Researchers are discovering it’s possible to determine a person’s age based on the amount of protein in the blood, but the technology isn’t always correct
Mass spectrometry is increasingly finding its way into clinical laboratories and with it—proteomics—the study of proteins in the human body. And like the human genome, scientists are discovering that protein plays an integral part in the aging process.
This is a most interesting research finding. Might medical laboratories someday use proteomic biomarkers to help physicians gauge the aging progression in patients? Might this diagnostic capability give pathologists and laboratory leaders a new product line for direct-to-consumer testing that would be a cash-paying, fast-growing, profitable clinical laboratory testing service? If so, proteomics could be a boon to clinical laboratories worldwide.
When research into genomics was brand-new, virtually no one imagined that someday the direct-to-consumer lab testing model would offer genetic testing to the public and create a huge stream of revenue for clinical laboratories that process genetic tests. Now, research into protein and aging might point to a similar possibility for proteomics.
For example, through proteomics, researchers led by Benoit Lehallier, PhD, Biostatistician, Instructor of Neurology and Neurological Sciences, and senior author Tony Wyss-Coray, PhD, Professor of Neurology and Neurological Sciences and co-director of the Stanford Alzheimer’s Disease Research Center at Stanford University in California, gained an understanding of aging that suggest intriguing possibilities for clinical laboratories.
In their study, published in Nature, titled, “Undulating Changes in Human Plasma Proteome Profiles Across the Lifespan,” the scientists stated that aging doesn’t happen in a consistent process over time, reported Science Alert.
The Stanford researchers also found that they can accurately
determine a person’s age based on the levels of certain proteins in his or her
blood.
Additionally, the study of proteomics may finally explain why blood from young people can have a rejuvenating effect on elderly people’s brains, noted Scientific American.
Each of these findings is important on its own, but taken
together, they may have interesting implications for pathologists who follow
the research. And medical laboratory leaders may find opportunities in mass
spectrometry in the near future, rather than decades from now.
Three Distinct Stages in Aging and Other Findings
The Stanford study found that aging appears to happen at
three distinct points in a person’s life—around the ages 34, 60, and 78—rather
than being a slow, steady process.
The researchers measured and compared levels of nearly 3,000
specific proteins in blood plasma taken from healthy people between the ages of
18 and 95 years. In the published study, the authors wrote, “This new approach
to the study of aging led to the identification of unexpected signatures and
pathways that might offer potential targets for age-related diseases.”
Along with the findings regarding the timeline for aging, the researchers found that about two-thirds of the proteins that change with age differ significantly between men and women. “This supports the idea that men and women age differently and highlights the need to include both sexes in clinical studies for a wide range of diseases,” noted a National Institutes of Health (NIH) report.
“We’ve known for a long time that measuring certain proteins in the blood can give you information about a person’s health status—lipoproteins for cardiovascular health, for example,” stated Wyss-Coray in the NIH report. “But it hasn’t been appreciated that so many different proteins’ levels—roughly a third of all the ones we looked at—change markedly with advancing age.”
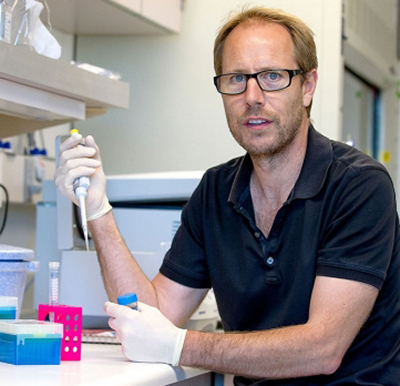
Tony Wyss-Coray, PhD (above), Professor of Neurology and Neurological Sciences at Stanford University, was senior author of the proteomics study that analyzed blood plasma from 4,263 people between the ages 18-95. “Proteins are the workhorses of the body’s constituent cells, and when their relative levels undergo substantial changes, it means you’ve changed, too,” he said in a Stanford Medicine news article. “Looking at thousands of them in plasma gives you a snapshot of what’s going on throughout the body.” (Photo copyright: Stanford University.)
