It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
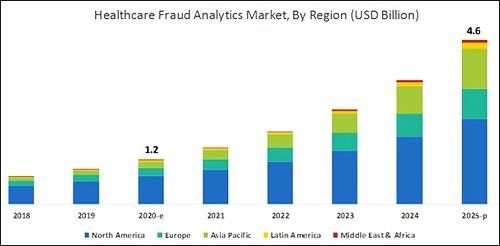
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.
Book provides detailed road map for clinical laboratory professionals who believe they have a valid case to file under the federal qui tam statute, as well as lab owners who want to understand what motivates whistleblowers and what practices to avoid
Several high-profile whistleblower cases uncovering massive fraud have shocked the clinical laboratory industry over the past decade. Media coverage nearly always focuses on the court battle and subsequent renderings of justice. But little is written about what it is like to be a whistleblower who wants to hold a medical laboratory accountable for alleged violations of federal and state laws.
Now, a new “tell-all” book penned by Chris Riedel, a whistleblower who owned a clinical laboratory company in California, details the exploits of clinical laboratory whistleblowers over the past 15 years. The intriguing white-collar crime thriller, titled, “Blood Money: One Man’s Bare-Knuckle Fight to Protect Taxpayers from Medical Fraud,” outlines Riedel’s battle with major clinical laboratory players—including the so-called “Blood Brothers” Labcorp (NYSE:LH) and Quest Diagnostics (NYSE:DGX)—to expose medical laboratory fraud.
‘Most Whistleblowers Get Absolutely Destroyed’
The book takes the reader on a gripping journey into extortion, money laundering, attempted murder, buried gold in a CEO’s backyard, fraudsters hiding money in the Cayman Islands, and, according to the author, an Assistant Attorney General sabotaging her own state’s case and a corrupt state Governor who undermined litigation by his own Attorney General.
“I wrote it to be a true crime thriller, so I’m hoping people who love thrillers will enjoy it as a true crime story,” Riedel said in an exclusive interview with Dark Daily. “For anyone who’s considering filing a whistleblower lawsuit, this is an absolute must read.
“Most whistleblowers get absolutely destroyed,” he explained. “When companies find out who’s trying to attack their business model, they do everything they can to destroy the whistleblower’s life. Many end up bankrupt, unemployable, and divorced.
“There are things you can do to protect yourself and I list those in my rules for whistleblowers. I hope enough people will read it—particularly in Congress and maybe the Department of Justice (DOJ)—to put pressure on the DOJ to change their behavior. They are far too willing to accept what they call ‘affordable civil settlements’ as opposed to punishing companies and people for their theft,” Riedel said.
Chris Riedel (above) has worked in the healthcare industry as an executive and an entrepreneur for more than 40 years. He founded five companies, including two medical laboratories and a cardiovascular disease management company. For the past 15 years, he has been tirelessly working to fight against medical companies that are defrauding US taxpayers. His actions have resulted in a court verdict and settlements totaling more than $550 million. (Photo copyright: Leadership Books.)
Riedel became a whistleblower in 2005 when he filed a case under California law that was sealed until 2009. Jerry Brown, California Attorney General at that time, joined the case and unsealed it.
Riedel had acted after his sales representatives informed him that his company, Hunter Laboratories, needed to come up with a way to compete against larger labs’ pricing to survive. Knowing the test-price-discounting practices transpiring within the lab industry in California, Riedel determined he had three choices:
Violate federal and state laws to compete,
Close his business, which would cause him to lay off more than 150 employees and lose most of his life’s savings, or
Try to stop the other companies from participating in fraudulent practices.
“It is very frustrating for honest CEOs of clinical labs to see that they cannot compete well against those lab companies employing fraudulent schemes. Rather than compete on the quality of service of their products as honest companies do, fraudsters compete based on the value of their illegal inducements,” he states on his website. “I felt the pain that many other honest CEO’s and lab owners have had to endure as they try to compete with fraud and watch their life’s work destroyed.”
