Legal actions highlight ongoing concerns about payer behavior and included a record-breaking settlement in antitrust case against Blue Cross and Blue Shield
Several high-profile federal lawsuits filed last year, along with settlements in older cases, demonstrate that providers, patients, and self-insured employers—including hospitals, clinical laboratories, and anatomic pathology groups—continue to have serious concerns about lack of transparency and certain business practices of health plans.
Self-Insured employers are suing because they cannot see their data and discovered their health plans overpaid providers from allowed charges (meaning a self-insured employer has greater health benefit costs).
Providers are suing because they are being paid less than agreed and have claims denied for spurious reasons.
These lawsuits show that there is increasing ill will and concerns by self-insured employers and providers as to how health insurers are properly conducting business.
Below is a rundown of the cases.
“Over the past 12 years we have dedicated an extraordinary amount of time, tireless effort, and resources to this historic outcome for providers,” said Co-Lead Counsel Edith Kallas, JD, of Whatley Kallas, a press release. The Blue Cross and Blue Shield Association settlement with healthcare providers is the largest healthcare-related antitrust settlement in US history, according to plaintiff’s attorney Whatley Kallas, LLP. Clinical laboratories and pathology groups can learn from these lawsuits. (Photo copyright: Whatley Kallas.)
BCBSA Settles Long-Running Antitrust Case
In October, the Blue Cross and Blue Shield Association (BCBSA) and the 33 independent Blue Cross and Blue Shield (BCBS) plans agreed to a $2.8 billion settlement in a 12-year-old federal antitrust lawsuit. Co-counsel for the plaintiffs Whatley Kallas, LLP, described the agreement as the “largest antitrust settlement in the history of the United States healthcare industry.”
Healthcare providers alleged that the BCBS plans had agreed “to allocate markets through the use of exclusive service areas and to fix the prices paid to providers through the BlueCard Program,” according to a news release.
In addition to the cash payment, the health plans also agreed to “invest hundreds of millions of dollars in system improvements for the benefit of providers,” the law firm noted, adding that the settlement would compel changes in how the plans “process claims, communicate with, and make payments to healthcare providers,” helping to “address resource-draining administrative burdens and inefficiencies currently experienced by providers.”
Whatley Kallas said the settlement would ultimately result in injunctive relief amounting to $17.3 billion during its first 10 years.
“Many important issues for providers are finally being addressed,” said Edith Kallas, JD, of Whatley Kallas in the news release. “We’re pleased that we have been able to achieve relief that will create a better system for healthcare providers and that will support the organizations and people we rely on to take care of us and our families every day.”
BCBSA also issued a statement: “This settlement ends a long-running legal challenge to the Blue Cross Blue Shield Association license agreements and related rules. We deny the allegations made in the lawsuit. However, to reach a settlement and put years of litigation behind us, we have agreed to make some operational changes and a monetary payment to the provider class involved in the case.”
As explained in court documents, plaintiff Sandra M. Peters was covered by an ERISA plan self-funded by Mars Inc. and administered by Aetna. The latter contracted with Optum to provide access to physical therapy, occupational therapy, and chiropractic services.
Peters alleged that Aetna, in collusion with Optum, fraudulently disguised the latter’s administrative fees as medical costs.
“These misrepresentations serve as the cover that allows Aetna to illegally (i) obtain payment of the Subcontractors’ administrative fees directly from insureds when the insureds’ deductibles have not been reached; (ii) use insureds’ health spending accounts to pay for these fees; (iii) inflate insureds’ co-insurance obligations using administrative fees; (iv) artificially reduce the amount of available coverage for medical services when such coverage is subject to an annual cap; and (v) obtain payment of the administrative fees directly from employers when an insured’s deductible has been exhausted or is inapplicable,” stated her original complaint, filed in 2015 in the US District Court for the Western District of North Carolina.
On Nov. 6, attorneys for Peters notified the court that they had settled the case. A month later, Optum said it had withdrawn from the settlement and was prepared to go to trial. Then, the parties appeared to resolve their remaining differences, and Peters’ attorneys filed notice on Dec. 17 that they had once again settled, Mealey’s reported. Terms of the settlement were not disclosed.
Owens and Minor Alleges Mismanagement of Self-Funded Plan
As reported by The Dark Report and various news outlets, Owens and Minor, a healthcare logistics company, filed a lawsuit in November against Anthem BCBS of Virginia, which had been administering Owens’ self-funded employee health plan since 2017.
