Best of all, the researchers say the test could provide an inexpensive means of early diagnosis. This assay could also be used to monitor how well patients respond to cancer therapy, according to a news release.
The protein had previously been identified as a promising biomarker and is readily detectable in tumor tissue, they wrote. However, it is found in extremely low concentrations in blood plasma and is “well below detection limits of conventional clinical laboratory methods,” they noted.
To overcome that obstacle, they employed an ultra-sensitive immunoassay known as a Simoa (Single-Molecule Array), an immunoassay platform for measuring fluid biomarkers.
“We were shocked by how well this test worked in detecting the biomarker’s expression across cancer types,” said lead study author gastroenterologist Martin Taylor, MD, PhD, Instructor in Pathology, Massachusetts General Hospital and Harvard Medical School, in the press release. “It’s created more questions for us to explore and sparked interest among collaborators across many institutions.”
“We’ve known since the 1980s that transposable elements were active in some cancers, and nearly 10 years ago we reported that ORF1p was a pervasive cancer biomarker, but, until now, we haven’t had the ability to detect it in blood tests,” said pathologist and study co-author Kathleen Burns, MD, PhD (above), Chair of the Department of Pathology at Dana-Farber Cancer Institute and a Professor of Pathology at Harvard Medical School, in a press release. “Having a technology capable of detecting ORF1p in blood opens so many possibilities for clinical applications.” Clinical laboratories may soon have a new blood test to detect multiple types of cancer. (Photo copyright: Dana-Farber Cancer Institute.)
Simoa’s Advantages
In their press release, the researchers described ORF1p as “a hallmark of many cancers, particularly p53-deficient epithelial cancers,” a category that includes lung, breast, prostate, uterine, pancreatic, and head and neck cancers in addition to the cancers noted above.
“Pervasive expression of ORF1p in carcinomas, and the lack of expression in normal tissues, makes ORF1p unlike other protein biomarkers which have normal expression levels,” Taylor said in the press release. “This unique biology makes it highly specific.”
Simoa was developed at the laboratory of study co-author David R. Walt, PhD, the Hansjörg Wyss Professor of Bioinspired Engineering at Harvard Medical School, and Professor of Pathology at Harvard Medical School and Brigham and Women’s Hospital.
The Simoa technology “enables 100- to 1,000-fold improvements in sensitivity over conventional enzyme-linked immunosorbent assay (ELISA) techniques, thus opening the window to measuring proteins at concentrations that have never been detected before in various biological fluids such as plasma or saliva,” according to the Walt Lab website.
Simoa assays take less than two hours to run and require less than $3 in consumables. They are “simple to perform, scalable, and have clinical-grade coefficients of variation,” the researchers wrote.
Study Results
Using the first generation of the ORF1p Simoa assay, the researchers tested blood samples of patients with a variety of cancers along with 406 individuals, regarded as healthy, who served as controls. The test proved to be most effective among patients with colorectal and ovarian cancer, finding detectable levels of ORF1p in 58% of former and 71% of the latter. Detectable levels were found in patients with advanced-stage as well as early-stage disease, the researchers wrote in Cancer Discovery.
Among the 406 healthy controls, the test found detectable levels of ORF1p in only five. However, the control with the highest detectable levels, regarded as healthy when donating blood, “was six months later found to have prostate cancer and 19 months later found to have lymphoma,” the researchers wrote.
They later reengineered the Simoa assay to increase its sensitivity, resulting in improved detection of the protein in blood samples from patients with colorectal, gastroesophageal, ovarian, uterine, and breast cancers.
The researchers also employed the test on samples from 19 patients with gastroesophageal cancer to gauge its utility for monitoring therapeutic response. Although this was a small sample, they found that among 13 patients who had responded to therapy, “circulating ORF1p dropped to undetectable levels at follow-up sampling.”
“More Work to Be Done”
The Simoa assay has limitations, the researchers acknowledged. It doesn’t identify the location of cancers, and it “isn’t successful in identifying all cancers and their subtypes,” the press release stated, adding that the test will likely be used in conjunction with other early-detection approaches. The researchers also said they want to gauge the test’s accuracy in larger cohorts.
“The test is very specific, but it doesn’t tell us enough information to be used in a vacuum,” Walt said in the news release. “It’s exciting to see the early success of this ultrasensitive assessment tool, but there is more work to be done.”