He chose to try leveling the playing field for all labs and stop taxpayers from being fleeced. After filing that first whistleblower lawsuit in California in 2005, he later filed similar whistleblower lawsuits in other states that had statutes defining how labs were to price lab tests for their Medicaid programs.
Riedel encountered many roadblocks and frustrations during the initial lawsuit, including some genuinely frightening moments. He described one such experience for Dark Daily.
“Quest and Labcorp together went to Blue Shield of California, a major insurance company, and they got our clinical lab kicked out of network. They offered Blue Shield a 10% discount on all their laboratory testing if they would kick Hunter Laboratories out of network,” Riedel explained. “Since [Quest and Labcorp] represented about 70% to 80% of the total outpatient laboratory testing for Blue Shield, it was too good for this insurer to pass up.
“When your lab loses a major insurance carrier like that, you can’t survive. What doctor is going to want to start with a clinical lab that doesn’t have Blue Shield? And existing clients don’t want to subject their patients to having much higher out-of-pocket expenses.
“From that point on, it was like a dagger in our heart,” he added. “We were literally two weeks away from both corporate and personal bankruptcy when we reached our historic settlement with Quest. Had it not been for that settlement, our 150 employees would have lost their jobs, we would have lost our house, and we would have been completely bankrupt. That was very scary, and I had a very hard time dealing with it.”
Uncovering Medical Laboratory Fraud
While performing his research for the whistleblower case, Riedel was astonished by the information and fraud he discovered.
“There was one point where we had to prove that Quest and Labcorp were passing out discounts to some clients that were at or below cost, without giving those same prices to the Medi-Cal program, as required by state law at that time,” Riedel explained. “I personally reviewed over a million documents. It took more than five years, but it was worth it.
“I eventually found three documents that exposed the complete fraud by Quest. These documents showed what Quest had billed Medi-Cal, how much money the company lost client billing and capitation contracts, and how much business they ‘pulled through’ from the government and insurance payers that made up for the staggering losses on deeply discounted client and capitated billing. That was like the silver bullet.”
In the process, Riedel also discovered what it was like to work with the federal Department of Justice.
“The DOJ hates people who file more than one whistleblower lawsuit,” he added. “They don’t like the statute to begin with, and they barely tolerate whistleblowers, so when they find someone who does it time and again, they really don’t like it.”
“Blood Money” (above) contains practical advice and suggestions that are useful for both clinical laboratory executives and pathologists who want to keep their lab operations compliant with federal law, thus not giving whistleblowers any issues to pursue a qui tam lawsuit, as well as lab whistleblowers who observe violations within their clinical labs—or at competing labs—and who want to do something that may rectify the situation. (Photo copyright: Chris Riedel.)
Riedel is considering writing a second book and is trying to decide which qui tam lawsuits will provide the best subject matter.
“I am currently investigating what would be a multi-billion-dollar lawsuit against an insurance company and that is going to be, by far, the biggest of the cases I have ever been involved in. That might make a good book all by itself,” he said.
Riedel finds his work fighting fraud against the government rewarding and plans to continue his efforts in the future.
“Even though it’s risky—and the book details how my life was almost destroyed when the Blood Brothers counter attacked—I enjoy the investigative work and legal challenges. For me, it is very fulfilling, and I am proud to carry the torch for taxpayers,” he says in a statement on his website.
The 368-page book should be of interest to clinical laboratory personnel, healthcare professionals, those considering becoming a whistleblower, and basically anyone involved in medical laboratory testing.
This fourth edition of the annual event will be held virtually with free registration for pathologists and clinical laboratory professionals
In its fourth year, stakeholders in the clinical laboratory community have promoted thought leadership around the Lab Industry at the Project Santa Fe Foundation’s Clinical Lab 2.0 Workshop. Clinical Lab 2.0 (CL 2.0) which identifies new opportunities for medical labs to add value as the healthcare industry transitions from fee-for-service to value-based delivery models. But how does this concept apply during the era of COVID-19? That’s a key question participants will discuss at the 2020 Clinical Lab 2.0 Workshop, a virtual event scheduled for Oct. 26-27 with a focus on Population Health.
