart attack, stroke, or heart failure over 10 to 30 years.
“Longer-term estimates are important because short-term or 10-year risk in most young adults is still going to be low. We wanted to think more broadly and apply a life-course perspective,” Khan said. “Providing information on 30-year risk may reveal earlier opportunities for intervention and prevention efforts in younger people.”
According to CDC data, about 695,000 people died of heart disease in the US in 2021. That equates to one in every five deaths. Clinical pathologists will need to understand the AHA recommendations and how doctors will be ordering clinical laboratory tests to determine if a patient has CKM. Then, labs will play a role in helping doctors monitor patients to optimize health and prevent acute episodes that put patients in the hospital.