The complaint further stated that “Defendant acted contrary to the fiduciary standards imposed by ERISA by, among other things, (i) paying more for healthcare claims than was even billed, (ii) securing kickbacks from providers, (iii) double-paying claims, and (iv) pocketing rebates belonging to Plaintiff.”
Owens initially requested plan data from Anthem in September 2021, but Anthem refused to do so, the complaint stated. “Eventually, Plaintiff had to sue Defendant to obtain its own data. Now that Plaintiff has a portion of that Plan data and has had the opportunity to analyze it, it is clear why Defendant fought so hard to prevent Plaintiff from accessing it.”
Becker’s Payer Issues noted that the lawsuit “reflects a wider legal trend for employers and health plan administrators navigating ERISA requirements. Under the law, plan fiduciaries must act in the best interests of beneficiaries by seeking the lowest reasonable costs for services. Recent amendments, such as the Consolidated Appropriations Act of 2021, have heightened transparency requirements, leaving employers with new tools—and new pressures—to ensure compliance.”
DOJ Alleges Overcharges Related to Military Managed Care
On March 13, the US Department of Justice (DOJ) announced that it had sued six health plans that participate in the Uniformed Services Family Health Plan (USFHP) program, which provides health benefits to military retirees and their families. The government alleged that the plans were aware of calculation errors that had inflated payment rates by more than $300 million between 2008 and 2012.
“The Plans failed to report or return any of those overpayments and, in fact, continued submitting claims to the government at the improperly inflated rates for several more months,” the complaint states.
Shortly after filing the lawsuit, US Family Health Plan Alliance issued a statement describing the allegations as “meritless,” Becker’s Payer Issues reported. The group said that the plans and the government had “expressly negotiated [payment rates] in a fixed-rate contract more than 10 years ago.”
These developments are clear signals in the market that self-insured employers, along with providers—including physicians, hospitals, and medical laboratories—have growing evidence that certain health insurance companies are gaming the system and not paying claims according to contractual arrangements. Expect to see more lawsuits against health plans, particularly by self-insured employers because, for them, the sums involved can be in the tens of millions of dollars.
Initially thought to be an attack by a nation-state, actual culprit turned out to be a known ransomware group and each day brings new revelations about the cyberattack
Fallout continues from cyberattack on Change Healthcare, the revenue cycle management (RCM) company that is a business unit of Optum, itself a division of UnitedHealth Group. Recent news accounts say providers are losing an estimated $100 million per day because they cannot submit claims to Change Healthcare nor receive reimbursement for these claims.
The cyberattack took place on February 21. The following day, UnitedHealth Group filed a Material Cybersecurity Incidents report (form 8-K) with the US Securities and Exchange Commission (SEC) in which it stated it had “identified a suspected nation-state associated cybersecurity threat actor [that] had gained access to some of the Change Healthcare information technology systems.”
A few days later the real identity of the threat actor was revealed to be a ransomware group known as “BlackCat” or “ALPHV,” according to Reuters.
Change Healthcare of Nashville, Tenn., is “one of the largest commercial prescription processors in the US,” Healthcare Dive reported, adding that hospitals, pharmacies, and military facilities had difficulty transmitting prescriptions “as a result of the outage.”
Change Healthcare handles about 15 billion payments each year.
According to a Change Healthcare statement, the company “became aware of the outside threat” and “took immediate action to disconnect Change Healthcare’s systems to prevent further impact.”
Change Healthcare has provided a website where parties that have been affected by the cyberattack can find assistance and updated information on Change’s response to the intrusion and theft of its data.
“The fallout is only starting to happen now. It will get worse for consumers,” Andrew Newman (above), founder and Chief Technology Officer, ReasonLabs, told FOX Business, adding, “We know that the likely destination for [the Change Healthcare] data is the Dark Web, where BlackCat will auction it all off to the highest bidder. From there, consumers could expect to suffer from things like identity theft, credit score downgrades, and more.” Clinical laboratories are also targets of cyberattacks due to the large amount of private patient data stored on their laboratory information systems. (Photo copyright: ReasonLabs.)
Millions of Records May be in Wrong Hands
Reuters reported that ALPHV/BlackCat admitted it “stole millions of sensitive records, including medical insurance and health data from the company.”
The ransomware group has been focusing its attacks on healthcare with 70 incidents since December, according to federal agencies.
In a letter to HHS, AHA warned, “Change Healthcare’s downed systems will have an immediate adverse impact on hospital finances. … Their interrupted technology controls providers’ ability to process claims for payment, patient billing, and patient cost estimation services.”