Differentiating Aging from Disease
Previous research studies also found it is indeed possible
to measure a person’s age from his or her “proteomic signature.”
The researchers published their findings in Aging Cell, a peer-reviewed open-access journal of the Anatomical Society in the UK, titled, “Plasma Proteomic Signature of Age in Healthy Humans.” In it, the authors wrote, “Our results suggest that there are stereotypical biological changes that occur with aging that are reflected by circulating proteins.”
The fact that chronological age can be determined through a
person’s proteomic signature suggests researchers could separate aging from
various diseases. “Older age is the main risk factor for a myriad of chronic
diseases, and it is invariably associated with progressive loss of function in
multiple physiological systems,” wrote the researchers, adding, “A challenge in
the field is the need to differentiate between aging and diseases.”
Can Proteins Cause Aging?
Additionally, the Stanford study found that changes in protein levels might not simply be a characteristic of aging, but may actually cause it, a Stanford Medicine news article notes.
“Changes in the levels of numerous proteins that migrate
from the body’s tissues into circulating blood not only characterize, but quite
possibly cause, the phenomenon of aging,” Wyss-Coray said.
Can Proteins Accurately Predict Age? Not Always
There were, however, some instances where the protein levels inaccurately predicted a person’s age. Some of the samples the Stanford researchers used were from the LonGenity research study conducted by the Albert Einstein College of Medicine, which investigated “why some people enjoy extremely long life spans, with physical health and brain function far better than expected in the 9th and 10th decades of life,” the study’s website notes.
That study included a group of exceptionally long-lived Ashkenazi Jews, who have a “genetic proclivity toward exceptionally good health in what for most of us is advanced old age,” according to the Stanford Medicine news article.
“We had data on hand-grip strength and cognitive function
for that group of people. Those with stronger hand grips and better measured
cognition were estimated by our plasma-protein clock to be younger than they
actually were,” said Wyss-Coray. So, physical condition is a factor in
proteomics’ ability to accurately prediction age.
Although understanding the connections between protein in
the blood, aging, and disease is in early stages, it is clear additional
research is warranted. Not too long ago the idea of consumers having their DNA
sequenced from a home kit for fun seemed like fantasy.
However, after multiple FDA approvals, and the success of
companies like Ancestry, 23andMe, and the clinical laboratories that serve them,
the possibility that proteomics might go the same route does not seem so
far-fetched.
Experts list the top challenges facing widespread adoption of proteomics in the medical laboratory industry
Year-by-year, clinical
laboratories find new ways to use mass spectrometry to
analyze clinical specimens, producing results that may be more precise than
test results produced by other methodologies. This is particularly true in the
field of proteomics.
However, though mass spectrometry is highly accurate and
fast, taking only minutes to convert a specimen into a result, it is not fully
automated and requires skilled technologists to operate the instruments.
Thus, although the science of proteomics is advancing
quickly, the average pathology laboratory isn’t likely to be using mass
spectrometry tools any time soon. Nevertheless, medical
laboratory scientists are keenly interested in adapting mass spectrometry
to medical lab test technology for a growing number of assays.
Molly Campbell, Science Writer and Editor in Genomics, Proteomics, Metabolomics, and Biopharma at Technology Networks, asked proteomics experts “what, in their opinion, are the greatest challenges currently existing in proteomics, and how can we look to overcome them?” Here’s a synopsis of their answers:
Lack of High Throughput Impacts Commercialization
Proteomics isn’t as efficient as it needs to be to be
adopted at the commercial level. It’s not as efficient as its cousin genomics. For it to become
sufficiently efficient, manufacturers must be involved.
John Yates
III, PhD, Professor, Department of Molecular Medicine at Scripps Research California
campus, told Technology
Networks, “One of the complaints from funding agencies is that you can
sequence literally thousands of genomes very quickly, but you can’t do the same
in proteomics. There’s a push to try to increase the throughput of proteomics
so that we are more compatible with genomics.”