More studies will be needed to valid these findings. That this promising new multi-cancer immunoassay is based on a clinical laboratory blood sample means its less invasive and less painful for patients. It’s a good example of an assay that takes a proteomic approach looking for protein cancer biomarkers rather than the genetic approach looking for molecular DNA/RNA biomarkers of cancer.
Theranos founder and former CEO continues down the path she began by defrauding her investors and lying to clinical laboratory leaders about her technology’s capabilities
As a result of the ban, Holmes is “barred from receiving payments from federal health programs for services or products, which significantly restricts her ability to work in the healthcare sector,” ARS Technica reported.
So, Holmes, who is 39-years old, is basically banned for life. This is in addition to her 11-year prison sentence which was paired with $452,047,200 in restitution.
“The exclusion was announced by Inspector General Christi Grimm of the Department of Health and Human Services’ Office of Inspector General,” ARS Technica noted, adding that HHS-OIG also “excluded former Theranos President Ramesh “Sunny” Balwani from federal health programs for 90 years.” This is on top of the almost 13-year-long prison sentence he is serving for fraud.
“The Health and Human Services Department can exclude anyone convicted of certain felonies from Medicare, Medicaid, and Pentagon health programs,” STAT reported.
“Accurate and dependable diagnostic testing technology is imperative to our public health infrastructure,” said Inspector General Christi Grimm (above) in an HHS-OIG statement. “As technology evolves, so do our efforts to safeguard the health and safety of patients, and HHS-OIG will continue to use its exclusion authority to protect the public from bad actors.” Observant clinical laboratory leaders will recognize this as yet another episode in the Elizabeth Holmes/Theranos fraud saga they’ve been following for years. (Photo copyright: HHS-OIG.)
Why the Ban?
“The Office of Inspector General (OIG) for the Department of Health and Human Services (HHS) cited Holmes’ 2022 conviction for fraud and conspiracy to commit wire fraud as the reason for her ban,” The Hill reported.
“False statements related to the reliability of these medical products can endanger the health of patients and sow distrust in our healthcare system,” Grimm stated in the HHS-OIG statement, which noted, “The statutory minimum for an exclusion based on convictions like Holmes’ is five years.
“When certain aggravating factors are present, a longer period of exclusion is justified,” the statement continued. “The length of Holmes’ exclusion is based on the application of several aggravating factors, including the length of time the acts were committed, incarceration, and the amount of restitution ordered to be paid.”
Rise and Fall of Elizabeth Holmes
Readers of Dark Daily’s e-briefs covering the Holmes/Theranos fraud saga will recall details on Holmes’ journey from mega success to her current state of incarceration for defrauding her investors.
In November 2022, she was handed an 11-year prison sentence for not disclosing that Theranos’ innovative blood testing technology, Edison, was producing flawed and false results. Theranos had “raised hundreds of millions of dollars, named prominent former US officials to its board, and explored a partnership with the US military to use its tests on the battlefield,” STAT reported.
To get Holmes physically into prison was a journey unto itself. At one point, evidence showed her as a potential flight risk. “In the same court filings, prosecutors said Holmes and her partner, William Evans, bought one-way tickets to Mexico in December 2021, a fact confirmed by her lawyers,” Dark Daily’s sister publication The Dark Report revealed in “Elizabeth Holmes’ Appeal Questions Competence of CLIA Lab Director.”
Drama around her move into prison continued. “The former CEO’s attorneys are making last-minute legal moves to delay her prison sentence while she appeals her guilty verdict,” Dark Daily reported.
At the same time, Holmes appeared to be on a mission to revamp her public image.
In the Times piece, Holmes talked about her plans to continue to pursue a life in healthcare. “In the story, Holmes contended that she still thinks about contributing to the clinical laboratory field. Holmes told The Times that she still works on healthcare-related inventions and will continue to do so if she reports to prison,” The Dark Report covered in “Elizabeth Holmes Still Wants ‘To Contribute’ in Healthcare.”
In the meantime, her legal fees continued to mount beyond her ability to pay. “Holmes’ prior cadre of lawyers quit after she could not compensate them, The Times reported,” The Dark Report noted. “One pre-sentencing report by the government put her legal fees at more than $30 million,” according to The New York Times.