“My understanding is Change/Optum touches almost every hospital in the US in one way or another,” John Riggi, AHA’s National Advisor for Cybersecurity and Risk, told Chief Healthcare Executive. “It has sector wide impact in potential risk. So, really, this is an attack on the entire sector.” Riggi spent nearly 30 years with the FBI.
Some physician practices may also have been impacted by the Change Healthcare cyberattack, according to the Medical Group Management Association (MGMA). In a letter to HHS, MGMA described negative changes in processes at doctors’ offices. They include delays in paper and electronic statements “for the duration of the outage.”
In addition, “prescriptions are being called into pharmacies instead of being electronically sent, so patients’ insurance information cannot be verified by pharmacies, and [the patients] are forced to self-pay or go without necessary medication.”
Here are “just a few of the consequences medical groups have felt” since the Change Healthcare cyberattack, according to the MGMA:
Substantial billing and cash flow disruptions, such as a lack of electronic claims processing. Both paper and electronic statements have been delayed. Some groups have been without any outgoing charges or incoming payments for the duration of the outage.
Limited or no electronic remittance advice from health plans. Groups are having to manually pull and post from payer portals.
Prior authorization submissions have been rejected or have not been transmittable at all. This further exacerbates what is routinely ranked the number one regulatory burden by medical groups and jeopardizes patient care.
Groups have been unable to perform eligibility checks for patients.
Many electronic prescriptions have not been transmitted, resulting in call-in prescriptions to pharmacies or paper prescriptions for patients. Subsequently, patients’ insurance information cannot be verified by pharmacies, and they are forced to self-pay or go without necessary medication.
Lack of connectivity to important data infrastructure needed for success in value-based care arrangements, and other health information technology disruptions.
Medical laboratory leaders and pathologists are advised to consult with their colleagues in IT and cybersecurity on how to best prevent ransomware attacks. Labs hold vast amount of private patient information. Recent incidents suggest more steps and strategies may be needed to protect laboratory information systems and patient data.
The speakers also noted that labs must learn to work collaboratively with payers—perhaps through health information technology (HIT)—to establish best practices that improve reimbursements on claims for novel genetic tests.
Harnessing the ever-increasing volume of diagnostic data that genetic testing produces should be a high priority for labs, said William Morice II, MD, PhD, CEO and President of Mayo Clinic Laboratories.
“There will be an increased focus on getting information within the laboratory … for areas such as genomics and proteomics,” Morice told the keynote audience at the Executive War College on Wednesday.
“Wearable technology data is analyzed using machine learning. Clinical laboratories must participate in analyzing that spectrum of diagnostics,” said William Morice II, MD, PhD (above), CEO and President of Mayo Clinic Laboratories. Morice spoke during this week’s Executive War College.
Precision Medicine Efforts Include Genetic Testing and Wearable Devices
For laboratories new to genetic testing that want to move it in-house, Morice outlined effective first steps to take, including the following:
Determine and then analyze the volume of genetic testing that a lab is sending out.
Research and evaluate genetic sequencing platforms that are on the market, with an eye towards affordable cloud-based options.
Build a business case to conduct genetic tests in-house that focuses on the long-term value to patients and how that could also improve revenue.
A related area for clinical laboratories and pathology practices to explore is their role in how clinicians treat patients using wearable technology.
For example, according to Morice, Mayo Clinic has monitored 20,000 cardiac patients with wearable devices. The data from the wearable devices—which includes diagnostic information—is analyzed using machine learning, a subset of artificial intelligence.
In one study published in Scientific Reports, scientists from Mayo’s Departments of Neurology and Biomedical Engineering found “clear evidence that direct seizure forecasts are possible using wearable devices in the ambulatory setting for many patients with epilepsy.”
Clinical laboratories fit into this picture, Morice explained. For example, depending on what data it provides, a wearable device on a patient with worsening neurological symptoms could trigger a lab test for Alzheimer’s disease or other neurological disorders.
“This will change how labs think about access to care,” he noted.
For Payers, Navigating Genetic Testing Claims is Difficult
While there is promise in genetic testing and precision medicine, from an administrative viewpoint, these activities can be challenging for payers when it comes to verifying reimbursement claims.
“One of the biggest challenges we face is determining what test is being ordered. From the perspective of the reimbursement process, it’s not always clear,” said Cristi Radford, MS, CGC, Product Director at healthcare services provider Optum, a subsidiary of UnitedHealth Group, located in Eden Prairie, Minnesota. Radford also presented a keynote at this year’s Executive War College.
