This is good news for clinical laboratories that already perform medical testing for telehealth providers and an opportunity for medical labs that do not, it is an opportunity to do so
Telemedicine visits have become commonplace since the arrival of COVID-19. Before the pandemic, telehealth was primarily used to give remote patients access to quality healthcare providers. But three years later both patients and physicians are becoming increasingly comfortable with virtual office visits, especially among Millennial and Gen Z patients and doctors.
Now, a recent study by the Perelman School of Medicine at the University of Pennsylvania (Penn Medicine) suggests that there could be a significant financial advantage for hospitals that conduct telemedicine. This would be a boon to clinical laboratories that perform medical testing for telemedicine providers.
According to Digital Health News, in July 2017 Penn Medicine launched a 24/7/365 copayment-free telemedicine program for its employees called Penn Medicine OnDemand. To engage with a telemedicine provider, patients must have a smartphone or tablet with a front-facing camera and updated operating system.
Telemedicine Visits Cost Less than In-Office Doctor Appointments
An analysis of the OnDemand program’s data collected from its inception through the end of 2019 found that the telemedicine appointment per-visit cost averaged around $380, whereas the cost of an in-person visit at an emergency department, primary care office, or urgent care clinic averaged around $493.
Typically, Penn Medicine’s employees used the telemedicine program for common, low risk health complaints. Healthcare conditions that many patients might otherwise not seek treatment for if an in-office visit was inconvenient.
“The data we analyzed pre-date the pandemic. It was a time when people were just putting a toe in the water and wondering, ‘Let me see if telemedicine could treat my needs,’” Krisda Chaiyachati MD, an internal medicine physician and Adjunct Assistant Professor at Penn Medicine, told Digital Health News. Chaiyachati lead the research team that conducted the telemedicine study.
“These days, people seem willing to jump in for an appropriate set of conditions,” he added. “The good news is that we made care easier while saving money, and we think the savings could be higher in the future.”
Chaiyachati and his colleagues found that telemedicine can save employers healthcare costs without sacrificing quality of care.
“The conditions most often handled by OnDemand are low acuity—non-urgent or semi-urgent issues like respiratory infections, sinus infections, and allergies—but incredibly common, so any kind of cost reduction can make a huge difference for controlling employee benefit costs,” Krisda Chaiyachati MD (above), a Penn Medicine physician and the study’s lead researcher, told Digital Health News. Clinical laboratories that already perform testing for telemedicine providers may see an increase in test orders once hospitals learn of the costs savings highlighted in the Penn Medicine study. (Photo copyright: Penn Medicine.)
Telemedicine on the Rise
The idea is not new. In late 2018, Planned Parenthood launched the Planned Parenthood Direct mobile app in New York State. The app provides New York patients with access to birth control, emergency contraception, and UTI treatment with no in-person visit required.
The program has since expanded across the country. Users of the app can connect with a physician to go over symptoms/needs, and the be sent a prescription within a business day to the pharmacy of their choice.
The concept is similar to Penn Medicine OnDemand, which gives patients 24/7 year around access to treatment for common and low-acuity medical issues in a convenient, virtual process.
Telemedicine was on the rise in other parts of the healthcare industry before the pandemic. According to “The State of Telehealth Before and After the COVID-19 Pandemic” published by Julia Shaver, MD, Kaiser Permanente, in the journal Primary Care: Clinics in Office Practice, 76% of US hospital systems had utilized some form of telemedicine by 2018. This rate grew exponentially while the healthcare system had to navigate a world with COVID-19 on the rise.
And, apparently, quality of care does not suffer when moved from in-person to virtual settings. Two studies conducted by The University of Rochester Medical Center (URMC) found telemedicine to be effective and that “common concerns about telemedicine don’t hold up to scrutiny,” according a news release.
In her New England Journal of Medicine (NEJM) paper on the studies, Kathleen Fear, PhD, URMC’s Director of Data Analytics, Health Lab, and her co-authors, wrote: “Three beliefs—that telemedicine will reduce access for the most vulnerable patients; that reimbursement parity will encourage overuse of telemedicine; and that telemedicine is an ineffective way to care for patients—have for years formed the backbone of opposition to the widespread adoption of telemedicine.”
