Multiple recent studies reveal a substantial number of patients continue to delay needed healthcare in the months since the onset of the SARS-CoV-2 outbreak
Based on an analysis of hospital emergency department (ED) usage, federal researchers concluded that patients continue to be cautious when visiting healthcare providers, including clinical laboratories, and that people are altering how they seek and utilize emergency care due to the COVID-19 pandemic. This not only reduces the number of typical test orders from the ER to the hospital lab, but also reduces the source of inpatient admissions.
Between March 29 and April 25 of this year, facilities the CDC examined recorded 1.2 million visits to EDs, compared to 2.1 million visits between March 31 and April 27 of last year. The steepest decrease in patient demographics was for individuals under the age of 14, women, and people living in the Northeast region.
The CDC’s data showed that 12% of ED visits were for children in pre-pandemic 2019, which dropped to 6% during the 2020 pandemic period. The CDC included ED visits from hospitals in 47 states (excluding Hawaii, South Dakota, and Wyoming) and captured information from approximately 73% of ED visits in the US.
Delaying Healthcare Visits Worsens Medical Conditions, Reduces Revenues
ED visits are an important referral source for inpatient admissions. Fewer patients in EDs means lost revenue for hospitals. However, one positive aspect of the waning number of ED visits is that it may be keeping patients with non-emergency situations away from emergency departments, thus reducing the overuse of costly ED visits. But healthcare professionals are concerned that individuals also may be avoiding or delaying care when needed, which could worsen medical situations and outcomes.
“We saw people, with COVID-19 and without, coming into the ED who were very ill,” Vik Reddy, MD, Chief Medical Officer at Wellstar Kennestone Hospital and Wellstar Windy Hill Hospital in the Atlanta area, told Modern Healthcare. He noted that some patients delayed care for critical non-COVID-19 illnesses. “The good news is that we’re seeing that trend reverse this time around. It was scary in March when we knew that people weren’t coming into the ED for heart attacks.”
The NSSP’s analysis concluded that the report’s findings were subject to at least four limitations:
The number of hospitals reporting to NSSP changes over time as facilities are added or closed. For example, 3,173 hospitals reported data in April of 2019, while 3,467 reported data in April 2020.
Diagnostic categories rely on the use of specific codes, which were missing in 20% of the ED visits reported.
NSSP coverage is not uniform across or within all the participating states.
The analysis is limited only to ED visits and does not take into account patients who did not go to an ED, but instead received treatment in other healthcare environments, such as urgent care clinics.
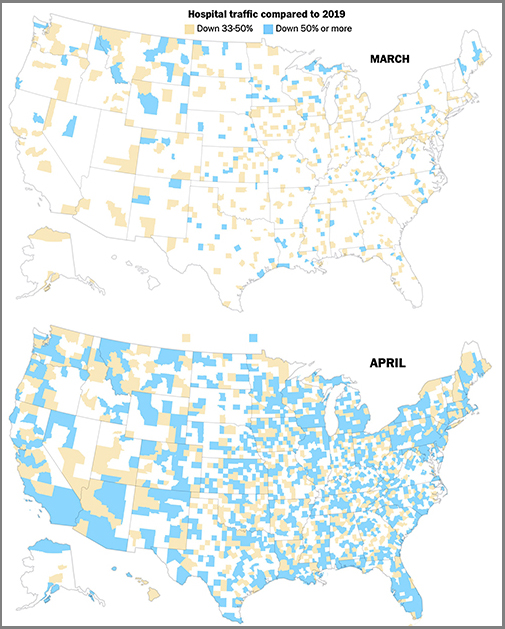
The graphics above are taken from a Washington Post article which reported that the newspaper’s analysis of smartphone location data of hospital traffic in 2020 showed the “drop” in hospital usage had turned into “a crash,” compared to the same two months last year, and that, “As in many other industries, those lost visits represented a widespread financial crisis for hospitals and other healthcare providers, even in places the novel coronavirus hardly touched.” (Graphics copyright: The Washington Post.)
Additional Studies Show Patients Avoiding Hospital EDs, Delaying Care
Other sources also are reporting similar findings regarding consumer attitudes towards seeking medical care during the COVID-19 pandemic. A PricewaterhouseCoopers survey released in May found that about 45% of 2,500 consumers surveyed plan to forgo their annual physical in 2020, due to the pandemic, Modern Healthcare reported.