Apparently, this closes the latest chapter in the never-ending saga of Elizabeth Holmes’ fall from grace and ultimate conviction for defrauding her investors and lying to healthcare executives, pathologists, and clinical laboratory leaders.
According to an EADV press release, the AI software demonstrated a “100% (59/59 cases identified) sensitivity for detecting melanoma—the most serious form of skin cancer.” The AI software also “correctly detected 99.5% (189/190) of all skin cancers and 92.5% (541/585) of pre-cancerous lesions.”
“Of the basal cell carcinoma cases, a single case was missed out of 190, which was later identified at a second read by a dermatologist ‘safety net.’ This further demonstrates the need to have appropriate clinical oversight of the AI,” the press release noted.
AI is being utilized more frequently within the healthcare industry to diagnose and treat a plethora of illnesses. This recent study performed by scientists in the United Kingdom demonstrates that new AI models can be used to accurately diagnose some skin cancers, but that “AI should not be used as a standalone detection tool without the support of a consultant dermatologist,” the press release noted.
“The role of AI in dermatology and the most appropriate pathway are debated,” said Kashini Andrew, MBBS, MSc (above), Specialist Registrar at University Hospitals Birmingham NHS Foundation Trust. “Further research with appropriate clinical oversight may allow the deployment of AI as a triage tool. However, any pathway must demonstrate cost-effectiveness, and AI is currently not a stand-alone tool in dermatology. Our data shows the great promise of AI in future provision of healthcare.” Clinical laboratories and dermatopathologists in the United States will want to watch the further development of this AI application. (Photo copyright: LinkedIn.)
How the NHS Scientists Conducted Their Study
Researchers tested their algorithm for almost three years to determine its ability to detect cancerous and pre-cancerous growths. A group of dermatologists and medical photographers entered patient information into their algorithm and trained it how to detect abnormalities. The collected data came from 22,356 patients with suspected skin cancers and included photos of known cancers.
The scientists then repeatedly recalibrated the software to ensure it could distinguish between non-cancerous lesions and potential cancers or malignancies. Dermatologists then reviewed the final data from the algorithm and compared it to diagnoses from health professionals.
“This study has demonstrated how AI is rapidly improving and learning, with the high accuracy directly attributable to improvements in AI training techniques and the quality of data used to train the AI,” said Kashini Andrew, MBBS, MSc, Specialist Registrar at University Hospitals Birmingham NHS Foundation Trust, and co-author of the study, in EADV press release.
Freeing Up Physician Time
The EADV Congress where the NHS researchers presented their findings took place in October in Berlin. The first model of their AI software was tested in 2021 and that version was able to detect:
85.9% (195 out of 227) of melanoma cases,
83.8% (903 out of 1078) of all skin cancers, and
54.1% (496 out of 917) of pre-cancerous lesions.
After fine-tuning, the latest version of the algorithm was even more promising, with results that included the detection of:
100% (59 out of 59) cases of melanoma,
99.5% (189 out of 190) of all skin cancers, and
92.5% (541 out of 585) pre-cancerous lesions.
“The latest version of the software has saved over 1,000 face-to-face consultations in the secondary care setting between April 2022 and January 2023, freeing up more time for patients that need urgent attention,” Andrew said in the press release.
Still, the researchers admit that AI should not be used as the only detection method for skin cancers.
“We would like to stress that AI should not be used as a standalone tool in skin cancer detection and that AI is not a substitute for consultant dermatologists,” stated Irshad Zaki, B Med Sci (Hons), Consultant Dermatologist at University Hospitals Birmingham NHS Foundation Trust and one of the authors of the study, in the press release.
“The role of AI in dermatology and the most appropriate pathway are debated. Further research with appropriate clinical oversight may allow the deployment of AI as a triage tool,” said Andrew in the press release. “However, any pathway must demonstrate cost-effectiveness, and AI is currently not a stand-alone tool in dermatology. Our data shows the great promise of AI in future provision of healthcare.”
Two People in the US Die of Skin Cancer Every Hour
According to the Skin Cancer Foundation, skin cancer is the most common cancer in the United States as well as the rest of the world. More people in the US are diagnosed with skin cancer every year than all other cancers combined.