For that to happen, Yates says manufacturers need to
continue advancing the technology. Much of the research is happening at
universities and in the academic realm. But with commercialization comes
standardization and quality control.
“It’s always exciting when you go to ASMS [the conference for the American Society
for Mass Spectrometry] to see what instruments or technologies are going to be
introduced by manufacturers,” Yates said.
There are signs that commercialization isn’t far off. SomaLogic, a privately-owned American protein
biomarker discovery and clinical diagnostics company located in Boulder, Colo.,
has reached the commercialization stage for a proteomics assay platform called SomaScan. “We’ll be
able to supplant, in some cases, expensive diagnostic modalities simply from a
blood test,” Roy
Smythe, MD, CEO of SomaLogic, told Techonomy.
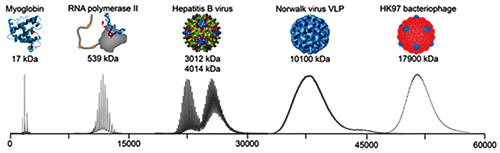
The graphic above illustrates the progression mass spectrometry took during its development, starting with small proteins (left) to supramolecular complexes of intact virus particles (center) and bacteriophages (right). Because of these developments, today’s medical laboratories have more assays that utilize mass spectrometry. (Photo copyright: Technology Networks/Heck laboratory, Utrecht University, the Netherlands.)
Achieving the Necessary Technical Skillset
One of the main reasons mass spectrometry is not more widely
used is that it requires technical skill that not many professionals possess.
“For a long time, MS-based proteomic analyses were technically demanding at
various levels, including sample processing, separation science, MS and the
analysis of the spectra with respect to sequence, abundance and
modification-states of peptides and proteins and false discovery rate
(FDR) considerations,” Ruedi
Aebersold, PhD, Professor of Systems Biology at the Institute of Molecular Systems Biology (IMSB) at
ETH Zurich, told Technology
Networks.
Aebersold goes on to say that he thinks this specific
challenge is nearing resolution. He says that, by removing the problem created
by the need for technical skill, those who study proteomics will be able to
“more strongly focus on creating interesting new biological or clinical
research questions and experimental design.”
Yates agrees. In a paper titled, “Recent Technical Advances in
Proteomics,” published in F1000 Research, a peer-reviewed open research
publishing platform for scientists, scholars, and clinicians, he wrote, “Mass
spectrometry is one of the key technologies of proteomics, and over the last
decade important technical advances in mass spectrometry have driven an
increased capability of proteomic discovery. In addition, new methods to
capture important biological information have been developed to take advantage
of improving proteomic tools.”
No High-Profile Projects to Stimulate Interest
Genomics had the Human Genome Project
(HGP), which sparked public interest and attracted significant funding. One of
the big challenges facing proteomics is that there are no similarly big,
imagination-stimulating projects. The work is important and will result in
advances that will be well-received, however, the field itself is complex and difficult
to explain.
Emanuel
Petricoin, PhD, is a professor and co-director of the Center for Applied
Proteomics and Molecular Medicine at George
Mason University. He told Technology
Networks, “the field itself hasn’t yet identified or grabbed onto a
specific ‘moon-shot’ project. For example, there will be no equivalent to the
human genome project, the proteomics field just doesn’t have that.”
He added, “The equipment needs to be in the background and
what you are doing with it needs to be in the foreground, as is what happened
in the genomics space. If it’s just about the machinery, then proteomics will
always be a ‘poor step-child’ to genomics.”
Democratizing Proteomics
Alexander
Makarov, PhD, is Director of Research in Life Sciences Mass Spectrometry
(MS) at Thermo Fisher
Scientific. He told Technology
Networks that as mass spectrometry grew into the industry we have today,
“each new development required larger and larger research and development teams
to match the increasing complexity of instruments and the skyrocketing
importance of software at all levels, from firmware to application. All this
extends the cycle time of each innovation and also forces [researchers] to
concentrate on solutions that address the most pressing needs of the scientific
community.”