In addition, an Optum Consumer Pulse Survey released in May found that nearly 20% of 700 surveyed individuals stated they were likely to avoid hospital EDs even if they were showing signs of a heart attack or appendicitis. Another 40% stated they were likely to avoid the ED if they had a cut that required stitches.
In “Americans Are Delaying Medical Care, and It’s Devastating Health-Care Providers,” The Washington Post analyzed hospital use during the pandemic based on smartphone tracking data. WaPo’s report found a significant drop in patients seeking in-person healthcare with many areas across the country reporting a 50% reduction in patients when compared to last year.
The article also states that almost 94 million people have delayed medical care due to the COVID-19 pandemic, and that 66 million of those individuals needed medical care unrelated to the virus but did not receive it.
These studies and others are showing a pattern. The COVID-19 pandemic has changed when and where patients access healthcare, and if the trend continues, it could have a long-term impact on clinical laboratories. Since fewer people are seeking medical care, fewer laboratory tests are being ordered and performed, which means less work and revenue for the nations’ hospital and independent clinical labs.
Meanwhile, some insurance payers are dropping coverage for certain medical treatments they consider “unnecessary,” leaving hospitals and their medical laboratories to wonder if they will be reimbursed for the tests they perform
Hospital-based medical laboratories and anatomic pathologists are well aware that the emergency department (ED) in their hospital is their single largest customer and that reporting test results within required turn-around times (TATs) is a non-stop battle. Thus, it will not be a surprise to learn that EDs provide nearly half of all hospital-related medical care in the US. That’s what a study by the University of Maryland School of Medicine (UMSOM) reports.
The UMSOM researchers claim their study, which was published in the International Journal for Health Services (IJHS), is the first ever to quantify the contribution EDs make to US healthcare. According to an UMSOM news release, they determined that 47.7% of all hospital-associated medical care between 1996 and 2010 was delivered by EDs.
Results Show EDs Critical to Healthcare Delivery
This a remarkable revelation. “I was stunned by the results,” David Marcozzi, MD, Associate Professor and Assistant Chief Medical Officer for Acute Care, UMSOM Department of Emergency Medicine, told Becker’s Hospital Review. Marcozzi led the study, which involved researchers from Thomas Jefferson University and other academic institutions.
“This research underscores the fact that emergency departments are critical to our nation’s healthcare delivery system,” he continued. “Patients seek care in emergency departments for many reasons. The data might suggest that emergency care provides the type of care that individuals actually want or need.”
As Becker’s Hospital Review explained, there were about 130-million visits to hospital EDs as compared to 101-million outpatient visits, and 39-million inpatient visits during 2010, the most recent year analyzed by UMSOM.
Quantifying the EDs Contribution to Healthcare
The researchers studied the role EDs play in caring for Americans, as compared to hospital outpatient and inpatient sectors. They were motivated, in part, by the apparent extra attention healthcare decision-makers pay to inpatient services and costs. As an emergency medicine and population health specialist, Marcozzi (who also works in the UM Medical Center Emergency Department) challenged that focal point.
In the first study to quantify the contribution of emergency department care to overall US healthcare, researchers at the University of Maryland School of Medicine (UMSOM) have found that nearly half of all US hospital-associated medical care is delivered by emergency departments. In this video, David Marcozzi, MD, MHS-CL, FACEP, talks about why this is happening and what the ramifications are for healthcare delivery in the US. Click on image above to view video. (Video and caption copyright: University of Maryland School of Medicine.)
The researchers cited National Center for Health Statistics data suggesting just 12% of ED encounters led to hospitalizations. This seems to counter claims of up to 50% of all healthcare being delivered in EDs. However, the researchers note that EDs also serve the uninsured and poor, many of whom are not admitted to the hospital.
“Traditional approaches to assessing the health of populations focus on the use of primary care and the delivery of care through patient-centered [medical] homes, managed care resources, and accountable care organizations. The use of EDs has not been given much consideration in these models,” the authors wrote in their paper.