When detected early, the five-year survival rate for melanoma is 99%, but more than two people in the US die of skin cancer every hour. At least one in five Americans will develop skin cancer by the age of 70 and more than 9,500 people are diagnosed with the disease every day in the US.
The annual cost of treating skin cancers in the United States is estimated at $8.1 billion annually, with approximately $3.3 billion of that amount being for melanoma and the remaining $4.8 billion for non-melanoma skin cancers.
More research is needed before University Hospitals Birmingham’s new AI model can be used clinically in the diagnoses of skin cancers. However, its level of accuracy is unprecedented in AI diagnostics. This is a noteworthy step forward in the field of AI for diagnostic purposes that can be used by clinical laboratories and dermatopathologists.
Clinical laboratories and pathology groups should be on the alert to this new digital threat; telehealth sessions and video conferencing calls particularly vulnerable to acoustic AI attacks
Banks may be the first to get hit by a new form of hacking because of all the money they hold in deposit accounts, but experts say healthcare providers—including medical laboratories—are comparably lucrative targets because of the value of patient data. The point of this hacking spear is artificial intelligence (AI) with increased capabilities to penetrate digital defenses.
AI is developing rapidly. Are healthcare organizations keeping up? The hackers sure are. An article from GoBankingRates titled, “How Hackers Are Using AI to Steal Your Bank Account Password,” reveals startling new AI capabilities that could enable bad actors to compromise information technology (IT) security and steal from customers’ accounts.
Though the article covers how the AI could conduct cyberattacks on bank information, similar techniques can be employed to gain access to patients’ protected health information (PHI) and clinical laboratory databases as well, putting all healthcare consumers at risk.
The new AI cyberattack employs an acoustic Side Channel Attack (SCA). An SCA is an attack enabled by leakage of information from a physical computer system. The “acoustic” SCA listens to keystrokes through a computer’s microphone to guess a password with 95% accuracy.
“With recent developments in deep learning, the ubiquity of microphones and the rise in online services via personal devices, acoustic side channel attacks present a greater threat to keyboards than ever,” wrote UK study authors Joshua Harrison, MEng, Durham University; Ehsan Toreini, University of Surrey; and Maryam Mehrnezhad, PhD, University of London.
Hackers could be recording keystrokes during video conferencing calls as well, where an accuracy of 93% is achievable, the authors added.
This nefarious technological advance could spell trouble for healthcare security. Using acoustic SCA attacks, busy healthcare facilities, clinical laboratories, and telehealth appointments could all be potentially compromised.
“The ubiquity of keyboard acoustic emanations makes them not only a readily available attack vector, but also prompts victims to underestimate (and therefore not try to hide) their output,” wrote Joshua Harrison, MEng (above), and his team in their IEEE Xplore paper. “For example, when typing a password, people will regularly hide their screen but will do little to obfuscate their keyboard’s sound.” Since computer keyboards and microphones in healthcare settings like hospitals and clinical laboratories are completely ubiquitous, the risk that this AI technology will be used to invade and steal patients’ protected health information is high. (Photo copyright: CNBC.)
Why Do Hackers Target Healthcare?
Ransomware attacks in healthcare are costly and dangerous. According to InstaMed, a healthcare payments and billing company owned by J.P. Morgan, healthcare data breaches increased to 29.5% in 2021 costing over $9 million. And beyond the financial implications, these attacks put sensitive patient data at risk.
Healthcare can be seen as one of the most desirable markets for hackers seeking sensitive information. As InstaMed points out, credit card hacks are usually quickly figured out and stopped. However, “medical records can contain multiple pieces of personally identifiable information. Additionally, breaches that expose this type of data typically take longer to uncover and are harder for an organization to determine in magnitude.”
With AI advancing at such a high rate, healthcare organizations may be unable to adapt older network systems quickly—leaving them vulnerable.
“Legacy devices have been an issue for a while now,” Alexandra Murdoch, medical data analyst at GlobalData PLC, told Medical Device Network, “Usually big medical devices, such as imaging equipment or MRI machines are really expensive and so hospitals do not replace them often. So as a result, we have in the network these old devices that can’t really be updated, and because they can’t be updated, they can’t be protected.”
But telehealth, according to the UK researchers, may also be one way hackers get past safeguards and into critical hospital systems.