“This workshop will help all clinical laboratory leaders and pathologists to better understand, ‘How do we manage a pandemic, identifying high risk pool, where are the care gaps, and how do we better manage in the future proactively?’” said Khosrow Shotorbani, MBA, MT (ASCP), co-founder of the CL2.0 initiative and a regular speaker at the Executive War College, in an exclusive interview with Dark Daily. He is President and Executive Director of the Project Santa Fe Foundation, the organization that promotes the Clinical 2.0 Movement.
The coronavirus pandemic has “truly elevated the value of the clinical laboratory and diagnostics as one essential component of the care continuum,” he noted. “The value of the SARS-CoV-2 test became immense, globally, and the mantra became ‘test to trace to treat.’”
Project Santa Fe Foundation’s website defines Clinical Laboratory 2.0 as an effort to demonstrate “the power of longitudinal clinical lab data to proactively augment population health in a value-based healthcare environment.” The “goals are to improve the clinical outcomes of populations, help manage population risk, and reduce the overall cost of delivering healthcare,” the CL 2.0 website states.
“It’s about harnessing lab test results and other data that have predictive value and can help us proactively identify individuals that need care,” explained Shotorbani. “In the context of population health or value-based care, our labs potentially can utilize the power of this data to risk-stratify a population for which we are responsible or we can identify gaps in care.”
Clinical Lab 2.0 and the SARS-CoV-2 Pandemic
In the context of COVID-19, “Clinical Lab 2.0 argues that there is a hidden universe of value that can help augment what happens between COVID-19 testing and COVID-19 tracing to convert this reactive approach—meaning we wait for the person to get ill—versus considering who may be most at risk if they were to become infected so that our clinical laboratories can help caregivers create proactive isolation or quarantine strategies,” he added.
Shotorbani then explained how clinical laboratories have data about comorbidities such as diabetes, asthma, heart disease, and immunosuppression that are associated with more serious cases of COVID-19. “This clinical lab data can be harnessed, associated with demographic and risk data such as age and zip codes to help physicians and others identify patients who would be most at risk from a COVID-19 infection,” he noted.
“Historically, the primary focus of a clinical laboratory was very much on the clinical intervention, contacting the care manager physician, and identifying who’s at risk,” he said. But with COVID-19, Shotorbani sees opportunities to forge relationships with public health specialists to encourage what he describes as “consumer engagement.”
“As medical laboratory professionals, we must evolve to accommodate and support the needs of consumers as they take a more active role in their health,” he continued. “This is moving past simply providing lab test results, but to then be a useful diagnostic and therapeutic resource that helps consumers understand their health conditions and what the best next steps are to manage those conditions.”
Khosrow Shotorbani (above) is President, Executive Director, of the Project Santa Fe Foundation and one of the leaders of the Clinical Laboratory 2.0 movement. He is hopeful that the prominent role of medical laboratories in responding to the coronavirus pandemic will lead to an ongoing “seat at the table” in the higher echelons of healthcare organizations. In normal times, “we reside in basements, and we’re done when we release a result,” he said during an exclusive interview with Dark Daily. “COVID-19 was a kick in the rear to get us upstairs to the C-suite, because healthcare CEOs are under the gun to demonstrate more SARS-CoV-2 testing capacity.” Looking ahead, “we want to make sure that our clinical laboratories stay in that seat and design a future delivery model above and beyond COVID-19, maybe even help health systems, hospitals, and other providers drive their strategies.” (Photo copyright: Albuquerque Business First.)
“None of these are pathologists or come from the lab,” Shotorbani said. “They represent the C-suite and higher organization constituents. These are the healthcare executives who are dealing with their organization’s pain points. As clinical labs, we want to align ourselves to those organizational objectives.”