Approximately 400 Current Procedural Terminology (CPT) codes are in place to represent the estimated 175,000 genetic tests on the market, Radford noted. That creates a dilemma for labs and payers in assigning codes to novel genetic tests.
During her keynote address, Radford showed the audience of laboratory executives a slide that charted how four labs submitted claims for the same high-risk breast cancer panel. CPT code choices varied greatly.
“Does the payer have any idea which test was ordered? No,” she said. “It was a genetic panel, but the information doesn’t give us the specificity payers need.”
In such situations, payers resort to prior authorization to halt these types of claims on the front end so that more diagnostic information can be provided.
“Plans don’t like prior authorization, but it’s a necessary evil,” said Jason Bush, PhD, Executive Vice President of Product at Avalon Healthcare Solutions in Tampa, Florida. Bush co-presented with Radford.
[Editor’s note: Dark Daily offers a free webinar, “Learning from Payer Behavior to Increase Appeal Success,” that teaches labs how to better understand payer behavior. The webinar features recent trends in denials and appeals by payers that will help diagnostic organizations maximize their appeal success. Click here to stream this important webinar.]
Payers Struggle with ‘Explosion’ of Genetic Tests
In “UnitedHealth’s Optum to Offer Lab Test Management,” Dark Daily’s sister publication The Dark Report, covered Optum’s announcement that it had launched “a comprehensive laboratory benefit management solution designed to help health plans reduce unnecessary lab testing and ensure their members receive appropriate, high-quality tests.”
Optum sells this laboratory benefit management program to other health plans and self-insured employers. Genetic test management capabilities are part of that offering.
As part of its lab management benefit program, Optum is collaborating with Avalon on a new platform for genetic testing that will launch soon and focus on identifying test quality, streamlining prior authorization, and providing test payment accuracy in advance.
“Payers are struggling with the explosion in genetic testing,” Bush told Executive War College attendees. “They are truly not trying to hinder innovation.”
For clinical laboratory leaders reading this ebriefing, the takeaway is twofold: Genetic testing and resulting precision medicine efforts provide hope in more effectively treating patients. At the same time, the genetic test juggernaut has grown so large so quickly payers are finding it difficult to manage. Thus, it has become a source of continuous challenge for labs seeking reimbursements.
Heath information technology may help ease the situation. But, ultimately, stronger communication between labs and payers—including acknowledgement of what each side needs from a business perspective—is paramount.
Executives and pathologists from many of the nation’s most prominent clinical laboratories are on their way to the Crescent City today to share best practices, hear case studies from innovative labs, and network
NEW ORLEANS—This afternoon, more than 900 lab CEOs, administrators, and pathologists will convene for the 28th Annual Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management conference. Three topics of great interest will center around adequate lab staffing, effective cost management, and developing new sources of lab testing revenue.
Important sessions will also address the explosion in next-generation sequencing and genetic testing, proposed FDA regulation of laboratory-developed tests (LDTs), and innovative ways that clinical laboratories and pathology groups can add value and be paid for that additional value.
All this is happening amidst important changes to healthcare and medicine in the United States. “Today, the US healthcare system is transforming itself at a steady pace,” explained Robert L. Michel, Editor-in-Chief of The Dark Report and Founder of the Executive War College. “Big multi-hospital health systems are merging with each other, and payers are slashing reimbursement for many medical lab tests, even as healthcare consumers want direct access to clinical laboratory tests and the full record of their lab test history.
“Each of these developments has major implications in how clinical laboratories serve their parent organizations, offer services directly to consumers, and negotiate with payers for fair reimbursement as in-network providers,” Michel added. “Attending the Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management equips lab leaders with the tools they’ll need to make smart decisions during these challenging times.”
Now in its 28th year, the Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management convenes April 25-26 in New Orleans. Executive War College extends to a third day with three full-day workshops: LEAN fundamentals for lab leaders, a genetic testing program track, and a digital pathology track. Learn more at www.ExecutiveWarCollege.com. (Photo copyright: The Dark Intelligence Group.)
Challenges and Opportunities for Clinical Laboratories
With major changes unfolding in the delivery and reimbursement of clinical services, clinical laboratory and pathology practice leaders need effective ways to respond to the evolving needs of physicians, patients, and payers. As The Dark Report has often covered, three overlapping areas are a source of tension and financial pressure for labs:
Day-to-day pressures to manage costs in the clinical laboratory or pathology practice.
The growing demand for genetic testing, accompanied by reimbursement challenges.