Makarov describes this change as “the increasing democratization of MS,” and says that it “brings with it new requirements for instruments, such as far greater robustness and ease-of-use, which need to be balanced against some aspects of performance.”
One example of the increasing democratization of MS may be
several public proteomic datasets available to scientists. In European
Pharmaceutical Review, Juan
Antonio Viscaíno, PhD, Proteomics Team Leader at the European Bioinformatics Institute (EMBL-EBI)
wrote, “These datasets are increasingly reused for multiple applications, which
contribute to improving our understanding of cell biology through proteomics
data.”
Sparse Data and Difficulty Measuring It
Evangelia
Petsalaki, PhD, Group Leader EMBL-EBI, told Technology
Networks there are two related challenges in handling proteomic data.
First, the data is “very sparse” and second “[researchers] have trouble
measuring low abundance proteins.”
Petsalaki notes, “every time we take a measurement, we
sample different parts of the proteome or phosphoproteome and
we are usually missing low abundance players that are often the most important
ones, such as transcription
factors.” She added that in her group they take steps to mitigate those
problems.
“However, with the advances in MS technologies developed by
many companies and groups around the world … and other emerging technologies
that promise to allow ‘sequencing’ proteomes, analogous to genomes … I expect
that these will not be issues for very long.”
So, what does all this mean for clinical laboratories? At the
current pace of development, its likely assays based on proteomics could become
more common in the near future. And, if throughput and commercialization ever
match that of genomics, mass spectrometry and other proteomics tools could
become a standard technology for pathology laboratories.
Clinical laboratories working with AI should be aware of ethical challenges being pointed out by industry experts and legal authorities
Experts are voicing concerns that using artificial
intelligence (AI) in healthcare could present ethical challenges that need
to be addressed. They say databases and algorithms may introduce bias into the
diagnostic process, and that AI may not perform as intended, posing a potential
for patient harm.
If true, the issues raised by these experts would have major
implications for how clinical
laboratories and anatomic
pathology groups might use artificial intelligence. For that reason,
medical laboratory executives and pathologists should be aware of possible
drawbacks to the use of AI and machine-learning
algorithms in the diagnostic process.
Is AI Underperforming?
AI’s ability to improve diagnoses, precisely target
therapies, and leverage healthcare data is predicted to be a boon to precision medicine and personalized
healthcare.
For example, Accenture
(NYSE:ACN) says that hospitals will spend $6.6 billion on AI by 2021. This
represents an annual growth rate of 40%, according
to a report from the Dublin, Ireland-based consulting firm, which states,
“when combined, key clinical health AI applications can potentially create $150
billion in annual savings for the United States healthcare economy by 2026.”
But are healthcare providers too quick to adopt AI?
Accenture defines AI as a “constellation of technologies
from machine learning to natural
language processing that allows machines to sense, comprehend, act, and
learn.” However, some experts say AI is not performing as intended, and that it
introduces biases in healthcare worthy of investigation.
Keith Dreyer, DO, PhD, is Chief Data Science Officer at Partners Healthcare and Vice Chairman of Radiology at Massachusetts General Hospital (MGH). At a World Medical Innovation Forum on Artificial Intelligence covered by HealthITAnalytics, he said, “There are currently no measures to indicate that a result is biased or how much it might be biased. We need to explain the dataset these answers came from, how accurate we can expect them to be, where they work, and where they don’t work. When a number comes back, what does it really mean? What’s the difference between a seven and an eight or a two?” (Photo copyright: Healthcare in Europe.)
What Goes in Limits What Comes Out
Could machine learning lead to machine decision-making that
puts patients at risk? Some legal authorities say yes. Especially when computer
algorithms are based on limited data sources and questionable methods, lawyers
warn.