ED Visits Jump Nearly 44% over 14 Years
Researchers analyzed ED patient, outpatient, and inpatient data from these sources:
National Hospital Ambulatory Medical Care Survey
National Hospital Discharge Survey
Electronic data files (sources of patient demographics and medical information) from commercial organizations, state data systems, hospitals, and hospital associations
They discovered that 3.5-billion healthcare encounters occurred over the 14-year period studied (1996 to 2010), representing a 43.7% increase in ED visits during that time.
During that period, ED utilization resulted in:
1.6-billion ED visits or 47.7%
1.3-billion outpatient visits or 37.6%
5.2-million hospital admissions or 14.8%
The UMSOM study also found EDs were increasingly being used by African Americans in the south and west and by Medicaid beneficiaries, Fierce Healthcare reported.
“When considering the isolated ED case mix, Medicaid as a course of payment showed a major increase in its contribution, shifting from 19.4% to 27.5% of all emergency care,” the researchers noted.
What’s needed, according to the study authors, are solutions to address non-urgent conditions often seen in EDs. However, they acknowledge, that the topic has drawn controversy.
Insurers Respond to Trend by Dropping Coverage of ‘Unnecessary’ ED Treatments
Some insurance companies on the hook for increasing ED costs have devised a novel approach to the increased cost—stop paying for it.
These new guidelines, which created quite a stir in Georgia before they went into effect July 1, 2017, are mirrored at BCBS affiliates in New York, Missouri, and Kentucky, noted sources in the Dark Daily report.
Non-avoidable Healthcare Events and ‘Connecting the Care’
“Despite a relentless campaign by the insurance industry to mislead policymakers and the public into believing that many ER visits are avoidable, the facts say otherwise,” stated Becky Parker, MD, President of the American College of Emergency Physicians (ACEP), in a news release.
UMSOM’s Marcozzi says the aim should be to “connect the care” delivered in EDs with other care offered by the healthcare system.
“Restricting EDs to patients classified as having critical illness does not seem a feasible or humanitarian option, as many individuals would not be able to find care elsewhere. In addition, many people do not have the knowledge to determine which symptoms indicate an emergency,” the researchers note.
Clinical Laboratories Can Download the UMSOM Full Study for Future Reference
At this point, it’s not clear how increasing ED costs and decreasing insurance payments will impact medical laboratories and anatomic pathology groups. Nevertheless, the UMSOM study is a good resource. ED volume and test orders will likely increase as more people go to EDs for treatment.
As a special to Dark Daily readers, Sage Publications is granting full access to UMSOM’s study through March 31, 2018. After that date, only the abstract will be available to non-IJHS subscribers. Click here to reach the full study article or place this URL into your browser: http://journals.sagepub.com/stoken/default+domain/JG8RNXfhAf7fuhFRIUIV/full.
Clinical laboratories and pathology groups that use taxicabs to pick up patient specimens and bring them to the lab now have the option of using Uber and Lyft for this service
For decades, medical laboratories have used taxicabs to have specimens picked up from one location and driven to the lab for testing. This was a way to handle STAT specimens, for example. Now, with the rise in popularity of ride-sharing services such as Uber and Lyft, a burgeoning trend has emerged where people utilize ride-services rather than driving themselves to the emergency room (ER) for medical treatment. Should clinical laboratories use ride-sharing services as well for transporting specimens?
Cost and Choice Two Advantages of Ride-sharing Services
According to the Center for Disease Control and Prevention (CDC), there are 130.4 million visits to ERs each year in the US and approximately 15% of those patients arrive by ambulance. But ambulance rides and EMT services can be costly.
According to howmuchisit.org, a website where visitors can find out how much average consumers paid for products and services around America, a trip to the ER by ambulance can range from $350 to $2,000 or more, depending on location, distance to the ER, and the patient’s insurance company.
Conversely, the cost for the same transportation by Uber or Lyft would typically cost less than $100.
So, price is one advantage ride-sharing services have over traditional ambulance rides. There are others. Patients also can choose which hospital they will be taken to for treatment. This option is generally not available via ambulance. Additionally, passengers know what the price of the trip with Uber or Lyft will be up front. Months can pass before patients receive a bill for a traditional ambulance ride.