“When trained on keystrokes recorded using the video-conferencing software Zoom, an accuracy of 93% was achieved, a new best for the medium. Our results prove the practicality of these side channel attacks via off-the-shelf equipment and algorithms,” the UK researchers wrote in IEEE Xplore.
“[AI] has worrying implications for the medical industry, as more and more appointments go virtual, the implications of deepfakes is a bit concerning if you only interact with a doctor over a Teams or a Zoom call,” David Higgins, Senior Director at information security company CyberArk, told Medical Device Network.
Higgins elaborated on why healthcare is a highly targeted industry for hackers.
“For a credit card record, you are looking at a cost of one to two dollars, but for a medical record, you are talking much more information because the gain for the purposes of social engineering becomes very lucrative. It’s so much easier to launch a ransomware attack, you don’t even need to be a coder, you can just buy ransomware off of the dark web and use it.”
Steps Healthcare Organizations Should Take to Prevent Cyberattacks
Hackers will do whatever they can to get their hands on medical records because stealing them is so lucrative. And this may only be the beginning, Higgins noted.
“I don’t think we are going to see a slowdown in attacks. What we are starting to see is that techniques to make that initial intrusion are becoming more sophisticated and more targeted,” he told Medical Device Network. “Now with things like AI coming into the mix, it’s going to become much harder for the day-to-day individual to spot a malicious email. Generative AI is going to fuel more of that ransomware and sadly it’s going to make it easier for more people to get past that first intrusion stage.”
To combat these attacks patient data needs to be encrypted, devices updated, and medical staff well-trained to spot cyberattacks before they get out of hand. These SCA attacks on bank accounts could be easily transferable to attacks on healthcare organizations’ patient records.
Clinical laboratories, anatomic pathology groups, and other healthcare facilities would be wise to invest in cybersecurity, training for workers, and updated technology. The hackers are going to stay on top of the technology, healthcare leaders need to be one step ahead of them.
This pioneering innovation is consistent with the trend to bring medical services to places more convenient for consumers and was spurred by a study which showed men twice as likely to have heart attacks than women
Patient-facing healthcare gets a boost with this novel program to offer a diagnostic service in locations frequented by men. In an attempt to decrease heart attacks in the UK, the country’s National Health Service (NHS) now employs a novel approach to prevention—bringing blood pressure screenings to the public in barbershops.
This is yet another example of moving diagnostics services out of traditional healthcare settings and reaching people in places that they visit in their daily lives. True, this is a blood pressure test. But once the service is established, it should be easy to collect other types of clinical laboratory specimens at barbershops as well. And if this approach enables healthcare policy makers to reach a population that needs further diagnostic tests—and it’s economically feasible—that may encourage adoption of this approach for other types of health screenings.
According to The Guardian, the screenings will be available at “barbershops, churches, mosques, community centers, and dominoes clubs.” The intention is to ensure screenings are more accessible, to educate the public, and to encourage lifestyle changes that lead to prevention.
This consumer-directed approach to healthcare by the NHS appears to be making a difference. The new screening locations already show promise. In 2023, efforts brought in 150,000 community-based blood pressure screenings by August. That more than doubled the previous year’s 58,000 that were performed by May, The Guardian noted.
“With the number of people living with major illnesses including heart disease and other cardiovascular conditions set to grow substantially over the coming years, it has never been more important to put in place preventive measures like easy-to-access blood pressure checks that can pick up the early signs and risks,” said David Webb (above), Chief Pharmaceutical Officer for England, NHS England, in a news release. Should this program succeed, it’s likely other types of clinical laboratory test specimens could also be collected in barbershops and other convenient locations. (Photo copyright: Paul Stuart/The Pharmaceutical Journal.)
Importance of Screening
According to the UK’s Health Foundation, more than 9.1 million people will have a major illness by 2040, and figures show an increase of 2.5 million from 2019 reports. These figures are “why prevention and early intervention tools such as community blood pressure checks are key priorities for the NHS,” the NHS news release states.
“Having high blood pressure raises the risk of a heart attack, but many men and women remain unaware they may be affected because typically there are no symptoms,” The Guardian reported. “Every year there are 100,000 NHS hospital admissions due to heart attacks—one every five minutes.”