Evolving consumer expectations in how they receive medical care and interact with providers.
Addressing all three issues and much more, the 2023 Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management features more than 80 sessions with up to 125 lab managers, consultants, vendors, and in vitro diagnostic (IVD) experts as speakers and panelists.
Old-School Lab Rules Have Evolved into New-School Lab Rules
Tuesday’s keynote general sessions (to be reported exclusively in Wednesday’s Dark Daily ebriefing) will include four points of interest for clinical laboratory and pathology leaders who are managing change and pursuing new opportunities:
Positioning the lab to prosper by serving healthcare’s new consumers, new care models, new payment models, and more, with Michel at the podium.
How old-school lab rules have evolved into new-school lab rules and ways to transition the lab through today’s disrupters in healthcare and the clinical laboratory marketplace, with Stan Schofield, Managing Principal of the Compass Group.
Generating value by identifying risk signals in longitudinal lab data and opportunities in big data from payers, physicians, pharma, and bioresearch, with Brad Bostic, Chairman and CEO of hc1.
Wednesday’s keynote sessions (see exclusive insights in Friday’s Dark Daily ebriefing) explore:
Wednesday’s keynotes conclude with a panel discussion on delivering value to physicians, patients, and payers with lab testing services.
Clinical Labs, Payers, and Health Plans Swamped by Genetic Test Claims
Attendees of the 2023 Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management may notice a greater emphasis on whole genome sequencing and genetic testing this year.
As regular coverage and analysis in The Dark Report has pointed out, clinical laboratories, payers, and health plans face challenges with the explosion of genetic testing. Several Executive War College Master Classes will explore critical management issues of genetic and genomic testing, including laboratory benefit management programs, coverage decisions, payer relations, and best coding practices, as well as genetic test stewardship.
This year’s Executive War College also devotes a one-day intensive session on how community hospitals and local labs can set up and offer genetic tests and next-generation sequencing services. This third-day track features more than a dozen experts including:
During these sessions, attendees will be introduced to “dry labs” and “virtual CLIA labs.” These new terms differentiate the two organizations that process genetic data generated by “wet labs,” annotate it, and provide analysis and interpretation for referring physicians.
State of the Industry: Clinical Lab, Private Practice Pathology, Genetic Testing, IVD, and More
For lab consultants, executives, and directors interested in state-of-the-industry Q/A and discussions concerning commercial laboratories, private-practice pathology, and in vitro diagnostics companies, a range of breakout sessions, panels, and roundtables will cover:
Action steps to protect pathologists’ income and boost practice revenue.
Important developments in laboratory legal, regulatory, and compliance requirements.
New developments in clinical laboratory certification and accreditation, including the most common deficiencies and how to reach “assessment ready” status.
An update on the IVD industry and what’s working in today’s post-pandemic market for lab vendors and their customers.
Federal government updates on issues of concern to clinical laboratories, including PAMA, the VALID Act, and more.
Long-time attendees will notice the inclusion of “Diagnostics” into the Executive War College moniker. It’s an important addition, Michel explained for Dark Daily.
“In the recent past, ‘clinical laboratory’ and ‘anatomic pathology’ were terms that sufficiently described the profession of laboratory medicine,” he noted. “However, a subtle but significant change has occurred in recent years. The term ‘diagnostics’ has become a common description for medical testing, along with other diagnostic areas such as radiology and imaging.”
Key managers of medical laboratories, pathology groups, and in vitro diagnostics have much to gain from attending the Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, now in its 28th year. Look for continued coverage through social media channels, at Dark Daily, and in The Dark Report.
Multiple recent studies reveal a substantial number of patients continue to delay needed healthcare in the months since the onset of the SARS-CoV-2 outbreak
Based on an analysis of hospital emergency department (ED) usage, federal researchers concluded that patients continue to be cautious when visiting healthcare providers, including clinical laboratories, and that people are altering how they seek and utilize emergency care due to the COVID-19 pandemic. This not only reduces the number of typical test orders from the ER to the hospital lab, but also reduces the source of inpatient admissions.
Between March 29 and April 25 of this year, facilities the CDC examined recorded 1.2 million visits to EDs, compared to 2.1 million visits between March 31 and April 27 of last year. The steepest decrease in patient demographics was for individuals under the age of 14, women, and people living in the Northeast region.
The CDC’s data showed that 12% of ED visits were for children in pre-pandemic 2019, which dropped to 6% during the 2020 pandemic period. The CDC included ED visits from hospitals in 47 states (excluding Hawaii, South Dakota, and Wyoming) and captured information from approximately 73% of ED visits in the US.