But is it a good idea to call up Uber or Lyft instead of dialing 911 in a potentially life-threatening situation when moments count and emergency medical technician (EMT) skills can save lives?
To Uber or Not to Uber? That Is the Question
There are no statistics on the number of people who use ride-sharing services to go to the ER. However, many drivers in a chat room for Uber drivers acknowledged an escalation in the amount of requests for trips to the ER, usually for maladies such as broken bones, bleeding wounds, vomiting, or allergic reactions.
In a STAT article, Francis Piekut, who drives for both Uber and Lyft in Boston, described what he encountered when taking a call to transport a passenger to the ER. “They were burned and wanted to go the emergency room,” he stated. “I don’t know how bad it was, but I knew they were in pain really bad.” He took the individual where they wanted to go, as he would any other fare.
“I didn’t mind it,” Piekut added. “I was already there, and I know the ambulance costs a lot.”
However, other drivers in the chat room indicated they had or would refuse such service requests due to:
Liability issues;
Fear of getting blood or vomit in their car;
Knowing that they could not speed through the streets like an ambulance during an emergency; and
Apprehension about being stuck with a dead body if the passenger perished on the way to the ER.
Officially, Uber and Lyft recommend that people call 911 in the event of an emergency. In an ABC News article, Uber stated: “We’re grateful our service has helped people get to where they’re going when they need it most. However, it’s important to note that Uber is not a substitute for law enforcement or medical professionals. In the event of any medical emergency, we encourage people to call 911.”
The screen shot above taken from an NBC News TODAY video shows that some Uber drivers feel they are not required or prepared to substitute for an actual ride in an ambulance or EMT van. Click on the link above to watch the full video report. (Photo copyright: NBC News TODAY.)
Nevertheless, some emergency departments are looking at ride-sharing services to reduce their workload. Officials in Washington DC are researching the use of such services for “non-emergency, low-acuity” calls. These types of calls were responsible for nearly half of the city’s 911 calls in 2015, STAT reported.
“In our research, we found that many of these calls did not require an ambulance,” Doug Buchanan, Chief Communications Officer for the District of Columbia Fire and Emergency Medical Services (DC FEMS), noted in the STAT article. He believes it would be beneficial if people with non-emergencies used ride-hailing services instead of an ambulance. “We would love our residents to take that initiative,” he stated.
Baltimore ER physician Mark Plaster, MD, believes there should be multiple transportation options available to patients to accommodate different types and intensities of injuries.
“I would hope that no one who needed truly urgent medical attention would take an Uber,” Plaster urged in the STAT article. “If you need medical care en route, a private car is a bad idea, because you won’t have the personnel or equipment to treat you.”
Nevertheless, Plaster can see some merit in using ride-sharing services to get to the ER.
“Rideshares don’t take ambulances out of service, and not everybody coming into the ER is in a dire situation,” he stated in the STAT article. “And the ambulance can be expensive.”
Clinical Laboratories Use Taxis to Transport Specimens
Ride-sharing services were originally established to improve on the cost and availability of taxicab services. Apparently, their faster service versus a traditional taxicab also makes them a desirable option for some individuals who need to get to an ER. But before you call Uber or Lyft to go to the ER, know that they are not prepared for true emergencies and your life could be on the line.
Clinical laboratories and pathology groups, on the other hand, have been using taxicabs for the delivery of lab specimens for decades. It is likely, then, that services like Uber and Lyft will soon be used for the transportation of lab test specimens, as well, and will continue to be utilized into the future.
Clinical laboratory managers are often part of the ER’s process improvement team
Hospital emergency rooms (ER) across the country are intensifying their focus on improving patient safety and reducing errors. The cost of malpractice lawsuits filed after errors in emergency rooms is a major reason why growing numbers of hospitals are initiating formal programs to identify and eliminate the source of errors and wrong care provided to patients.
It probably won’t surprise most pathologists and clinical laboratory managers to learn that diagnostic errors are one significant source of malpractice claims that result from care provided by hospital emergency rooms, which can often be chaotic and overcrowded. Recently, The Wall Street Journal reported that a large percentage of medical errors in hospitals—and the resulting malpractice suits—occur because of mistakes in the emergency room. Studies of closed claims show that 37% to 55% of the malpractice suits are attributable to diagnostic errors. (more…)