How can AI provide accurate medical insights for people when
the information going into databases is limited in the first place? Ossorio
pointed to lack of diversity in genomic
data. “There are still large groups of people for whom we have almost no
genomic data. This is another way in which the datasets that you might use to
train your algorithms are going to exclude certain groups of people
altogether,” she told HDM.
She also sounded the alarm about making decisions about
women’s health when data driving them are based on studies where women have
been “under-treated compared with men.”
“This leads to poor treatment, and that’s going to be
reflected in essentially all healthcare data that people are using when they
train their algorithms,” Ossorio said during a Machine Learning for Healthcare (MLHC) conference
covered by HDM.
How Bias Happens
Bias can enter healthcare data in three forms: by humans, by
design, and in its usage. That’s according to David Magnus, PhD, Director
of the Stanford Center for
Biomedical Ethics (SCBE) and Senior Author of a paper published in the New England
Journal of Medicine (NEJM) titled, “Implementing Machine
Learning in Health Care—Addressing Ethical Challenges.”
The paper’s authors wrote, “Physician-researchers are
predicting that familiarity with machine-learning tools for analyzing big data
will be a fundamental requirement for the next generation of physicians and
that algorithms might soon rival or replace physicians in fields that involve
close scrutiny of images, such as radiology and anatomical pathology.”
In a news
release, Magnus said, “You can easily imagine that the algorithms being
built into the healthcare system might be reflective of different, conflicting
interests. What if the algorithm is designed around the goal of making money?
What if different treatment decisions about patients are made depending on
insurance status or their ability to pay?”
In addition to the possibility of algorithm bias, the
authors of the NEJM paper have other concerns about AI affecting
healthcare providers:
“Physicians must adequately understand how
algorithms are created, critically assess the source of the data used to create
the statistical models designed to predict outcomes, understand how the models
function and guard against becoming overly dependent on them.
“Data gathered about patient health, diagnostics,
and outcomes become part of the ‘collective knowledge’ of published literature
and information collected by healthcare systems and might be used without
regard for clinical experience and the human aspect of patient care.
“Machine-learning-based clinical guidance may
introduce a third-party ‘actor’ into the physician-patient relationship, challenging
the dynamics of responsibility in the relationship and the expectation of
confidentiality.”
“We need to be cautious about caring for people based on what algorithms are showing us. The one thing people can do that machines can’t do is step aside from our ideas and evaluate them critically,” said Danton Char, MD, Lead Author and Assistant Professor of Anesthesiology, Perioperative, and Pain Medicine at Stanford, in the news release. “I think society has become very breathless in looking for quick answers,” he added. (Photo copyright: Stanford Medicine.)
Acknowledge Healthcare’s Differences
Still, the Stanford researchers acknowledge that AI can
benefit patients. And that healthcare leaders can learn from other industries,
such as car companies, which have test driven AI.
“Artificial intelligence will be pervasive in healthcare in a
few years,” said
Nigam Shah, PhD, co-author of the NEJM paper and Associate Professor of Medicine at Stanford, in the news release. He added that healthcare leaders need to be aware of the “pitfalls” that have happened in other industries and be cognizant of data.
“Be careful about knowing the data from which you learn,” he
warned.
AI’s ultimate role in healthcare diagnostics is not yet fully
known. Nevertheless, it behooves clinical laboratory leaders and anatomic
pathologists who are considering using AI to address issues of quality and
accuracy of the lab data they are generating. And to be aware of potential
biases in the data collection process.
Researchers believe new findings about genetic changes in C. difficile are a sign that it is becoming more difficult to eradicate
Hospital infection control teams, microbiologists, and clinical laboratory professionals soon may be battling a strain of Clostridium difficile (C. difficile) that is even more resistant to disinfectants and other forms of infection control.
A WSI news release states the researchers “identified genetic changes in the newly-emerging species that allow it to thrive on the Western sugar-rich diet, evade common hospital disinfectants, and spread easily.”
Microbiologists and infectious disease doctors know full well that this means the battle to control HAIs is far from won.