Delaying Healthcare Visits Worsens Medical Conditions, Reduces Revenues
ED visits are an important referral source for inpatient admissions. Fewer patients in EDs means lost revenue for hospitals. However, one positive aspect of the waning number of ED visits is that it may be keeping patients with non-emergency situations away from emergency departments, thus reducing the overuse of costly ED visits. But healthcare professionals are concerned that individuals also may be avoiding or delaying care when needed, which could worsen medical situations and outcomes.
“We saw people, with COVID-19 and without, coming into the ED who were very ill,” Vik Reddy, MD, Chief Medical Officer at Wellstar Kennestone Hospital and Wellstar Windy Hill Hospital in the Atlanta area, told Modern Healthcare. He noted that some patients delayed care for critical non-COVID-19 illnesses. “The good news is that we’re seeing that trend reverse this time around. It was scary in March when we knew that people weren’t coming into the ED for heart attacks.”
The NSSP’s analysis concluded that the report’s findings were subject to at least four limitations:
The number of hospitals reporting to NSSP changes over time as facilities are added or closed. For example, 3,173 hospitals reported data in April of 2019, while 3,467 reported data in April 2020.
Diagnostic categories rely on the use of specific codes, which were missing in 20% of the ED visits reported.
NSSP coverage is not uniform across or within all the participating states.
The analysis is limited only to ED visits and does not take into account patients who did not go to an ED, but instead received treatment in other healthcare environments, such as urgent care clinics.
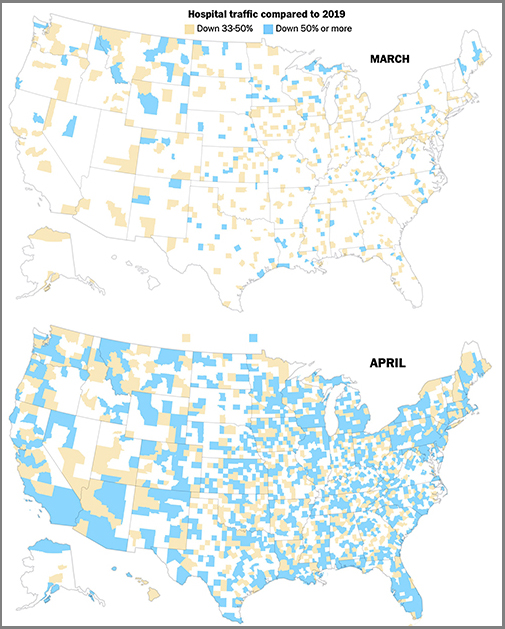
The graphics above are taken from a Washington Post article which reported that the newspaper’s analysis of smartphone location data of hospital traffic in 2020 showed the “drop” in hospital usage had turned into “a crash,” compared to the same two months last year, and that, “As in many other industries, those lost visits represented a widespread financial crisis for hospitals and other healthcare providers, even in places the novel coronavirus hardly touched.” (Graphics copyright: The Washington Post.)
Additional Studies Show Patients Avoiding Hospital EDs, Delaying Care
Other sources also are reporting similar findings regarding consumer attitudes towards seeking medical care during the COVID-19 pandemic. A PricewaterhouseCoopers survey released in May found that about 45% of 2,500 consumers surveyed plan to forgo their annual physical in 2020, due to the pandemic, Modern Healthcare reported.
In addition, an Optum Consumer Pulse Survey released in May found that nearly 20% of 700 surveyed individuals stated they were likely to avoid hospital EDs even if they were showing signs of a heart attack or appendicitis. Another 40% stated they were likely to avoid the ED if they had a cut that required stitches.
In “Americans Are Delaying Medical Care, and It’s Devastating Health-Care Providers,” The Washington Post analyzed hospital use during the pandemic based on smartphone tracking data. WaPo’s report found a significant drop in patients seeking in-person healthcare with many areas across the country reporting a 50% reduction in patients when compared to last year.
The article also states that almost 94 million people have delayed medical care due to the COVID-19 pandemic, and that 66 million of those individuals needed medical care unrelated to the virus but did not receive it.
These studies and others are showing a pattern. The COVID-19 pandemic has changed when and where patients access healthcare, and if the trend continues, it could have a long-term impact on clinical laboratories. Since fewer people are seeking medical care, fewer laboratory tests are being ordered and performed, which means less work and revenue for the nations’ hospital and independent clinical labs.