The NHS’ moves were spurred by recent findings announced at the European Society of Cardiology’s 2023 annual meeting. The world’s largest heart conference showcased a 22-year-long study examining the gender-specific risks of cardiovascular diseases. The results clearly showed that men were twice as likely to experience heart attacks and peripheral artery disease than women.
The University of Aberdeen conducted the study which ran from 1993-2018 and followed 20,000 individuals over the age of 40. While researchers noted many factors—such as ethnicity, body mass index (BMI), physical activity, deprivation, consumption of alcohol, and cigarette smoke—a clear defining line landed between male and female participants, The Guardian reported. Additionally,“Men are also more likely to experience a heart attack at a younger age than women.”
And, according to the study, while cardiovascular disease was higher for men during their entire lifetime, “sex differences were most pronounced for myocardial infarction and peripheral artery disease, followed by atrial fibrillation, heart failure, and cardiovascular mortality,” The Guardian reported, adding, “Men also have a 50% higher risk of heart failure and atrial fibrillation. The study discovered that men have a 42% higher risk of dying from cardiovascular disease. The research did not look at why.”
Education Part of Prevention
“Men should start looking early at-risk factors, like obesity, lack of exercise, smoking, alcohol consumption, and reach out to their GP to get those things addressed. The earlier the better. There’s no harm in minimizing your cardiovascular risk,” Tiberiu Pana, MRes, lead researcher and honorary research fellow at the University of Aberdeen, told The Guardian. Pana is also a junior doctor in the NHS and focuses on cardiovascular epidemiology and the brain-heart interactions.
“Coronary heart disease is the most common killer of men. There’s never been a better time to get physically active and replace that pub session with an extra session in the gym,” cardiologist Sonya Babu-Narayan, MBBS, Associate Medical Director at the British Heart Foundation, told The Guardian. Babu-Narayan is also a consultant cardiologist at Royal Brompton Hospital.
Women, however, are not exempt from the risk of heart disease.
“If we consider the effects of heart disease over a lifetime, we need to remember that it costs lives for both men and women,” Babu-Narayan said. “With 30,000 women in the UK admitted to hospital with a heart attack each year, it is vital to dismantle the dogma that heart attacks are the preserve of men. Regardless of gender, cardiovascular disease is the world’s biggest killer and there are steps everyone can take to reduce their risks.”
In addition to the aforementioned community locations for screenings, NHS has launched a few other approaches to meet patients on their own turf.
A mobile blood pressure service named How’s Thi Ticker in Barnsley, South Yorkshire, “travels around local neighborhoods including to barber shops, supermarkets, and community centers, seeing more than a third of people referred to pharmacists with high blood pressure—freeing up GPs and catching early signs of heart attack and stroke risk,” according to the NHS news release.
Future Showing Further Promise
As the process continues, NHS expects to prevent 1,350 cardiovascular events every year, and expects to see 2.5 million more blood pressure checks performed in the community in England as a result of the endeavor, The Guardian noted.
One can only imagine how far this trend can go. Clinical laboratory managers and pathologists can expect healthcare policy makers in the UK to continue their efforts to bring needed diagnostic testing to underserved populations in accessible ways. This should be a win-win financially and in improving the health of the country’s population.
Nationwide, hospital losses are in the billions of dollars, which affects access to medical care including clinical laboratory testing
Hospitals and health systems across the United States continue to report substantial financial losses. At some institutions, this might severely restrict access to physicians and clinical laboratory testing for patients in those areas. The latest state to announce its hospitals were in trouble is Minnesota. The Minnesota Hospital Association (MHA) announced its hospitals are in “financial crisis” revealing that the state’s health systems experience hundreds of millions of dollars in operating losses annually.
The MHA stated that two out of three surveyed hospitals in Minnesota reported losing money in the cumulative amount of more than $400 million during the first half of 2023, KARE 11 reported. The MHA surveyed more than 70 health system members which represented facilities of all sizes and in all geographical regions of the state.
Rahul Koranne, MD, President and CEO of MHA told KARE 11 that part of the problem is that a larger proportion of patients rely on federal programs such as Medicare and Medicaid to pay hospital costs. Those programs provide lower reimbursement rates when compared to private insurers. In some facilities, almost 75% of patients are on one of these government programs.