Pathologist Mark Fung, MD, PhD, will then present a CL 2.0 model for managing COVID-19 or other infectious disease pandemics, followed by a response from the other panelists. Fung is Vice Chair for Population Health in the Department of Pathology and Laboratory Medicine at the Larner College of Medicine at the University of Vermont. He is also on the Project Santa Fe Foundation (PSFF) board of directors.
“Lab 2.0 is a thought leadership organization,” Shotorbani said. “We are developing a template and abstract of this model of clinical laboratory services that other labs can follow while applying some of their own intuition as they make it operational.”
Day Two to the CL 2.0 workshop will feature case studies from the Henry Ford Health System in Detroit and Geisinger Health in Danville, Pa., followed by a discussion with eight PSFF directors. Then, Beth Bailey of TriCore Reference Laboratories in Albuquerque, N.M., will preside over a crowdsourcing session with participation from audience members.
Free Registration for Clinical Laboratories
This will be the first Clinical Lab 2.0 Workshop to be held virtually and registration this year will be free for members of the clinical laboratory community, Shotorbani said. In the past “there has been a hefty tuition to get into this because it’s a very high-touch workshop, especially for senior leaders. But given the critical topic that we’re facing, we felt it was important to waive the cost.”
The Fourth Annual Clinical Lab 2.0 Workshop is partnering this year with the American Society for Clinical Pathology (ASCP), which will provide the software platform for hosting the event, he said. In addition to the live conference sessions, registrants will have access to prerecorded presentations from past workshops. Content will be viewable for six months following the event.
Register for this critical event by clicking here, or by placing this URL in your browser (https://projectsantafefoundation.regfox.com/clinical-lab-20-workshop).
A former officer of a Cigna contractor claims the insurer hatched a scheme to submit invalid diagnostic codes and filed the now-unsealed qui tam action in 2017
In a case that could provide a cautionary tale for clinical laboratories, a federal whistleblower lawsuit alleges that Cigna, through its HealthSpring subsidiary, “received billions in overpayments from the federal government” in a scheme involving the insurer’s Medicare Advantage plans. The Qui tam (whistleblower) lawsuit was filed by Robert A. Cutler, a former officer of Cigna contractor Texas Health Management LLC (THM), under the federal False Claims Act.
Cutler alleged that “Cigna-HealthSpring has knowingly defrauded the United States through an intentional and systematic pattern and practice of submitting to CMS invalid diagnosis codes derived from in-home health assessments.” He claimed this took place “from at least 2012 until at least 2017,” and likely thereafter.
Cigna has denied the allegations. “We are proud of our industry-leading Medicare Advantage program and the manner in which we conduct our business,” the insurer stated in an email to HealthPayerIntelligence. “We will vigorously defend Cigna against all unjustified allegations,” Cigna stated.
As the lawsuit explains, Medicare Advantage (MA) plans are administered by private insurers under Medicare Part C. “Rather than pay providers directly based on the medical services provided, Medicare Part C pays MA Organizations a monthly capitated rate for each covered beneficiary, and tasks the MA Plan with paying providers for services rendered to plan members,” the lawsuit states. “MA insurers are generally paid more for providing benefits to beneficiaries with higher-risk scores—generally older and sicker people—and less for beneficiaries with lower-risk scores, who tend to be younger and healthier.”
The lawsuit notes that CMS relies on information—specifically ICD codes—from the insurers to calculate the risk scores.
Cigna’s 360 Program as Described in Lawsuit
Cutler alleged that Cigna defrauded CMS through its “360 Program,” in which primary care providers (PCPs) were encouraged to perform enhanced annual wellness visits that included routine physical exams. He claimed that “Cigna-HealthSpring designed the program so that, in practice, the 360 assessment was a mere data-gathering exercise used to improperly record lucrative diagnoses to fraudulently raise risk scores and increase payments from CMS.”
Cigna-HealthSpring, he alleged in the court documents, offered PCPs financial bonuses to perform the 360 program exams, especially on patients deemed most likely to yield high-risk scores. However, many clinicians declined, so the insurer recruited third-party contract providers, including THM, to send nurse practitioners (NPs) or registered nurses (RNs) to the homes of MA plan members.