“C. difficile is currently forming a new species with one group specialized to spread in hospital environments. This emerging species has existed for thousands of years, but this is the first time anyone has studied C. difficile genomics in this way to identify it. This particular [bacterium] was primed to take advantage of modern healthcare practices and human diets,” said Nitin Kumar, PhD (above), in the news release. (Photo copyright: Wellcome Sanger Institute.)
Genomic Study Finds New Species of Bacteria Thrive in
Western Hospitals
In the published paper, Nitin Kumar, PhD, Senior Bioinformatician at the Wellcome Sanger Institute and Joint First Author of the study, described a need to better understand the formation of the new bacterial species. To do so, the researchers first collected and cultured 906 strains of C. difficile from humans, animals, and the environment. Next, they sequenced each DNA strain. Then, they compared and analyzed all genomes.
The researchers found that “about 70% of the strain collected specifically from hospital patients shared many notable characteristics,” the New York Post (NYPost) reported.
Hospital medical laboratory leaders will be intrigued by the
researchers’ conclusion that C. difficile is dividing into two separate
species. The new type—dubbed C. difficile clade A—seems to be targeting
sugar-laden foods common in Western diets and easily spreads in hospital
environments, the study notes.
“It’s not uncommon for bacteria to evolve, but this time we actually see what factors are responsible for the evolution,” Kumar told Live Science.
New C. Difficile Loves Sugar, Spreads
Researchers found changes in the DNA and ability of the C.
difficile clade A to metabolize
simple sugars. Common hospital fare, such as “the pudding cups and instant
mashed potatoes that define hospital dining are prime targets for these strains”,
the NYPost explained.
Indeed, C. difficile clade A does have a sweet tooth. It was associated with infection in mice that were put on a sugary “Western” diet, according to the Daily Mail, which reported the researchers found that “tougher” spores enabled the bacteria to fight disinfectants and were, therefore, likely to spread in healthcare environments and among patients.
“The new C. difficile produces spores that are more
resistant and have increased sporulation
and host colonization capacity when glucose or fructose is available for
metabolism. Thus, we report the formation of an emerging C. difficile
species, selected for metabolizing simple dietary sugars and producing high
levels or resistant spores, that is adapted for healthcare-mediated
transmission,” the researchers wrote in Nature Genetics.
Bacteria Pose Risk to Patients
The findings about the new strains of C. difficile bacteria
now taking hold in provider settings are important because hospitalized
patients are among those likely to develop life-threatening diarrhea due to
infection. In particular, people being treated with antibiotics are vulnerable
to hospital-acquired infections, because the drugs eliminate normal gut
bacteria that control the spread of C. difficile bacteria, the
researchers explained.
According to the Centers for Disease Control and Prevention (CDC), C. difficile causes about a half-million infections in patients annually and 15,000 of those infections lead to deaths in the US each year.
New Hospital Foods and Disinfectants Needed
The WSI/LSHTM study suggests hospital representatives should
serve low-sugar diets to patients and purchase stronger disinfectants.
“We show that strains of C. difficile bacteria have continued to evolve in response to modern diets and healthcare systems and reveal that focusing on diet and looking for new disinfectants could help in the fight against this bacteria,” said Trevor Lawley, PhD, Senior Author and Group Leader of the Lawley Lab at the Wellcome Sanger Institute, in the news release.
Microbiologists, infectious disease physicians, and their
associates in nutrition and environmental services can help by understanding
and watching development of the new C. difficile species and offering
possible therapies and approaches toward prevention.
Meanwhile, clinical laboratories and microbiology labs will
want to keep up with research into these new forms of C. difficile, so
that they can identify the strains of this bacteria that are more resistant to
disinfectants and other infection control methods.