However, URMC’s study found the opposite to be true. The NEJM authors wrote, “there is no support for these three common notions about telemedicine. At URMC, the most vulnerable patients had the highest uptake of telemedicine; not only did they complete a disproportionate share of telemedicine visits, but they also did so with lower no-show and cancellation rates. It is clear that … telemedicine makes medical care more accessible to patients who previously have experienced substantial barriers to care.
“Importantly, this access does not come at the expense of effectiveness. Providers do not order excessive amounts of additional testing to make up for the limitations of virtual visits. Patients do not end up in the ER or the hospital because their needs are not met during a telemedicine visit, and they also do not end up requiring additional in-person follow-up visits to supplement their telemedicine visit,” the NEJM authors concluded.
“Not only did our most vulnerable patients not get left behind—they were among those engaging the most with, and benefiting the most from, telemedicine services. We did not see worse outcomes or increased costs, or patients needing an increased amount of in-person follow up. Nor did we find evidence of overuse. This is good care, and it is equitable care for vulnerable populations,” Fear said in the news release.
“For patients, the message is clear and reassuring: Telemedicine is an effective and efficient way of receiving many kinds of healthcare,” she added.
Opportunities for Clinical Laboratories
Dark Daily has covered the fast growing world of telemedicine in many ebriefs over the years.
As telemedicine broadens its reach across the healthcare world, clinical laboratories and pathology groups would be wise to seek collaboration with health plans and providers of telemedicine to figure out where sample collection and testing fits into this new virtual healthcare space.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
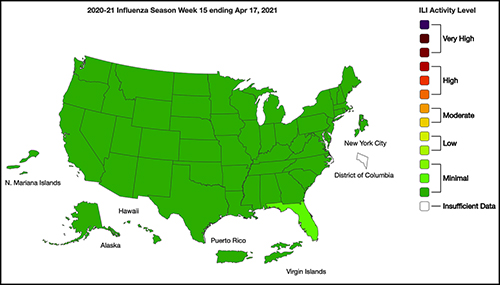
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
Clinical laboratories must stay informed about the success of bundled-payment initiatives because they will need to negotiate a share of these payments where medical laboratory testing is involved
Research published this year concluded that bundled payments for joint replacement services performed on Medicare patients reduce Medicare’s costs without negatively affecting patient outcomes. Because these types of surgeries do not generally utilize many lab tests, the question is still out as to whether bundled payments allow clinical laboratories to be adequately reimbursed for their services.
The study of the bundled payment program was published in the Journal of the American Medical Association (JAMA). The researchers sought to determine the cause of the reduction in Medicare payments and hospital savings when bundled payment models for joint replacement surgeries were used.
The research was performed by staff at the Perelman School of Medicine at the University of Pennsylvania (UPenn). They examined hospital costs and Medicare claims for patients requiring hip and knee replacements at the 5-hospital Baptist Health System (BHS) in San Antonio. (more…)
Clinical laboratories and pathology groups can benefit from developing a strategy for addressing negative Yelp reviews
In today’s wired world, clinical laboratories and anatomic pathology groups have a new challenge: what to do when unhappy patients go to social networking sites and post comments about their negative experience with their lab. A lab can have a sterling reputation for service and it can all unravel if a vociferous and angry patient posts rants on the Internet.
Today’s reality is that, like them or not, online reviews posted on websites such as Yelp are here to stay. That is why medical lab managers and pathologists should know about a recent court ruling that protects websites that feature consumer reviews about businesses.
One business owner who sued such a website learned this out the hard way—in court. A locksmith in Redmond, Wash., reportedly filed a libel lawsuit, claiming he lost 95% of his business after receiving a negative 1-star review on Yelp. Regardless, a federal appeals court ruled that Yelp’s star rating system, which is based on user input, does not make Yelp responsible for negative reviews of businesses, the Chicago Tribune reported. (more…)