For each visit, the NPs and RNs were given health reports listing the beneficiary’s previous diagnoses. “Cigna-HealthSpring intended the document to serve as a ‘cheat-sheet’ list of conditions and diagnoses it expected 360 contractors to capture during the in-home visit,” Cutler alleges. “The list of diagnoses did not indicate the date they were reported or any other information concerning their status.”
During each visit, which typically lasted 30-60 minutes, “NPs and RNs relied primarily on the patient’s self-assessment, i.e., subjectively reported information, as well as current medications to the extent available and, during certain time periods and for certain plan members, limited [clinical] laboratory findings,” Cutler alleged.
NPs were expected to record 20 or more diagnoses per visit, he wrote, including diagnoses based on “weak links” involving medications. “For example, Cigna-HealthSpring encouraged contractors to record atrial fibrillation, deep vein thrombosis, and pulmonary embolus based on the presence of certain classes of anti-coagulation medications on members’ medication lists or in their homes,” he stated.
He also alleged that “Cigna-HealthSpring, in purposeful violation of CMS rules, designed its 360 form to force NPs to capture diagnoses that were uncertain, probable, or merely suspected.”
These diagnoses were subsequently submitted as risk-adjustment data to CMS, he alleged, adding up to “hundreds of thousands of false claims from its six contractors during the relevant period. Although the exact amount will be proven at trial, the United States has paid billions of dollars in improper, inflated payments to Defendants under the MA Plan as a result of this scheme.”
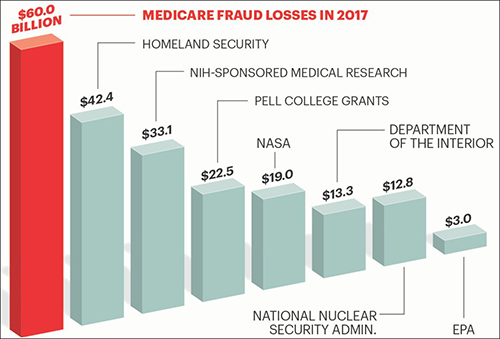
The graphic above is taken from an AARP article, titled, “Medicare Under Assault from Fraudsters,” which states, “The amount of tax dollars that are lost each year to Medicare fraud and waste is greater than the entire annual budget of some of the federal government’s most important programs and departments.” Clinical laboratories also are in danger of being drawn into the federal government’s fraud investigations which can be disruptive to business and revenues. (Graphic copyright: AARP.)
The Federal False Claims Act “allows a private citizen to step into the shoes of and pursue a claim on behalf of the government,” explained the Boyers Law Group of Coral Gables, Fla., in an article for HG.org, which states, the lawsuit “may proceed with or without the assistance of the government.”
If the government chooses to intervene, the whistleblower, known formally as the “relator,” can receive 15% to 25% of the proceeds recovered in the action, the law firm explained in another article for HG.org, adding that, in most cases, the government does not intervene, which increases the potential award to 30%.
In the Cigna case, the US Attorney’s office notified the court on Feb. 25, 2020, that the government had decided not to intervene “at this time.”
Significance for Clinical Laboratories
Regardless of how this case proceeds, medical laboratory managers should remember that they are subject to legal action if internal whistleblowers identify policies or procedures that violate federal fraud and abuse laws. And because it involves coding, it is also a reminder of the importance of documenting diagnoses and clinical laboratory test orders as protection against fraud allegations.
Another benefit of carefully documenting each lab test order is that labs can make the information available when auditors from government or private payers show up and want documentation on the medical necessity of each lab test claim.
Charges against this life science company executive include healthcare fraud as well as the first COVID-19 related securities fraud
In the first securities fraud prosecution involving clinical laboratory COVID-19 testing, the US federal Department of Justice (DOJ) charged the president of a Sunnyvale, Calif., life sciences biotechnology company with participating in a scheme to mislead investors and also to commit healthcare fraud, stated a DOJ press release.