CRISPR-Cas9 connection to cancer prompts research to investigate different approaches to gene editing
Dark Daily has covered CRISPR-Cas9 many times in previous e-briefings. Since its discovery, CRISPR, or Clustered Regularly Interspaced Short Palindromic Repeats, has been at the root of astonishing breakthroughs in genetic research. It appears to fulfill precision medicine goals for patients with conditions caused by genetic mutations and has anatomic pathologists, along with the entire scientific world, abuzz with the possibilities such a tool could bring to diagnostic medicine.
All of this research has contributed to a deeper understanding of how cells function. However, as is often the case with new technologies, unforeseen and problematic questions also have arisen.
“Here we report significant on-target mutagenesis, such as large deletions and more complex genomic rearrangements at the targeted sites in mouse embryonic stem cells, mouse hematopoietic progenitors, and a human differentiated cell line,” wrote the authors in their introduction.
Another study, this one conducted by biomedical researches at Cambridge, Mass., and published in Nature, describes possible toxicity caused by Cas9.
“Our results indicate that Cas9 toxicity creates an obstacle to the high-throughput use of CRISPR-Cas9 for genome engineering and screening in hPSCs [human pluripotent stem cells]. Moreover, as hPSCs can acquire P53 mutations, cell replacement therapies using CRISPR-Cas9-enginereed hPSCs should proceed with caution, and such engineered hPSCs should be monitored for P53 function.”
Essentially what both groups of researchers found is that CRISPR-Cas9 cuts through the double helix of DNA, which the cell responds to as it would any injury. A gene called p53 then directs a cellular “first-aid kit” to the “injury” site that either initiates self-destruction of the cell or repairs the DNA.
Therefore, in some instances, CRISPR-Cas9 is inefficient because the repaired cells continue to function. And, the repair process involves the p53 gene. P53 mutations have been implicated in ovarian, colorectal, lung, pancreatic, stomach, liver, and breast cancers.
Though important, some experts are downplaying the significance of the findings.
Erik Sontheimer, PhD (above), Professor, RNA Therapeutics Institute, at the University of Massachusetts Medical School, told Scientific American that the two studies are important, but not show-stoppers. “This is something that bears paying attention to, but I don’t think it’s a deal-breaker,” he said. (Photo copyright: University of Massachusetts.)
“It’s something we need to pay attention to, especially as CRISPR expands to more diseases. We need to do the work and make sure edited cells returned to patients don’t become cancerous,” Sam Kulkarni, PhD, CEO of CRISPR Therapeutics, told Scientific American.
Both studies are preliminary. The implications, however, is in how genes that have become corrupted are used.
A team from the Salk Institute may have found a solution. They are investigating a different enzyme—Cas13d—which, in conjunction with CRISPR would target RNA rather than DNA. “DNA is constant, but what’s always changing are the RNA messages that are copied from the DNA. Being able to modulate those messages by directly controlling the RNA has important implications for influencing a cell’s fate,” Silvana Konermann, PhD, a Howard Hughes Medical Institute (HHMI) Hanna Gray Fellow and member of the research team at Salk, said in a news release.
The Salk team published their findings in the journal Cell. The paper describes how “scientists from the Salk Institute are reporting for the first time the detailed molecular structure of CRISPR-Cas13d, a promising enzyme for emerging RNA-editing technology. They were able to visualize the enzyme thanks to cryo-electron microscopy (cryo-EM), a cutting-edge technology that enables researchers to capture the structure of complex molecules in unprecedented detail.”
The researchers think that CRISPR-Cas13d may be a way to make the process of gene editing more effective and allow for new strategies to emerge. Much like how CRISPR-Cas9 led to research into recording a cell’s history and to tools like SHERLOCK (Specific High-sensitivity Enzymatic Reporter unLOCKing), a new diagnostic tool that works with CRISPR and changed clinical laboratory diagnostics in a foundational way.
Each discovery will lead to more branches of inquiry and, hopefully, someday it will be possible to cure conditions like sickle cell anemia, dementia, and cystic fibrosis. Given the high expectations that CRISPR and related technologies can eventually be used to treat patients, pathologists and medical laboratory professionals will want to stay informed about future developments.