“Those reimbursements, or payments, are fixed. So, we can’t raise prices. These two programs are paying significantly below the cost of providing care to our patients,” he noted. “So, if you have 70% of your patients covered by these governmental programs, we can’t raise prices, and they’re paying you below the cost of care—that’s what causes [the problem].”
He went on to state that workforce staffing represents a significant challenge for hospitals and urged the state legislature to address the needs of health professionals and facilities.
“We need to really resource it in this upcoming session and many sessions to come, so that we can have workers and staff we need,” Koranne said. “If we don’t have the money, and if we don’t have the workers, we will not be providing care and that would be sad.”
“This is a pretty grave state and, I would say, quite a crisis,” Rahul Koranne, MD (above), President and CEO of the Minnesota Hospital Association, told KARE 11. “Our not-for-profit hospitals and healthcare systems are hanging dangerously from this cliff and they’re getting tired.” Access to medical laboratory testing can be greatly affected by hospital financial losses. (Photo copyright: Twin Cities Business.)
Other US Healthcare Systems in Crisis as Well
Minnesota is not the only state with healthcare systems in financial crisis. Last year, the Washington State Hospital Association (WSHA) announced that hospitals in that state reported cumulative losses of $2 billion for 2022. Cassie Sauer, President and CEO of WSHA told the media that the massive deficits are “clear and incredibly concerning” to the state’s healthcare leaders.
In “Hospitals, Pharmacies Struggle to Be Profitable,” we reported that the WSHA survey determined that the state’s hospitals suffered collective operating losses of $750 million during the first six months of 2023.
“The financial losses that our hospitals are experiencing continue to be enormous,” Sauer told The Seattle Times. “Revenues simply are not keeping up with rapidly escalating costs. It’s most concerning as these large losses are putting patient care at risk in many communities across the state.”
The WSHA findings were based on a survey of 81 acute-care hospitals that represented about 98% of the state’s hospital beds. Of those facilities, 69 reported losing money mostly due to rising costs for supplies, labor, and other expenses as well as the need for longer hospital stays due to more complicated care and a larger percentage of patients on government programs, which offer lower reimbursement rates for care.
“When hospitals are not financially viable and over time sustain heavy losses, you must either increase revenue or reduce healthcare services,” Chelene Whiteaker, Senior Vice President, Government Affairs at WSHA, told The Seattle Times. “Reducing healthcare services is an option nobody wants on the table. So, that leaves increasing revenues.”
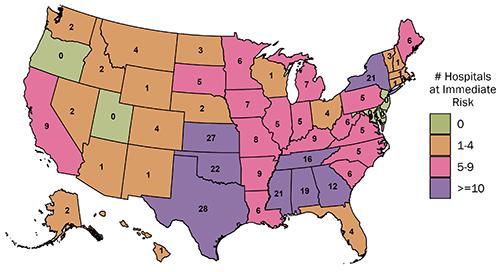
The graphic above from the Center for Healthcare Quality and Payment Reform (CHQPR) shows the number and location of rural hospitals in America that are at “immediate” risk of closure. The number of hospitals simply “at risk” of closure is substantially higher. Patients who depend on these hospitals would lose access to critical healthcare services including clinical laboratory testing. (Graphic copyright: Center for Healthcare Quality and Payment Reform.)
Becker’s Hospital Review reported last year that many hospitals across the country reported substantial losses in 2022. Three of the hospital systems in that article reported losses in the billions. They were:
In another article, Becker’s reported that 72 hospitals across the US closed departments or ended services in 2023. These cuts included the shuttering of health and urgent care clinics, the closure of outpatient cancer and pulmonary clinics, the reduction of certain surgical services and behavioral health services, and the ending of home healthcare services.
Some states are taking measures to prevent further hospital closures. But is it too late? In “California Doles Out $300 Million in No-Interest Loans to Save its Financially Struggling Hospitals,” The Dark Report’s sister publication Dark Daily covered how that state had launched an interest-free loan program to ensure local communities have access to community hospitals, their physicians, and clinical laboratories. No report on how many hospitals have been temporarily saved from closing thanks to this program.
If US hospitals continue to lose money at this rate, access to critical care—including clinical laboratory and anatomic pathology services—could be further restricted and facilities closed. These actions may also result in increased staff layoffs and have an even greater effect on patient care in Minnesota, Washington State, and throughout the US.