The DOJ charged Mark Schena, PhD, president of Arrayit Corporation, with one count of securities fraud and one count of conspiracy to commit healthcare fraud related to submissions of more than $69 million in claims for allegedly unnecessary medical laboratory allergy and COVID-19 tests, the Associated Press (AP) reported.
“The defendant allegedly defrauded Medicare through illegal kickbacks and bribes, and then turned to exploiting the pandemic by fraudulently promoting an unproven COVID-19 test to the market,” said Brian Benczkowski, DOJ Assistant Attorney General, Criminal Division, in the DOJ press release.
According to the Washington Post, Arrayit allegedly bundled its finger-stick allergy test with the COVID-19 test kit.
Authorities Question Bundling of Tests, Claims
An affidavit in support of the criminal complaint stated that Arrayit was promoting “‘microarray technology’ for allergy and COVID-19 testing that allows for laboratory testing on a finger prick drop of blood that is placed on a paper card and sent by mail to Arrayit’s laboratory.”
The government’s investigation actually goes back two years to a time when Arrayit allegedly submitted or caused submission of $5.9 million in Medicare lab test claims and $63 million in lab test claims to private insurers through bribes and kickbacks, MedTech Dive reported.
The company’s clinical laboratory test for COVID-19 failed to receive US Food and Drug Administration Emergency Use Authorization (EUA), because it did not have the level of specificity and sensitivity required, MedTech Dive noted.
“Schena offered an Arrayit COVID-19 test in order to obtain Medicare beneficiary information that then was used to submit false and fraudulent claims for an unrelated and far more expensive allergy test for 120 allergens,” the DOJ complaint stated, adding, “Schena and others transmitted false and fraudulent e-mail communications and marketing materials about the Arrayit COVID-19 test and purported need to bundle the COVID-19 test with Arrayit’s allergy test, while never disclosing there were substantial questions about the accuracy of Arrayit’s COVID-19 test.”
Highlights of DOJ Charges
According to the DOJ press release:
Schena and others from 2018 through February allegedly “paid kickbacks and bribes” to recruiters and doctors to run a medical laboratory test for allergy screening (with 120 allergens) on patients “regardless of medical necessity and then make numerous misrepresentations to potential investors.”
News releases and social media promoted partnerships with companies and government agencies that either “did not exist” or were minor.
As the pandemic heated up, Arrayit representatives “made false claims concerning Arrayit’s ability to provide accurate, fast, reliable and cheap COVID-19 tests in compliance with state and federal regulations,” prosecutors said.
According to the DOJ’s complaint, Schena told investigators developing a test for COVID-19 was “like a pastry chef” who switches from selling “strawberry pies” to selling “rhubarb and strawberry pies.”
“The allure of cheap reliable alternatives to today’s standard blood tests panels has captured the imagination of the healthcare industry, making such alternatives a prime subject for fraudsters,” said David Anderson (above), US Attorney for the Northern District of California, in the DOJ press release, adding, “The scheme described in the complaint, in which the defendant allegedly leveraged this allure by appending the fear of the COVID-19 pandemic, amounts to a cynical multi-million-dollar hoax.” (Photo copyright: San Francisco Examiner.)
DOJ Prioritizing Coronavirus Fraud
US Attorney General William Barr earlier this year called for prioritization of investigation and prosecution of coronavirus fraud schemes, noted a DOJ statement, which pointed out that these types of fraud schemes leverage COVID-19 testing information generated by healthcare providers to fraudulently bill Medicare for other tests and procedures.
In April, Dark Daily’s sister publication, The Dark Report (TDR), covered one such kickback scheme in Georgia the DOJ was investigating. In that case, a Georgia man allegedly participated in a fraudulent kickback scheme in which clinical laboratory companies paid him on a per-test basis for referring cancer genetic, coronavirus, and respiratory pathogen panel tests to labs, TDR noted.
Clearly, the DOJ is stepping up its investigation into COVID-19 test fraud. Thus, medical laboratory leaders and pathologists should remain vigilant, as they are likely to observe more enforcement activity as the pandemic persists.